
Abstract
Introduction
Obesity is a chronic, multifaceted condition characterized by the accumulation of excess body fat, which can negatively impact health. The harmful effects of obesity are well-documented and among others include fertility issues (Hunter et al., 2021), an increased risk of type 2 diabetes and coronary artery disease (Piché et al., 2020), as well as certain types of cancer (Pati et al., 2023). However, the prevalence of obesity and consequently the associated economic burden is also increasing in the USA and the UK (Wang et al., 2011). Lifestyle interventions have been used to reduce excess body weight using a combination of methods such as diet, physical activity, behavior modification, and/or education (Cavero-Redondo et al., 2020; Lawlor et al., 2020; Salas-Salvadó et al., 2018). The majority of these studies are largely aimed at individuals living with overweight or obesity, seeking to identify the most effective ways to reduce excess weight. However, many health-related behaviors including eating or smoking are concordant in couples (Arden-Close and McGrath, 2017; Meyler et al., 2007) and research in Canadian adults has shown that following cohabitation, couples tend to mimic obesity risk (Katzmarzyk et al., 1999). Even though it is not clear exactly how social roles affect body weight, previous research concluded that changes in marital status like marriage or divorce can lead to gaining body weight (Teachman, 2016; Umberson et al., 2009). Additionally, a longitudinal national study in the USA with 10 years of follow-up, examined marital status and body weight in more than 9000 people and identified that those who were not married at baseline but married at follow-up had a greater increase in their weight compared to those who were married at both baseline and follow-up suggesting that change in social roles affect body weight (Sobal et al., 2003).
Interactions with family members affect the emotional well-being of a person (Martire and Schulz, 2007); consequently, the involvement of a close member of the family could enhance the results of a lifestyle intervention both for the individual and for the family member and tend to be more effective in maintaining health behavior changes in the long term (Burke et al., 2003). Indeed, a study exploring the barriers and facilitators of following a Mediterranean diet among women in the UK concurs that their partner's food choices affected their own eating behaviors (Kretowicz et al., 2018) which demonstrates the need to involve both members of the couple in weight management efforts. Additionally, a study of expectant couples in Sweden has shown that the odds of being overweight or obese increased relative to the partner's overweight or obesity (Edvardsson et al., 2013) which indicates that couples tend to share an obesity risk (Schierberl Scherr et al., 2013) and potential future weight loss interventions should focus on the couple rather than the individual. However, many lifestyle interventions have targeted only women, neglecting the home environment that affects eating behavior and choices (Gorin et al., 2017).
In research involving couples, there has been evidence of a ripple effect meaning that the partners who were not actively involved in a weight loss intervention, still lost some weight. For example, in a two-arm weight-loss pilot study involving Black men, researchers compared a behavioral intervention for those enrolled with their partners versus those participating alone. After 12 weeks, untreated women in the partner group lost 2.5 kg (compared to 0.2 kg in the standard group); although the difference was not statistically significant, it suggests a synergistic effect in weight loss efforts (Alick et al., 2018). Similar results were found in the study by Gorin et al. (2018) whereby there was weight loss in untreated partners but were not statistically significant between the intervention groups.
Even though there is evidence that couples’ interventions can be more supportive and successful compared to individuals’ interventions (Powers et al., 2022), it is not clear to what extent. Understanding this may inform the development of future interventions and public health policies targeted at this population. However, lifestyle interventions in couples are limited and those that exist have been using multiple study designs with different levels of couples’ involvement. For instance, some studies intervene equally on both members of the couple, others only on the primary participant, and others only on the primary participant's partner. Similarly, the intervention content differs among the studies which also contribute to the heterogeneity of the studies; however, they all employ a lifestyle intervention and focus on weight loss. Therefore, the aim of this systematic review of randomized controlled trials (RCTs) was to assess the effectiveness of lifestyle interventions targeting couples directly or indirectly as opposed to individuals or standard care, in terms of weight loss.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (Prisma) (Moher et al., 2010). The protocol for this systematic review was published in Prospero before the beginning of the study (Arvanitidou et al., 2019).
Search strategy and objective
The objective of the study was to identify studies that explore the use of lifestyle interventions on couples aiming to lose body weight.
The databases searched were MEDLINE Ovid, Scopus, CINHAL, and mySearch which are Bournemouth University's iteration of the EBSCO Discovery Service (EDS) tool. MySearch systematically searches several databases including Cochrane Review, Education Research Complete, PsychINFO, SocINDEX, Web of Science, CINHAL, and MEDLINE. The systematic search of the literature was conducted in March 2019 and repeated in April 2021 to ensure the search was updated. Limits on the date of publication were not set; the starting publication dates in the databases varied from 1698 to 1937 and the final search conducted was on 26th April 2021. Email alert service was set to all databases to identify eligible publications up until the preparation of final manuscript. Keywords used in the search strategy include ‘couple’, ‘intervention’, ‘weight management’, ‘diet change’, ‘body composition’ using Boolean operators. Subject headings were also searched using Medical Subject Heading (MESH) using the Medline EBSCOhost for the keywords: “lifestyle intervention” and “body composition”. Limiters applied were English language, full-text studies (no abstracts), and studies on human participants only.
Inclusion/exclusion criteria and outcomes
Eligible studies for this systematic review were randomized control trials (RCTs) that target couples, deliver a diet and lifestyle intervention compared to standard practice or no intervention, and aim to reduce body weight or Body Mass Index (BMI). The main outcomes of interest are weight and BMI while secondary outcomes include dietary intake and cardiovascular (CVD) biomarkers but are not presented in this research paper. Pharmacological interventions and studies that have delivered exclusively a physical activity intervention (without dietary advice) were excluded from this systematic review. The couple in this review was defined as partners in a romantic relationship regardless of marital status or sexual preference. Therefore, couples presented as parents-offspring, flat-mates, friends, etc. were excluded.
Study selection and data extraction
EndNote (Endnote X9, Thomson Reuters, New York, USA) was used to export all records from the database searches and remove duplicate records. Assessment for study eligibility commenced with titles and abstracts screening (twice by the first author and the second author randomly double-checked a sample), followed by full-text reading of potentially eligible studies. The studies that met all the criteria were discussed and agreed by all authors. The reference lists of the eligible studies were also checked to identify further eligible interventions.
Data from the eligible RCTs were extracted by two authors (EIA and IT) independently in duplicate. Data were extracted in an Excel spreadsheet and included comparisons between couples versus individuals’ interventions, and couples versus no interventions. Data extracted included study characteristics (first author's name, year of publication, country, setting, sample size, age, duration, medical condition if any), intervention-related variables (category of comparison per arm: intervention type and duration, primary and secondary outcomes), and intervention effects for both members of the couple, where available, (values of mean weight and standard deviations (SDs) of weight at baseline and at the first post-intervention assessment values). To ensure the independence between the studies, pilot studies that did not clearly state that their participants were different from their respective follow-up full-scale studies, were excluded. In case of missing data in the eligible papers, the authors were contacted to request them.
Quality assessment
The quality of the studies was assessed using the updated Critical Appraisal Skills Programme (CASP) for randomized controlled trials (CASP, 2023). Factors considered included assessing the research question in relation to methodology, randomization, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, equal treatment across intervention groups, effects and precision of the intervention, applicability, and benefits of the intervention. All authors assessed independently the eligible studies against these criteria.
Data synthesis and statistical analysis
To perform the meta-analysis, two datasets were constructed; the first dataset compared couples versus individuals’ interventions and the second dataset compared couples versus no intervention. To maximize the number of studies per comparison (some studies do not have both comparisons) and because these comparisons are independent of each other and each provides unique information, two meta-analyses were conducted based on each comparison (Borenstein et al., 2009).
For each data set mean weight, SD, and number of participants both at baseline and at the end of the intervention were recorded. When only 95% CI and SD were reported in the study, a proper transformation was carried out to calculate the weighted mean. Similarly, when the weight was reported in units other than kilograms, all values were transformed into kilograms. One author calculated and aggregated the final results (IT).
Meta-analysis
R (version 3.6.1) and RStudio (version 1.2.5001) meta package (version 4.9-9) were used to run the meta-analysis. Weighted mean difference (WMD) was used as a summary measure of weight of the difference in the means of the treatment group and the control group. The random effect model has been used for the meta-analysis as the included interventions vary in study characteristics and sample. In order to estimate the variance of the distribution of true effect sizes tau2 in the random-effect model, DerSimonian-Laird (DL) has been used. Both Higgin's and Thompson's I2 and tau2 are used to measure between-study heterogeneity. Outlier studies were detected by identifying which study's confidence interval did not overlap with the confidence interval of the pooled effect
Results
Study selection
The search strategy, following deduplication, resulted in 1508 papers that were title and abstract screened for eligibility. Seventeen studies met the inclusion criteria and 11 were included in the meta-analysis (Figure 1). All 17 studies are RCTs except the study by Matsuo et al. (2010) where participants chose the group they wanted to participate in to enhance compliance. Gorin et al. (2008) is an ancillary study to the multicentered RCT Look AHEAD (Action for Health in Diabetes) and the study by Schierberl Scherr et al. (2013), is a secondary analysis of the Lifestyle Eating and Activity Programme (LEAP) RCT (Gorin et al., 2013). Two pilot studies were eligible for this systematic review. The pilot study by Burke et al. (1999) is included in the meta-analysis because the authors clearly state that participants who took part in the pilot study were not included in the final publications (Burke et al., 2002, 2003). In the study by Trief et al. (2019), there is no clear statement to declare whether the participants of the pilot study (Trief et al., 2011) were excluded from their final analysis so it was excluded from this meta-analysis. The study by Dubbert and Wilson (1984) was excluded from the meta-analysis because the standard deviations (SD) were not reported in their results. The corresponding authors of the studies that measured but did not present weight and/or BMI data for participants and their partners were contacted but were unable to provide it and were excluded from this meta-analysis (Burke et al., 1999, 2002, 2003; Jensen et al., 2018; van Dijk et al., 2020; Voils et al., 2013); however, these studies remain of interest in terms of the intervention components and dietary data that will be reported in following publications.
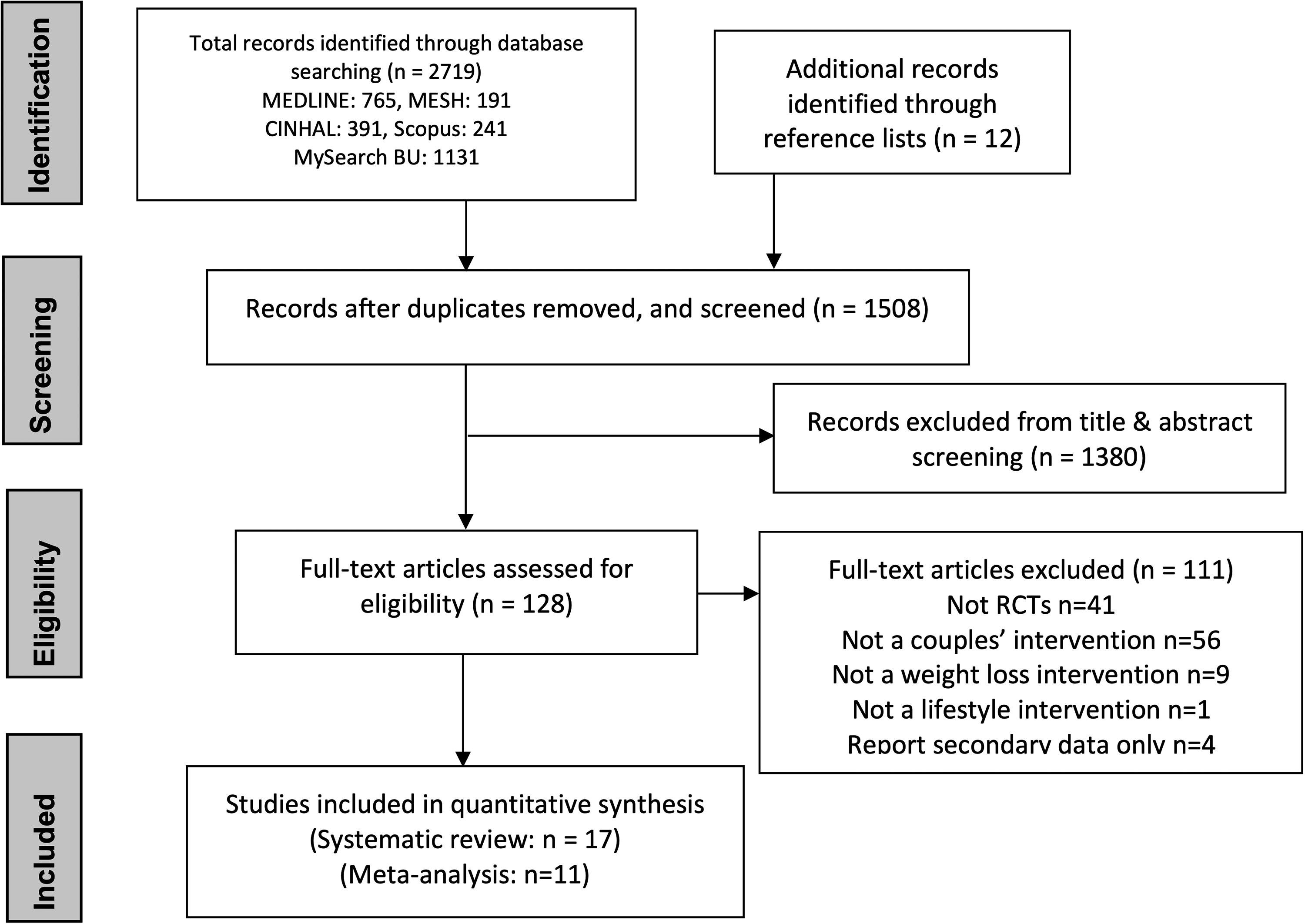
Study selection, PRISMA flow diagram.
Study characteristics
Duration
The included RCTs have a variety of duration and types of intervention. Study duration varies from 9 weeks to 18 months. Five studies had a short-time intervention from 9 weeks to 3 months (Black and Lantz, 1984; Israel and Saccone, 1979; Murphy et al., 1982; Pearce et al., 1981; Trief et al., 2011). Six studies had medium-term duration varying from 3,5 to 5 months (Burke et al., 1999, 2002; Dubbert and Wilson, 1984; Matsuo et al., 2010; Trief et al., 2016, 2019; Wing et al., 1991). Two studies had a longer intervention period, one for 1 year (Gorin et al., 2017) and the last one for 18 months (Schierberl Scherr et al., 2013); however, the data presented in their paper are for 6 months only.
Study population
The majority of studies included in the meta-analysis recruited middle-aged participants. The participants of six studies were over 50 years old; 4 studies recruited participants with mean ages between 35 to 41; one study did not report participants’ mean age and only the study by Burke et al. (2002) and its pilot (Burke et al., 1999) recruited young adults (Table 1).
Study characteristics of the eligible randomised control trials.
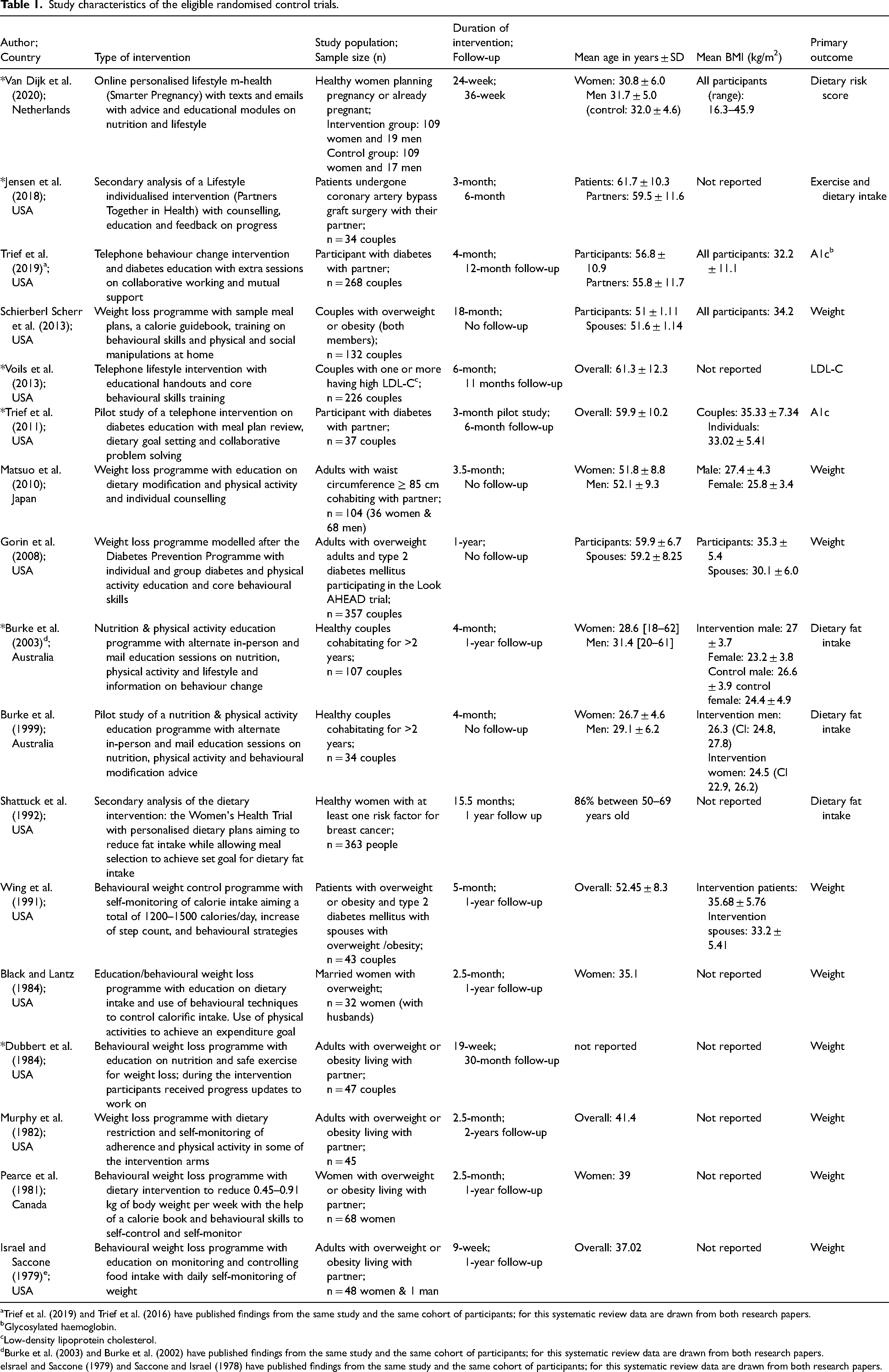
Trief et al. (2019) and Trief et al. (2016) have published findings from the same study and the same cohort of participants; for this systematic review data are drawn from both research papers.
Glycosylated haemoglobin.
Low-density lipoprotein cholesterol.
Burke et al. (2003) and Burke et al. (2002) have published findings from the same study and the same cohort of participants; for this systematic review data are drawn from both research papers.
Israel and Saccone (1979) and Saccone and Israel (1978) have published findings from the same study and the same cohort of participants; for this systematic review data are drawn from both research papers.
Intervention content
The dietary advice given varies and includes prescribing a generic hypocaloric diet (Black et al., 1984; Dubbert and Wilson, 1984; Matsuo et al., 2010; Murphy et al., 1982; Pearce et al., 1981) or using the principles of the Diabetes Prevention Programme (Gorin et al., 2008, 2013; Schierberl Scherr et al., 2013) or focusing on managing glycemic control (Trief et al., 2016, 2019). Other studies aimed to control specific macronutrients such as reducing dietary fat (Shattuck et al., 1992) and/or carbohydrates (Wing et al., 1991), or followed specific national dietary guidelines such as the Australian (Burke et al., 1999, 2002, 2003) while others do not present detailed information about the dietary plan (Saccone and Israel, 1978).
Types of intervention
All studies eligible for inclusion consisted of lifestyle interventions offering dietary advice to achieve calorie deficit and manage specific macronutrient intake such as dietary fat and targeting behavior change. Most studies offered physical activity advice as well (Black et al., 1984; Burke et al., 1999, 2003; Dubbert and Wilson, 1984; Gorin et al., 2008; Matsuo et al., 2010; Pearce et al., 1981; Schierberl Scherr et al., 2013; Wing et al., 1991). All studies focused on weight loss for participants with overweight or obesity (Black et al., 1984; Dubbert and Wilson, 1984; Israel and Saccone, 1979; Matsuo et al., 2010; Murphy et al., 1982; Pearce et al., 1981; Schierberl Scherr et al., 2013); or patients with type 2 diabetes (Gorin et al., 2008; Trief et al., 2011, 2016, 2019; Wing et al., 1991). Burke et al. (2003), and their pilot study (Burke et al., 1999) were the only studies that recruited healthy adult couples. The studies by Trief et al. (2019), Matsuo et al. (2010), Schierberl Scherr et al. (2013), Gorin et al. (2008), and Shattuck et al. (1992) have examined the effects of indirect interventions on untreated spouses supporting the evidence for the ripple effect.
All studies targeted behavior change but very few reported which theories or models of behavior change they used. Among the ones used are social learning theory (Bandura, 2004) used by Trief et al. (2016, 2019) and Dubbert and Wilson (1984). A combination of elements of theories such as the transtheoretical model (Prochaska and Velicer, 1997), Bandura's social cognitive theory(Bandura, 2004), and Fogg's behavior model (Fogg, 2009) were used in the study by van Dijk et al. (2020) and the rest of the studies used several behavioral theories and skills derived from social support theory including goal setting, stimulus-control or problem-solving.
Outcomes
Weight change
One study was detected as an outlier and removed from the meta-analysis (Matsuo et al., 2010) because it differed significantly from the overall effect. Following its removal, a forest plot was produced (Figure 2) to assess the effectiveness of couples’ interventions versus individual interventions. The estimated effect is −2.25 kg, and the 95% confidence interval stretches from −3.63 to −0.88 kg. Substantial heterogeneity is found between studies. The estimated effect of couples’ interventions versus control is −4.5 kg with 95% confidence interval from −6.62 to −2.38 kg (Figure 3) and moderate heterogeneity.
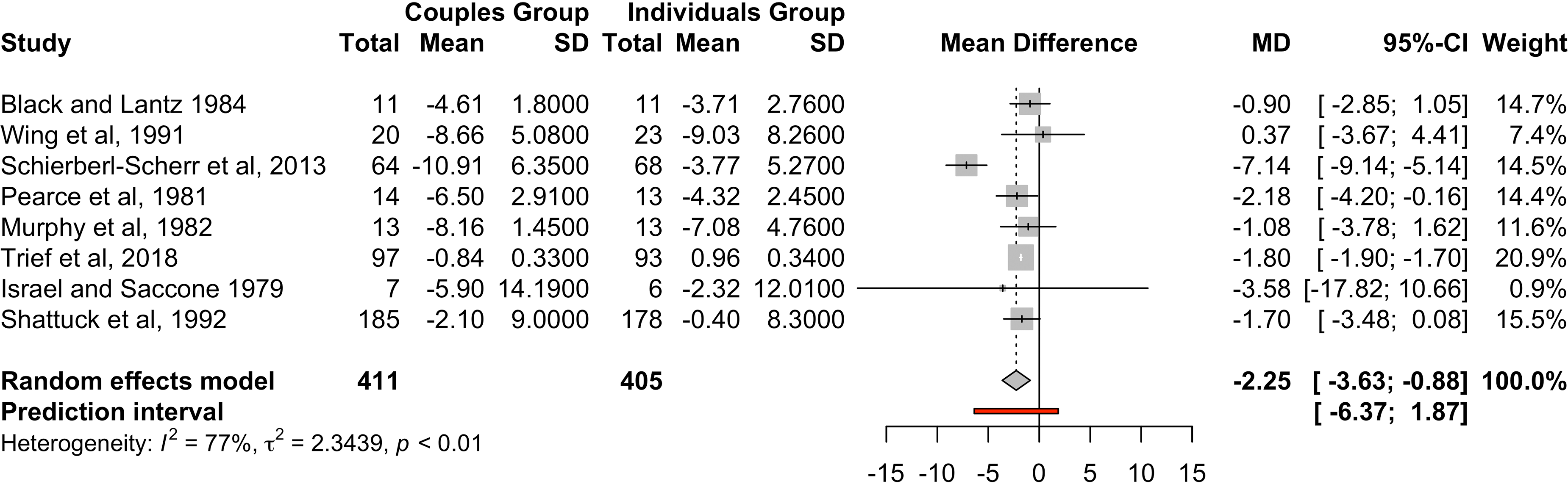
Change in weight by comparing couples’ intervention (direct or indirect) versus individual intervention.
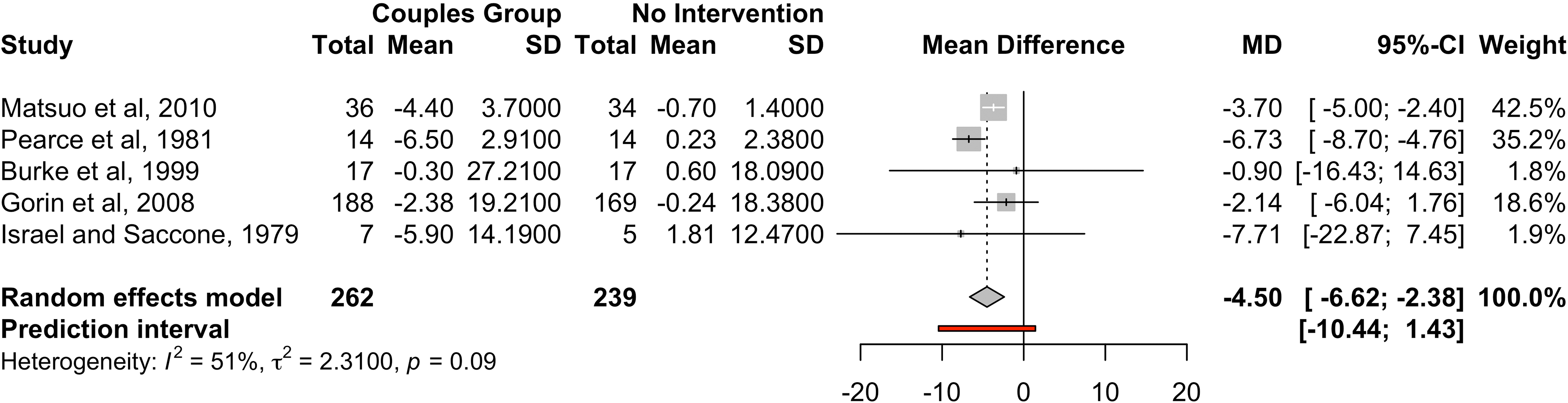
Change in weight by comparing couples’ intervention (direct or indirect) versus no intervention.
Body mass index
Three studies reported a change in BMI (Matsuo et al., 2010; Trief et al., 2016; Wing et al., 1991). Because of the small number of studies, a meta-analysis was not performed. Matsuo et al. (2010) investigated the effects of a lifestyle intervention on untreated spouses, by targeting their wives who were primarily the ones living with overweight or obesity (67%). Findings demonstrated a statistically significant reduction of BMI in untreated spouses of −1.5 ± 1.2 kg/m2 (CI: −1.9–1.1). Trief et al. (2016) conducted a telephonic intervention for patients with uncontrolled type 2 diabetes mellitus (mean age 57.8 ± 10.8 years old) and found a small but statistically significant reduction in BMI in the couples group (no change found in the individuals arm). The third study (Wing et al., 1991) is a 20-week weight-loss behavioral intervention targeting adults living with diabetes with both members of the couple being actively involved in the intervention versus only one member taking part. Both groups showed small and very similar statistically significant reductions in BMI in the patients with diabetes while the spouses who did not suffer from diabetes and were actively involved reduced their BMI more compared to the non-participating spouses.
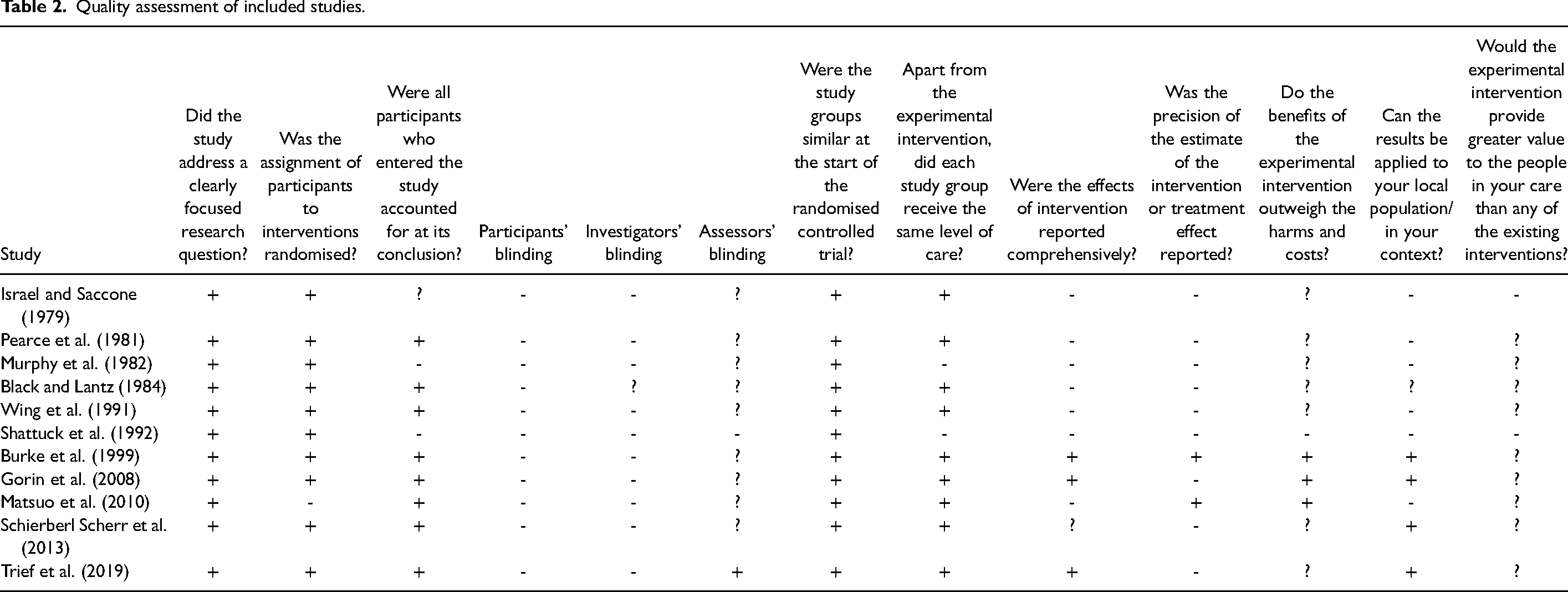
Risk of bias
Most studies were secondary analyses of previous bigger RCTs. Therefore, for the quality assessment, both the eligible study and its previous main study were considered (Table 2) independently by the paper's authors (EIA, JW, and FT). Analysis of the studies demonstrated that in terms of the study design, all studies were of good quality except the study by Matsuo et al. (2010) which was not randomized to increase participants’ adherence to the study. The methodology of the studies in terms of group similarity and equal treatment was good, but none of the participants or investigators were blinded, while only the studies by Trief et al. (2016, 2019) and Gorin et al. (2008) reported that those analyzing outcomes were blinded. The quality of results reporting was mixed with newer studies being of higher quality compared to older ones and only two studies (Burke et al., 1999; Gorin et al., 2008) reported treatment effects. The results of four studies (Burke et al., 1999; Gorin et al., 2008; Schierberl Scherr et al., 2013; Trief et al., 2019) could be applicable in the context of young couples in the UK but it is not clear whether these studies would add value to existing interventions. Four of the studies (Black et al., 1984; Israel and Saccone, 1979; Pearce et al., 1981; Saccone and Israel, 1978; Wing et al., 1991) required participants to deposit money (the amount varies from 11$ to 150$) to take part which would be returned gradually by attending training sessions or scheduled measurement sessions.
Quality assessment of included studies.
Publication bias
To assess for possible publication bias, a funnel plot was developed which consists of two axes [the y-axis shows the Standard Error (SE) and the x-axis shows the effect size of each study]. No asymmetry is found in the graph for the couples versus individuals (Figure 4) or for couples compared to no intervention (Figure 5), indicating no publication bias is found.
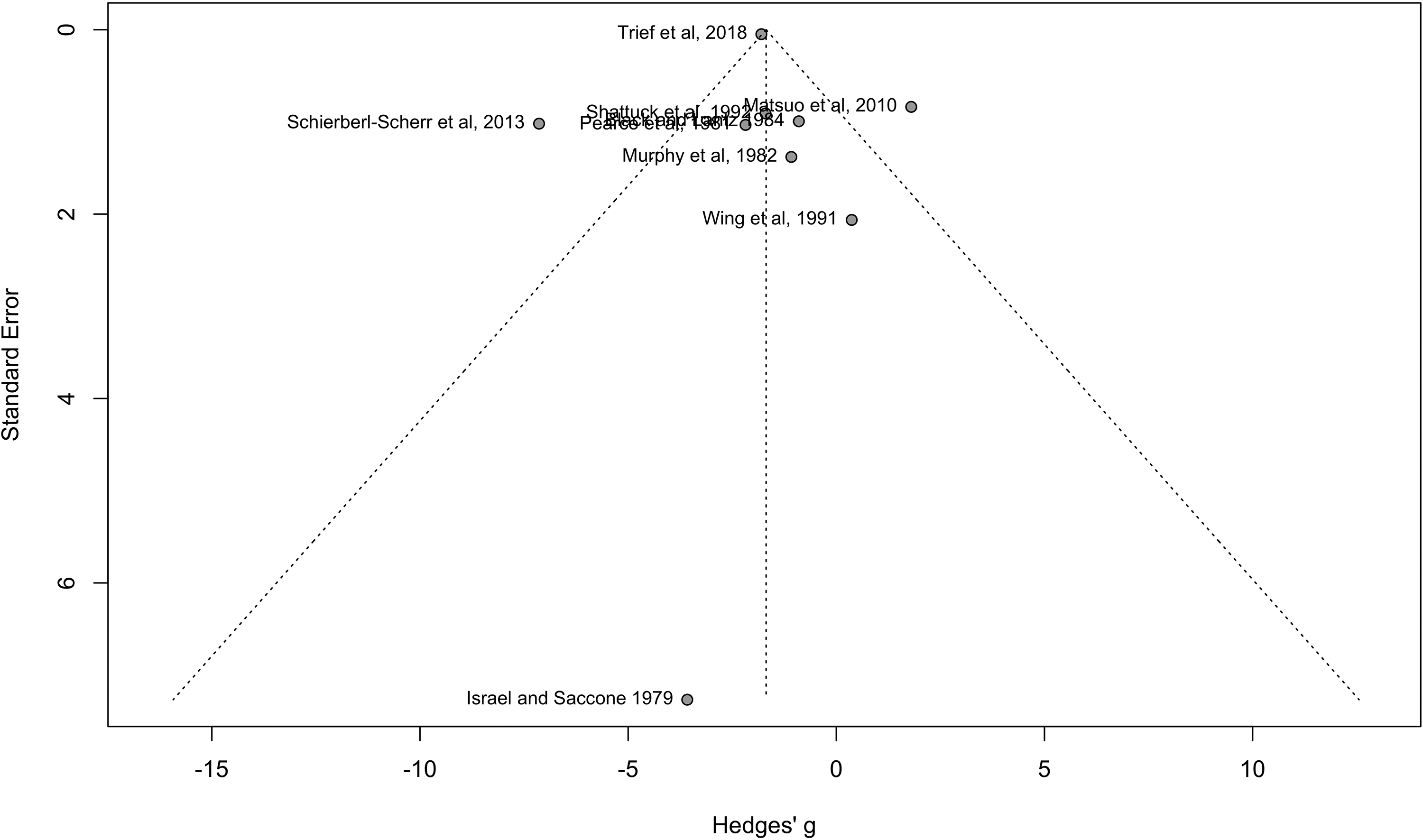
Funnel plot of studies of couples versus individuals.
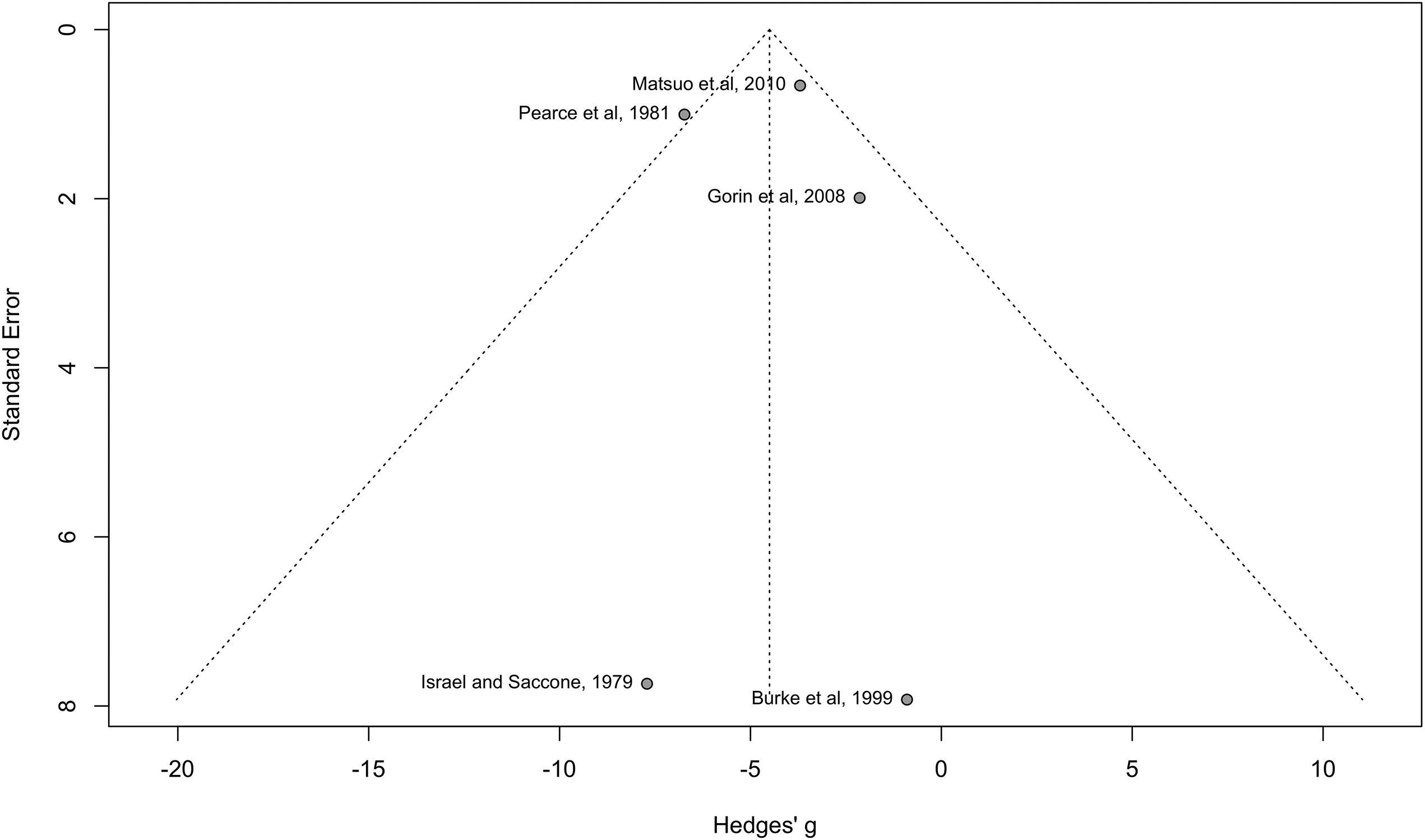
Funnel plot of studies of couples versus no intervention.
Discussion
This systematic review and meta-analysis identified RCTs that aimed to reduce the body weight of couples using lifestyle interventions. Findings suggest that targeting the couple can reduce body weight more in comparison to targeting individuals on their own. However, results should be interpreted carefully considering the significant variability of intervention content and the population differences.
Weight
The meta-analysis results demonstrate that targeting the couple rather than the individual is more effective in weight loss (WMD = −2.25 kg, 95% CI−3.63 to −0.88). Similarly, targeting the couple is more effective compared to standard care (WMD = −4.5 kg, 95% CI−6.62 to −2.38). In line with these results, a previous meta-analytic evaluation (Black et al., 1990) on behavioral weight loss programs comparing weight loss in couples or individuals working alone, found the couples’ programs more effective compared to the individual ones. A more recent systematic review (Arden-Close and McGrath, 2017) exploring health behavior change in couples (including obesity, diet, cancer prevention, physical activity, smoking in pregnancy, and multiple health behaviors) found mixed results. However, that systematic review focused on several health behaviors and consequently incorporated a great variation both in the populations and in study designs and interventions, not allowing for a meta-analysis to investigate the overall effect which highlights the need for more targeted research that could isolate the effects of couple dynamics on weight loss outcomes.
The findings of this meta-analysis support the effectiveness of lifestyle interventions targeting couples, suggesting that a shared behavioral change approach may enhance weight loss outcomes; however, given the broad prediction interval, which stretches well below zero, we cannot be overly confident that the positive effect we found for our interventions is robust in every context. Additionally, some studies investigated the ripple effect, where untreated partners showed weight loss despite not being actively involved in the intervention which suggests the potential for couple-based interventions to have broader impacts which has previously been shown in the family environment of adults living with overweight or obesity (Rossini et al., 2011). Previous research in couples has also demonstrated that interventions targeting health behavior change indirectly affect the untreated spouses (White et al., 1991; Zomeño et al., 2021). However, further exploration is needed to assess the mechanisms behind this phenomenon.
Body mass index
In this review, the three RCTs that assessed and reported BMI change from baseline to the end of the intervention found a small but statistically significant reduction in BMI in the couple groups (Matsuo et al., 2010; Trief et al., 2016; Wing et al., 1991). However, these findings should also be treated with caution considering the methodological flaws of the included studies. For example, one study had a small sample size (Wing et al., 1991) which potentially means that the study was underpowered and not generalizable; mean age was quite advanced in the study by Trief et al. (2016) but also age varied among all the studies; or allocation bias might have been introduced by not incorporating randomization in the study by Matsuo et al. (2010) (Paludan-Müller et al., 2016).
While BMI has advantages, such as ease of calculation and broad applicability in population studies, it also has significant limitations that can affect its reliability as an indicator of body composition. For instance, BMI cannot differentiate between lean mass and fat mass which is particularly pronounced in populations with high muscle mass, such as athletes (Prentice and Jebb, 2001); it does not differentiate between visceral or subcutaneous fat where the first is associated with increased health risks (Camhi et al., 2011); the relationship between BMI and body fat percentage is influenced by age, with older adults often having higher body fat levels at the same BMI compared to younger individuals (Di Renzo et al., 2022). Likewise, gender differences also play a role, as hormonal variations can affect fat distribution and body composition, further complicating the interpretation of BMI across sexes, while BMI may not be a reliable indicator of obesity in certain ethnic groups, as variations in body composition exist that are not accounted for by BMI alone (Camhi et al., 2011; Prentice and Jebb, 2001). Instead, body composition assessment can provide a better alternative for future interventions, recognizing that all assessment methods have their own advantages and disadvantages (Holmes and Racette, 2021; Prentice and Jebb, 2001). Finally, although researchers have not concluded what is the ideal intervention duration for a visible effect on BMI (Ahern et al., 2017; Brindal, 2017), a longer intervention duration can support behavioral change processes that can lead to a reduction in BMI (Samdal et al., 2017).
The beneficial effects of couples’ interventions on BMI shown in this study align with previous research, suggesting that spousal support in lifestyle interventions may lead to a positive combined effect compared to usual care, even if the results are not statistically significant (Alick et al., 2018). Another RCT targeting adults with type 2 diabetes and overweight or obesity, recruited an additional family member who also had overweight or obesity (but not type 2 diabetes) to participate in behavioral intervention; results showed there was a statistically significant reduction in BMI, although only 29% of pairs were partners or spouses (Samuel-Hodge et al., 2017). However, others have suggested that while partner involvement can increase health behavior change, benefits might only be temporary (Voils et al., 2020). This contradiction may stem from variations in intervention components, participant characteristics, and the nature of couple dynamics.
This review demonstrates that couples-based lifestyle interventions aiming to reduce body weight and BMI are limited with multiple differences in intervention designs. Nevertheless, they seem to have a small but significant effect on weight loss but less clear results on BMI. Similar results have been demonstrated by a recent systematic review that explored whether couples’ interventions are more effective than individual ones in reducing weight for metabolic syndrome prevention and potentially reducing the epigenetic risk of metabolic syndrome to couples’ offspring (Nizamani et al., 2022). The authors concluded that targeting couples for weight loss is at least as favorable as targeting individuals; however, statistically significant differences were not observed between couples and control groups.
Study characteristics
The duration of the interventions included in this study varies significantly and intervention studies with longer duration are needed to understand the long-term effects on weight loss. This variability poses challenges for synthesizing results and the heterogeneity in duration and intensity of the interventions complicates the generalizability of the results. A previous systematic review and meta-analysis of 80 weight loss interventions (including very low-energy diet; diet alone; meal replacement; diet and exercise; exercise alone; and pharmacotherapy) demonstrated a modest weight loss of 5–9% of their body weight within the first 6 months; the weight-loss plateaued at 6 months and stabilized to 4.8–8% loss at 1 year (Franz et al., 2007). Similar smaller but clinically meaningful weight loss reduction [−1.7 kg (−3.2–0.3)] is found for patients suffering from type 2 diabetes, according to a systematic review and meta-analysis of lifestyle and behavioral interventions that were used to develop 5 practice guidelines (Norris et al., 2005). A more recent systematic review and meta-analysis reported <5% total weight loss at one year without significant metabolic improvements that would be beneficial for patients with diabetes, suggesting the need for a longer duration of lifestyle interventions for these populations (Headland et al., 2016).
Types of interventions
All the studies included in this review offered dietary advice and training on behavior modification. Even though all studies aimed at weight loss, the dietary advice varied significantly making direct comparisons challenging, but the authors intend to explore the dietary component of the studies in a future paper.
Even though there is evidence to suggest that interventions developed and designed according to health behavior theories (HBT) have a strong theoretical basis, enhance understanding of the process of change and its determinants, and can be evaluated (Michie et al., 2008), the results on the effectiveness are inconsistent. For instance, a systematic review of nine systematic reviews aiming to explore the effectiveness of theory-based interventions against non-theory-based interventions found that the RCTs that used HBT were not more effective in behavior change including weight loss (Dalgetty et al., 2019). However, this might be explained by the fact that in some cases the full theory might not be implemented, and its missing components might be the ones that could have an effect (Michie and Prestwich, 2010) or in some cases the studies that stated they are not using a theory may in fact be guided by one (Prestwich et al., 2014).
Couple-based interventions have been effective in some health behavior outcomes such as BMI reduction (Trief et al., 2016) or physical activity (Voils et al., 2013) but it was found that only half of couple-based interventions achieved better results than individual-focused approaches (Arden-Close and McGrath, 2017). The mixed findings might be explained by the significant heterogeneity of studies. Further research is needed to understand in what contexts and with what components or intensities couples’ interventions may offer better outcomes compared to interventions on individuals (Gouin and Dymarski, 2024).
Study quality
All the studies that were eligible for this meta-analysis have methodological flaws and none of the studies is of very high quality (Table 2). The nature of the intervention does not allow for blinding of participants but blinding of the measurements’ assessors would be possible to reduce detection bias (Probst et al., 2016). Selection bias might have also been introduced in the study by Matsuo et al. (2010) which can risk internal validity (Armijo-Olivo et al., 2022).
In some studies, participants were required to pay for participation and they could receive their money back in installments if they were participating in pre-arranged sessions of the intervention. This practice potentially raises ethical concerns because according to current ethical regulatory frameworks, it could undermine the autonomy of choice or introduce social inequalities (London et al., 2012). It is also an example of potential sampling bias. Future lifestyle interventions should address the issue of having medium and low-quality studies to enable intervention development to produce meaningful results. Using a framework such as GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) could improve the evaluation of certainty of the evidence.
The absence of publication bias strengthens confidence in the review's findings (Henmi and Copas, 2010). However, the small number of included studies could limit the ability to detect subtle biases in combination with the significant heterogeneity calls for caution in results interpretation.
Strengths and limitations
To our knowledge, this is the first meta-analysis to examine the effect of interventions that focus on the couple rather than the individual, on weight loss. The total weight change between the baseline and the end of the intervention was analyzed. Methodologically this review is strong, because the systematic search of the evidence, the analysis, and the reporting of the findings have been performed according to the Prisma guidelines (Moher et al., 2010), the quality assessment according to CASP (CASP, 2023) and the data were extracted independently by two researchers.
A limitation of this meta-analysis is the wide heterogeneity between the RCTs included in this review with different populations (healthy, people with diabetes); a wide age range with primarily older participants (the majority of participants were older than 35 years old except for two studies (Burke et al., 1999, 2002, 2003) different intervention content (some but not all offer physical activity advice) and the dietary advice and/or plan is different in the studies. Also, the duration and follow-up of the intervention varied significantly, and for this reason, the weight changes between baseline to the first assessment after intervention were analyzed, but it would be interesting to analyze the weight change at follow-up. Additionally, some of the studies have a small sample size and might have been underpowered. For this review, only weight and BMI outcomes are reported but body composition outcomes could have been analyzed. Consequently, even though our results met statistical significance they should be treated with caution.
Even though according to this study targeting couples instead of individuals appears promising in terms of weight loss, there are only a few studies and future research is needed to better understand the effects of lifestyle interventions on couples. Important areas to be considered include addressing the challenges identified such as ensuring equal involvement of both members of the couple, use of a theoretical framework to underpin the development of the intervention, longer duration, involvement of younger participants, and better quality of study design.
Conclusions
Findings from this systematic review and meta-analysis suggest that lifestyle interventions on couples are more effective in weight loss compared to interventions on individuals or standard practice. However, the results should be treated with caution because of the significant heterogeneity of the studies. The number of studies meeting the eligibility criteria for this review is limited and the included studies have different intervention components and levels of couple involvement which make direct comparisons more challenging. Yet, interventions targeting couples, seem to have a small but significant effect on weight loss and a smaller effect on BMI.
It would be beneficial for future research to explore involving younger participants while incorporating longer intervention duration with follow-up, and informing the intervention design by the evidence base.
Footnotes
Abbreviations
RCT, BMI, SD, CVD, WMD
Acknowledgments
The search strategy for this work was developed with the support of Bournemouth University's Faculty of Health and Social Science librarian and the statistical analysis with the support of Dr Orouba Almilaji.
Author contributions
Study concept and design: EIA, FT, JW; data screening: EIA; data extraction: EIA, IT; data analysis: all authors; first draft of the manuscript: EIA; manuscript revision, finalization and agreement: all authors.
Availability of data and materials
Data are available upon request from the correspondence author.
Consent for publication
All authors agree to publish.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Electronic search strategy
Publication date: 1865–26.4.2021
Search:
couple* OR spouse* OR marriage OR husband OR wife OR wives OR partner* OR cohabit*
AND
(Nutrition* OR diet* OR eat*) N3 (intervene* OR counse* OR educat* OR train* OR behav*)
AND
“body composition” OR weight N3 los* OR weight N3 chang* OR weight N3 reduc* OR weight N3 mainten* OR BMI OR “body mass index” OR waist N3 circumference OR “anthropometric characteristics” OR “fat mass” OR “lean mass” OR energy N3 restriction OR improve* N3 diet OR “diet* change” OR “healthy diet” OR “healthy eating” OR eating OR “diet* intake” OR “food intake” OR “food consumption”
Subject headings were also searched using Medical Subject Heading (MESH) using the Medline, EBSCOhost on 28/03/2019 for the period of 1977 to April week 5 2021.
Lifestyle intervention/ gives: “Healthy lifestyle”
AND
Body composition/
Ethical approval
Not required for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.