
Abstract
Keywords
Introduction
The 1989 International Convention on the Rights of the Child recognizes the rights of the child as human rights with consideration for their vulnerability and needs (UN General Assembly, 1959). The global community is in consensus that all children have the right to have their fundamental needs met. Children have the right to good nutrition, care, and support that will ensure their full development (UN General Assembly, 1959, 2015; UNICEF, 2021; United Nations Children's Fund, 2021). Countries and the global community, therefore, are accountable to uphold these children's rights (UN General Assembly, 1959, 2015; UNICEF, 2021; United Nations Children's Fund, 2021). When considering the needs of all children, it is important to recognize those whose rights are marginalized, including many of the nearly 240 million children worldwide living with disabilities (United Nations Children's Fund, 2021). Disability refers to the interaction between physical, mental, or intellectual impairments and a child's environment, which can limit and even restrict their full participation in activities (World Health Organization, 2011).
Childhood is a critical period of growth and development and malnutrition during this time can result in lifelong consequences to health, cognitive and neurobehavioral growth, growth, and limited educational or economic attainment later in life (Gakidou et al., 2017). Malnutrition is defined as “Any condition in which deficiency, excess, or imbalance of energy, protein, or other nutrients… adversely affects body function and/or clinical outcome” (Meier and Stratton, 2008). Millions of children worldwide are impacted by malnutrition, including undernutrition, overnutrition, and micronutrient deficiencies. In 2020, 149 million children were stunted and 45 million were wasted (UNICEF-WHO-World Bank: Joint Child Malnutrition Estimates - 2021 edition interactive dashboard - UNICEF DATA, n.d.). Malnutrition is linked to more than 1 million deaths and 3.8% of the disability-adjusted life years (DALYs) lost globally (Gakidou et al., 2017).
Children with disabilities are at an increased risk of malnutrition (Black et al., 2013a; Black et al., 2013b; DeLacey et al., 2020, 2021, 2022; Groce et al., 2014). Children with disabilities are 25% more likely to be wasted and 34% more likely to be stunted than those without disabilities (United Nations Children's Fund, 2021). This increased risk can be directly and indirectly related to underlying impairments or children's environments. Health and medical conditions that require additional care or present feeding challenges, in addition to economic, social, and cultural norms, can all increase children's risk of malnutrition (United Nations Children's Fund, 2021; DeLacey et al., 2020, 2021, 2022; Groce et al., 2014). Despite being a high-risk population, children with disabilities are often neglected in malnutrition guidelines and determining nutritional status or appropriate assessment methods may be difficult (United Nations Children's Fund, 2021; Engl et al., 2022; Hardy et al., 2018).
Anthropometry is a reliable common way of assessing nutritional status and growth patterns of individuals (World Health Organization Expert Committee, 1995). Common measures include weight, height or length, head circumference, and mid-upper arm circumference (MUAC; Fryar et al., 2021). Anthropometric measures are routinely taken at medical check-ups and plotted on growth charts to illustrate growth patterns and inform clinicians of a child's growth and nutritional status (Fryar et al., 2021). Consecutive anthropometric measurements can help identify abnormal growth patterns, which could be a sign of underlying medical, nutritional, or psychosocial problems (Child Health and Disability Prevention Program, 2016). The World Health Organization's child growth standards and references are commonly used and offer a standardized way to assess anthropometric measures in z-scores or percentiles (World Health Organization, 2007, 2022).
Mid-upper arm circumference is an anthropometric measure that originated in the 1950s (Glasman, 2018). MUAC measurement is widely used because it offers a simple, quick way to identify children at high risk of malnutrition that does not need to be adjusted for age or sex (though MUAC z-score and percentile tables do exist by age and sex) (World Health Organization, 2022). For children 6 months to 5 years of age, the WHO's recommended cutoffs are 11.5 cm for severe malnutrition and between 11.5 cm and 12.5 cm for moderate malnutrition (World Health Organization, 2013). To help with assessment, MUAC tapes are often color coded so that even those with limited numeracy can easily use and interpret them in community settings (Bliss et al., 2018; MUAC,Child 11.5 Red,PAC-50,English, n.d.). Although there currently are not internationally agreed-upon cutoffs for children older than 5 years, research on its application among older children continues, with the potential for MUAC to provide insights into the nutritional status of children of all ages (Shinsugi et al., 2020; World Health Organization, 2009a). However, there is limited information on if MUAC has the potential to be an appropriate or useful measure of malnutrition risk for children with disabilities.
Aim and objectives
The aim of our review is to describe the use of MUAC measurement among children with disabilities. Our objectives were to:
Describe the use of MUAC measurement in the assessment of nutritional status of children with disabilities. Examine the use of MUAC in relation to other anthropometric measurements or the use of MUAC between groups of children (e.g., comparison of those with disabilities to those without disabilities where possible). Explore the usability of current MUAC cutoff values or MUAC z-scores as part of assessing the nutritional status of children with disabilities.
Methods
Search strategy
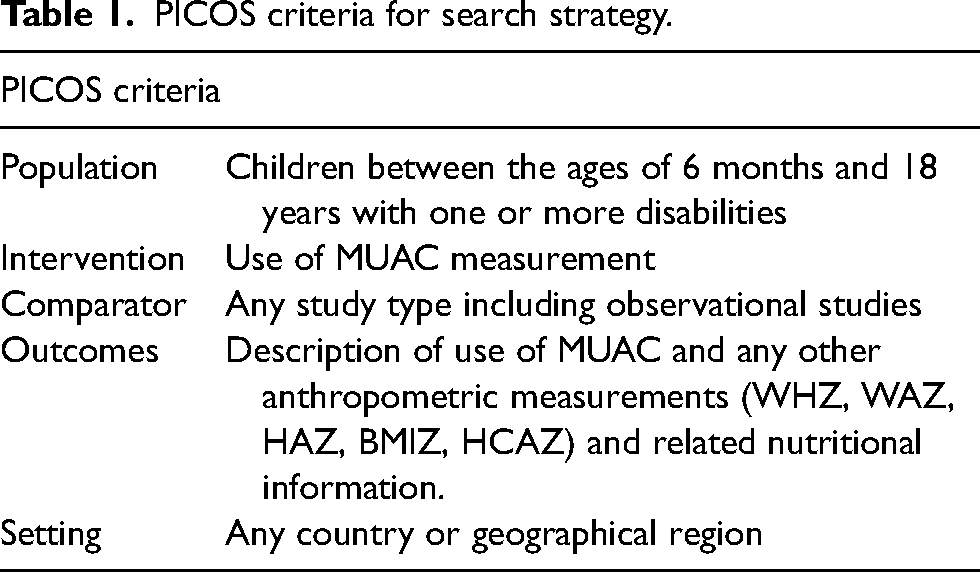
Following PRISMA guidelines, we analyzed existing published peer-reviewed literature on the use of MUAC among children with disabilities (S1) (Page et al., 2021). A PICOS framework was used to develop the research question (Table 1), and a PROSPERO registration was completed prior to the start of the study [PROSPERO 2021 CRD42021258027 Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021258027](Aslam and Emmanuel, 2010). Ethical approval for this systematic review was determined not to be required by the [University Ethics Reference].
PICOS criteria for search strategy.
Inclusion/exclusion criteria
Inclusion criteria included studies published in English from January 1990 through September 2021, which contained research on children with disabilities and MUAC measurements (Table A1). Studies needed to include at least one measurement of MUAC. Other anthropometric indicators were included for comparison (e.g., length/height-for-age, weight-for-age, weight-for-length/height, and BMI-for-age) where available. Full-text cross-sectional studies, case–control studies, cohort studies, and randomized controlled trials conducted in all geographic areas were eligible for inclusion. Studies were excluded if they were conducted in intensive care settings or if MUAC values were used to calculate other arm measurements including upper arm muscle area (UAMA) and upper arm fat area (UAFA) but no values for MUAC were included.
Study selection
JH, ED, and MQ determined and tested the appropriate search strategy. The search strategy was developed with guidance from a search strategy from Banks et al. (Table A2) (Banks et al., 2017). JH and ED applied the finalized search strategy from September 8, 2021, through September 29, 2021. Two electronic databases were searched through OVID, Embase, and Global Health, and two electronic databases were searched through EBSCO Host, PubMed/Medline, and CINHAL Plus. JH and ED independently completed initial title and abstract screening of articles identified by the search strategy. One additional paper was identified for inclusion through other methods. Papers identified by JH and ED as eligible for possible inclusion and full-text review were then analyzed by JH, MQ, and ED against the predetermined inclusion/exclusion criteria. Any discords in the inclusion of full-text studies were discussed among JH, MQ, and ED with ED deciding any discords.
Data extraction and analysis
Studies included were imported into EndNote X9 v12 and Mendeley Desktop v1.19.8 for review, synthesis, and coding (The EndNote Team, 2013; The Mendeley Team, 2008). We undertook data extraction using a standardized form that included study design, location, population, age range, sex representation, disability type, and setting (Table 2a and Table 2b). Data were extracted on methods for MUAC measurement with any variations in terminology, measurement references, or measurement techniques as reported. Z-scores and percentiles for MUAC and other anthropometric measures were included where available.
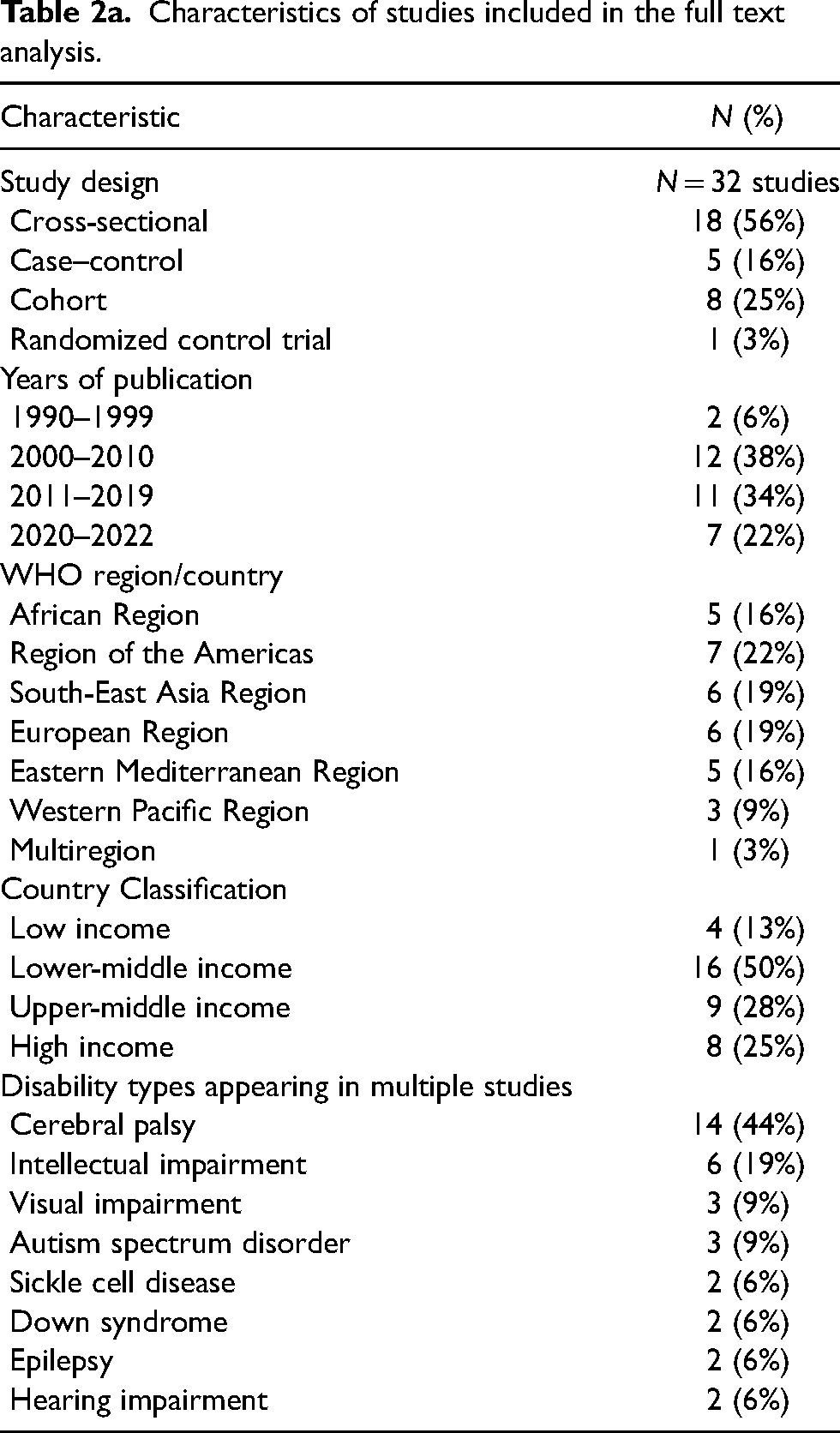
Characteristics of studies included in the full text analysis.
Description of studies included in the review of use of mid-upper arm circumference (MUAC) among children with disabilities.
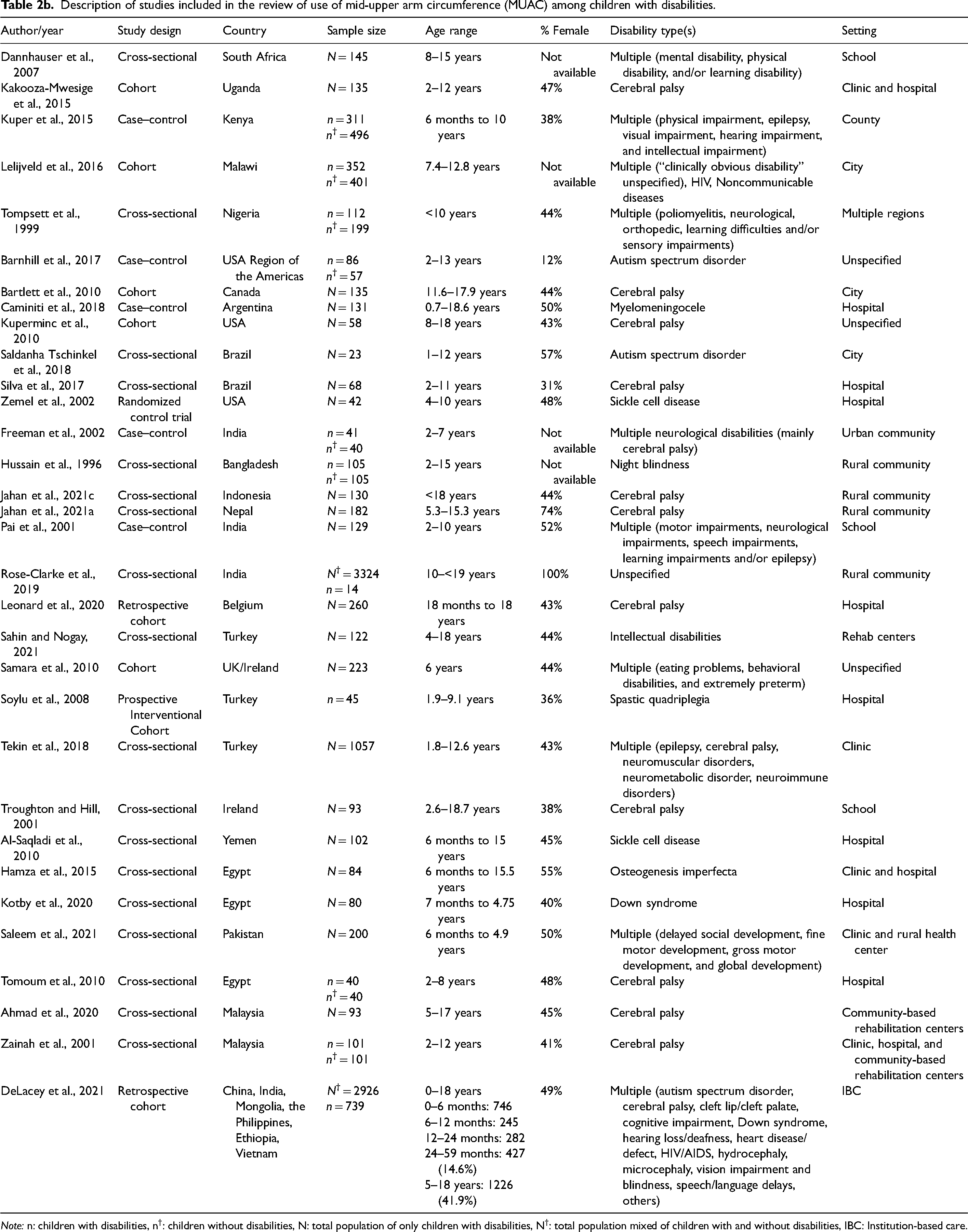
Note: n: children with disabilities, n†: children without disabilities, N: total population of only children with disabilities, N†: total population mixed of children with and without disabilities, IBC: Institution-based care.
Children with specific disabilities were extracted for subgroup analysis if there was sufficient data (e.g., use of MUAC among children with cerebral palsy). Heterogeneity in the data available limited our ability to conduct a meta-analysis, so a narrative synthesis was used.
Critical appraisal
The JBI Critical Appraisal Tool for appraisal of cross-sectional studies, cohort studies, case–control studies, and randomized control trials was used to assess the papers (Moola et al., 2020). Critical appraisal of each study using the appropriate tool for study type can be found in Table A3.1 to Table A3.4.
Results
Study selection
The database search generated 304 studies and one study was found through other methods. After 121 duplicates were removed, 184 records were screened by title/abstract using the inclusion and exclusion criteria, of which 58 were eligible for full-text review (Figure 1). Following a full-text review and critical appraisal, 32 studies were determined to meet the inclusion criteria and 23 studies were excluded (Figure 1, Table A3 and Table A5).
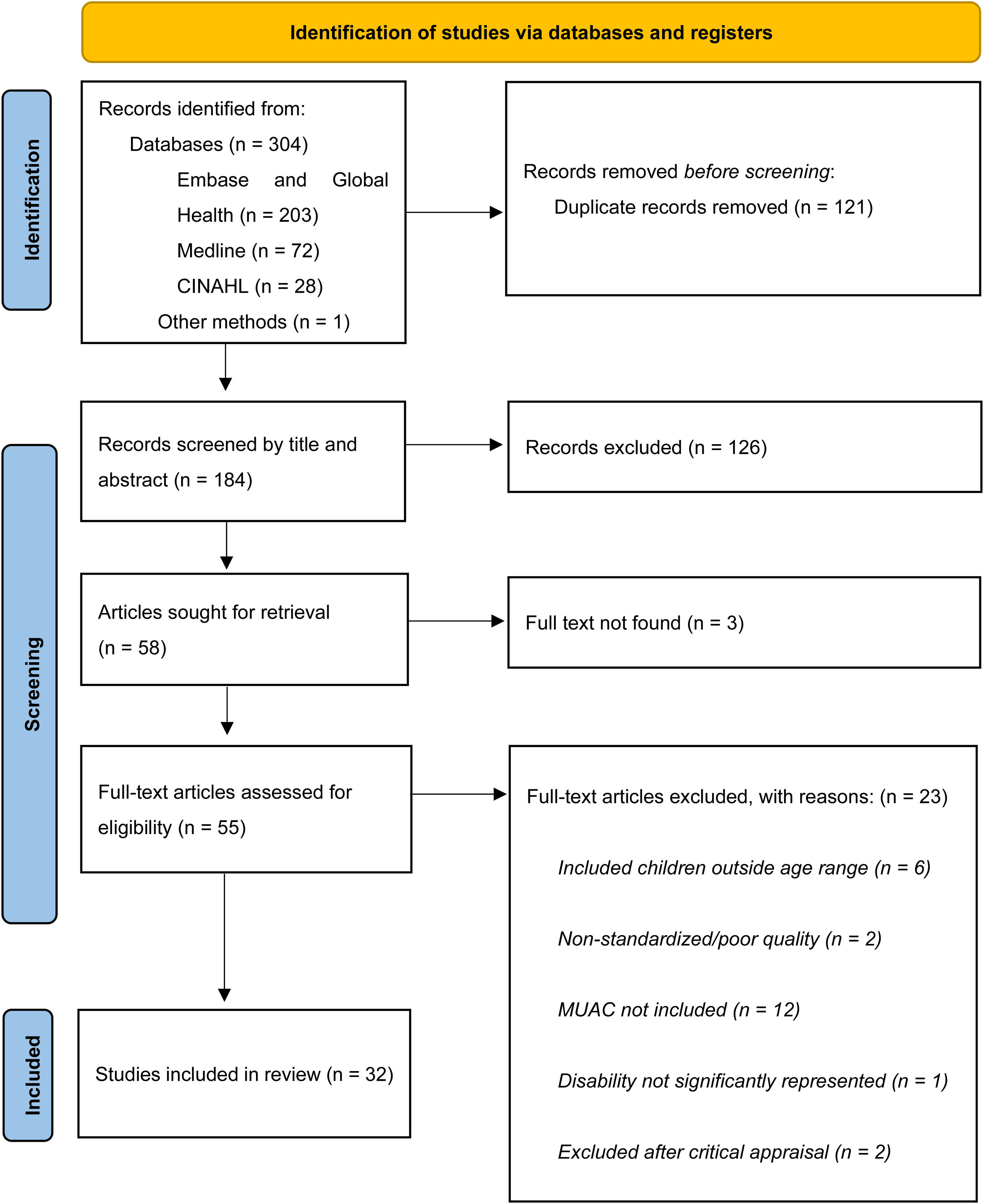
PRISMA flow diagram.
Study characteristics
Most of the studies included in the review were observational studies (29/32, 91%), representing 26 different countries. India, Egypt, and the United States were each represented in 3/32 (9%) of the studies. Of the included studies, over half (17/32, 53%) were published in the past 5 years (2017 through 2021) (Table 2b). The median age of children in the research was 8 years. The most common types of disability reported were cerebral palsy, intellectual impairment, and autism spectrum disorder (Table 2a). Nine studies (29%) included more than one type of disability. Gender was reported in 28 studies (88%). The average female representation among 28 studies was 47%.
There was a wide geographic distribution based on WHO regions. The most common was the Americas represented in seven studies (22%). The European Region and South-East Asia Region were represented in six studies (19%), and the African Region and the Eastern Mediterranean Region both represented in five studies (16%) (Table 2a, Table A4). The distribution of studies among countries of different income levels was also widespread. The most common level represented was lower-middle income countries in 16 studies (50%). Upper-middle income followed, represented in nine studies (28%) followed by high income represented in eight studies (25%).
Anthropometric indicators
Varying anthropometric measurements were reported including weight-for-length/height, length/height-for-age, weight-for-age, BMI/BMI-for-age, weight, height, head circumference, waist circumference, triceps skinfold thickness, and subscapular skinfold thickness (Table 3). Besides MUAC, the most common anthropometric indicator was height-for-age found in 25 (78%) of studies, followed by weight-for-age (24/32, 75%), BMI (20/32, 63%) and weight-for-length/height (14/32, 44%). Additional indicators, such as head circumference-for-age, were reported in several of the studies (20 (63%)).
Mid-upper arm circumference (MUAC) measurement, presentation, and growth references used for other anthropometry, cutoffs, and methods of measurement.
Note: WHO: World Health Organization; WFH: Weight-for-Length/Height; WHZ: Weight-for-Length/Height z score; WAZ: Weight-for-Age z score; HAZ: Length/Height-for-Age z score; cm: centimeter; mm: millimeter.
Use of MUAC
The terminology of MUAC varied in the 32 included studies (Table 3). Additional information on MUAC terminology, methods for MUAC measurement, measurement references (e.g., WHO, CDC) and data reported for MUAC and other anthropometric indicators (e.g., weight-for-age, height-for-age, weight-for-length/height, and BMI) are included in Table A4. Although most studies referred to MUAC using MUAC or a variation of all those words, 11 used other variations that did not include MUAC (Table 3). Few studies reported methods for measuring MUAC. Twelve of the studies (12/32, 38%) specified if the measurement was completed on the mid-upper arm, if the left arm was used, and if the arm was at a 90° angle for the measurement and seven (7/32, 22%) noted measurements were obtained to the nearest 0.1 centimeter. Only one study mentioned using a specialized MUAC tape. Nonstandard, limited descriptions of the methods used for MUAC measurement were common among the few studies that reported methods. How MUAC measurements were presented also varied greatly among the studies. Sixteen (50%) studies presented MUAC values as means with standard deviations, 11 (34%) presented MUAC values as the number or percentage of children within a specific percentile, and 6 (19%) used z-scores to present MUAC values obtained for specific groups. Four studies (13%) presented MUAC results in other ways and two studies (6%) did not include MUAC values but did mention MUAC in their methods sections. When grouped by disability type, using means with standard deviations was most common for studies that included children with multiple types of disabilities (6/9, 66%). Several of the studies included children over 5 years in MUAC analysis or did not specify the ages included.
Reference values for MUAC
MUAC reference values that were used are shown in Table 3. Publication years ranged from 1996 to 2021. Growth references evolved through this period and, therefore, variation in references used for anthropometric measurements is notable. In studies dated 1996 through 2010, the US National Center for Health Statistics (NCHS) data were used most, in six of 14 studies published during this time. In the studies dated 2015 through 2021, WHO growth standards became common, referred to in 16 out of 18 studies published during this time frame. Additionally, three studies noted the use of findings by Frisancho based on NCHS data and the Nutritional Examination Survey of 1971 to 1974 for the assessment of anthropometric measurements (Table 3) (Frisancho, 1981, 1990).
MUAC vs. Weight-for-length/height
Of the studies included, 15 (47%) studies included measurements for both MUAC and weight-for-length/height (Table 3 and Table 4). Of these studies, four (27%) reported MUAC and weight-for-length/height as means with standard deviations, five (20%) reported each as the number and/or percentage of children with measurements within a specified range or percentile, three (20%) studies reported both as mean z-scores. Among the 12 studies that reported both MUAC and weight-for-length/height with the same method (mean ± standard deviation, number and/or percentage of children with measurements with/in a specified range or percentile, or z-scores), five reported anthropometric data in multiple ways. Four studies did not report MUAC and weight-for-length/height in comparable ways. A comparison of MUAC measurements with weight-for-length/height measurements among these studies is included in Table 4. Of the studies that included measurements for both MUAC and weight-for-length/height only eight reported both with the same methods. Despite the limited comparability of these two indicators in the data, narrative data from the studies suggest that MUAC was a useful measure, especially for children with disabilities for which obtaining height is a challenge.
Comparison of mid-upper arm circumference and weight-for-length/height anthropometry with age ranges as specified in each study of children included in the entire study or for only those who received MUAC measurements, and/or those who received weight-for-length/height measurements as available.
Note: SD: standard deviation; WFH: Weight-for-Length/Height; WHZ: Weight-for-Length/Height z score; cm: centimeters.
Discussion
We found that MUAC is being used in the assessment of the nutritional status of children of all ages with various disabilities in several countries within different settings. However, methods for obtaining MUAC measurements and reporting methods varied markedly. The 32 papers included in this review indicated that most children with disabilities were able to be measured using MUAC as part of assessments examining nutritional status, although few studies compared MUAC to other anthropometry or analyzed the findings within the broader context of changes in nutritional status or long-term health outcomes. There were also limited data on how MUAC use compared for children with disabilities to counterparts without disabilities and only limited reference to the use of MUAC for children with disabilities older than 5 years of age, despite several of the studies including children over 5 years of age in their analysis, and there are no internationally agreed-upon MUAC references for older children. Additionally, none of the studies examined MUAC's ability to identify children at high risk for malnutrition-associated adverse outcomes (notably mortality, morbidity, and impaired neurodevelopment in comparison to other indicators. This limited the comparability of the prevalence and severity of undernutrition as identified by MUAC-based assessment versus weight-for-length/height z-score-based assessment. Standardized references for cutoffs available at the time of publication were mostly used, however, not all studies referenced the guidelines used for MUAC specifically. Together, these are notable findings because the lack of clear standardized reporting limits the examination of the applicability of MUAC for children with disabilities.
Anthropometry and use of MUAC in nutritional assessment
Anthropometry is key to assessing nutritional status and evaluating children's growth and health (World Health Organization, 2007, 2022). It is not, however, a direct measure of nutrition and there is no single “gold standard” anthropometric measure (Kerac et al. 2020). All have benefits and limitations and are best presented together to evaluate clinically relevant health and developmental risks. MUAC is commonly used in conjunction with other anthropometric measurements as a part of nutritional assessments, in addition to being often used as an independent criterion for identifying children at high risk of mortality and morbidity in resource-limited and humanitarian settings (Myatt et al., 2006; Sørensen et al., 2021). Over the last few decades, the use of MUAC as an anthropometric indicator has evolved, specifically the type of tape used for the measurement and reference cutoffs (Rana et al. 2021). In 1997, the WHO first published a standard reference for MUAC, which was updated in 2007 and then again in 2009 (Glasman, 2018). The widely used threshold for moderate malnutrition (wasting) for children 6 months to 5 years old is under 12.5 cm and under 11.5 cm for severe wasting. These thresholds are also independent admission criterion for most therapeutic and supplementary feeding programs. As part of the new 2006 child WHO growth standards, MUAC-for-age references were also developed (World Health Organization and UNICEF, 2009). MUAC offers some advantages over other measures due to its simplicity, speed, and ease of use, as well as not requiring age and sex adjustment. This makes it suitable for use in most settings including large-scale community services and programs. There is even research that suggests the use of MUAC by families to assess their own children (Blackwell et al., 2015; Bliss et al., 2018).
Anthropometry for children with disabilities
Older guidelines suggest that anthropometric results from children with disabilities should be disregarded (Tompsett et al., 1999). However, near the turn of the twenty-first century, researchers recognized the importance of resolving the measurement gaps between populations so that all children, regardless of ability, could achieve their right to good nutrition (Child Health and Disability Prevention Program, 2016; Tompsett et al., 1999; UN General Assembly, 1959). Despite this recognition by Tompsett et al. more than 20 years ago, there remains a gap in the research and recommendations for the use of anthropometric measurements among children with disabilities (Child Health and Disability Prevention Program, Health Assessment Guidelines, 2016; Tompsett et al., 1999; United Nations Children's Fund, 2021). The WHO provides clear guidance on anthropometric measurements for children but there is limited or unclear information on the appropriateness of these measures for children with varying types of disabilities (World Health Organization, 2008, 2022). This is also true for other nutritional assessment tools including ESPGHAN, NCHS, and the CDC (Centers for Disease Control and Prevention, 2000; Published Guidelines - ESPGHAN, n.d.).
Several of the studies in this research note the challenges of conducting anthropometric measurements for children with physical disabilities. Disabilities that can present with physical impairments, such as cerebral palsy, were the most common disabilities included in the studies (21/32, 66%). Due to physical characteristics such as body contractures and spinal deformities found in varying degrees of severity among children with cerebral palsy, there are questions about which anthropometric measurements are most appropriate for use in this population (Zainah et al., 2001). Length/height-based measurements for some children with CP and other physical disabilities can be challenging and can either result in missing values or incorrect values—such as underestimating height when a child cannot stand or lie straight. This could result in a falsely high weight-for-height (WFH), missing true cases of malnutrition and misidentifying children eligible and needing to enter nutrition treatment or feeding programs. Troughton and Hill were unable to obtain height measurements in 20% of their study population due to contractures (Troughton and Hill, 2001). Additionally, other disabilities such as Down syndrome and some intellectual disabilities can present with varying composition of body fat and lean masses (González-Agüero et al., 2011; De Lopes et al., 2008). This is important because not being able to get an accurate height measurement limits the application of several other anthropometric indices including weight-for-length/height or BMI-for-age (Hardy et al., 2018). Some research supports the use of other equations or alternative height measurements, such as upper arm length or lower leg length, but these also present with limitations for the use of other standardized references such as BMI-for-age and weight-for-length/height and their associated growth charts (Zainah et al., 2001). Our research found a limited discussion on how varying disabilities may impact MUAC measurement accuracy.
Use of MUAC for children with disabilities
Our research found that MUAC is commonly being used for children of all ages with disabilities of all types and severities. This highlights the need that health care providers and programs have to track and monitor the growth and nutritional status of children with disabilities—that even without internationally agreed-upon guidance, people are seeking ways to provide inclusive care. However, there was little insight in this research on referral systems to nutrition programs or services for children with disabilities when malnutrition was indicated. Identifying if a child with disabilities falls below the MUAC thresholds, presents the opportunity to have them referred to lifesaving treatment programs and potentially removing another barrier that excludes children with disabilities from services (Bhutta et al., 2017; United Nations Children's Fund, 2021). Our findings suggest that MUAC is a valuable part of multimodal nutritional assessments for children with a wide variety of disabilities, especially when measurements are routinely tracked. Through routine tracking, it becomes possible to gain insights into a child's overall nutritional status and growth patterns (Shinsugi et al., 2020; World Health Organization, 2007, 2009b, 2022). However, the variance in data presentation among the studies reveals that greater research on this topic is necessary for the guidance of the development of accurate and reliable reference data and measurement tools for this population. There were limited and inconsistent descriptions of methods but it is clear that finding methods for identifying children with disabilities who are at high risk for malnutrition is necessary. Not having clear MUAC guidelines for children with disabilities is a serious issue since optimal cutoffs for referral to nutrition support services are unknown and these children may be:
Smaller than the general population—children with disabilities are more likely to be stunted, wasted, or underweight. Have variations in muscle mass and fat deposits related to some genetic disorders or disabilities. Larger than the general population— some children with disabilities may mobilize using their arms and thus have a larger-than-normal MUAC.
Future research
Future research should work toward identifying anthropometric measurements that are appropriate for children with disabilities. For a population with greater needs and at higher risk of nutritional challenges, understanding and supporting their unique growth patterns and development needs is imperative. This research highlights the clear gaps in information on the use of MUAC for children with disabilities. Future research on the use of MUAC should include not only children of all ages but also children with different types of disabilities and present clear standardized methods of MUAC measurement and reference values (United Nations Children's Fund, 2021; Mramba et al., 2017). MUAC presents as a potentially more disability-inclusive measure, especially for those who face challenges in having their length/height measured or have difficulty with being weighed. Clear guidance on its use could enable more children to be reached and included in treatment programs for malnutrition (United Nations Children's Fund, 2021). In combination with other anthropometric measures including weight-for-length/height, length/height-for-age, weight-for-age, and BMI, it could help build a greater foundation of population-specific data to inform future programming, practices, and policies. A key question for examination in future research is whether mortality/morbidity and development risks are the same for children with disabilities with a low MUAC as for children without disabilities with a low MUAC. Do thresholds need to be adjusted to take the disability into account—and if so, which thresholds are for which types of disabilities? WHO guidelines are highly regarded and used to develop malnutrition protocols worldwide, but the lack of disability-specific recommendations leaves children with disabilities underserved. Through future research examining the use of this anthropometric indicator, we can work toward creating more inclusive health systems.
Strengths and limitations
This study utilized a comprehensive search strategy with inclusive terms for disability. One strength of this research was the studies included came from several countries in different geographical settings of varying income classifications. Of the papers identified, the use of nonstandardized language, measurements, or methods was common. Despite the lack of internationally agreed-upon standards, many of the studies used MUAC for children of all ages and with various disabilities. Additionally, our search strategy included studies from 1990 to 2021 during which research and findings on the use of MUAC have markedly changed and developed. This paper was limited to peer-reviewed research published in English.
Although some research was found, this review did not find enough comparable studies to assess MUAC's ability to identify malnutrition-associated adverse outcomes in children with disabilities compared to those without or compared to other anthropometric indicators or other subgroups of children. This could be related in part to the limited inclusion of children with disabilities in research (DeLacey et al., 2020; United Nations Children's Fund, 2021). Importantly, no study asked the key question of which anthropometric measure best identifies children at high risk of mortality/morbidity/poor development. This information is critical to being able to understand the true benefits of different measures (Mwangome et al., 2012). Neither did any study directly explore the reliability of the different measures as would be ideal to know (Mwangome and Berkley, 2014).
There is the potential for some publication bias within this systematic review, as the focus of these studies often limited what was reported in terms of outcomes and anthropometric indicators. There is a potential risk of measurement bias for the anthropometric measures. Additionally, causes of malnutrition may be underdiagnosed for children with disabilities, possibly related to perceptions of disability in different contexts or for individual children with disabilities who may weigh less or have a reduced height related to their clinical sequelae (Groce et al., 2014; United Nations Children's Fund, 2021). There are also many types of disabilities, but this research was limited by the available data in the studies which included children with various disabilities, who may have been selectively included for their high risk of malnutrition or for other factors such as severity of disability. Furthermore, disabilities are identified in various ways in different countries. Future research in this area could explore utilizing standardized disability identification methods such as the Washington Group Questionnaire (Grellety et al., 2015).
Findings from this study should be used with caution, especially from the studies which included children older than 5 years, for whom there are no internationally agreed-upon MUAC ranges for nutritional assessment. Additionally, the needs of individual children with different types of impairments should be considered; although routine tracking of anthropometric indicators over time should identify children whose growth patterns are flat or declining, interventions to address their growth will vary. Given the biological links between malnutrition, development, and disability, evaluation of the most useful tools to track and monitor children's nutritional status should be prioritized.
Conclusion
There are 240 million children worldwide living with a disability, many of whom are at high risk for malnutrition. These vulnerable children continue to be routinely excluded from health services, nutrition programs, research, and even basic demographic and census data—all of which could improve their lives. Without tools to measure and count these children, they will continue to be underserved or excluded. MUAC is currently being used among children with disabilities and presents a potentially valuable part of anthropometric assessment for this population but there is a limited amount of interpretable or clear data on its use. Without validated measures to identify malnutrition and monitor the growth of these children, millions could have severe but avoidable consequences to their health and development. Future research should examine the use of MUAC both as part of multimodal nutrition assessments and as a tool for identifying children at high risk of malnutrition-associated adverse outcomes, especially when other anthropometric measurements may not be appropriate based on clinical sequelae.
Supplemental Material
sj-docx-1-nah-10.1177_02601060231181607 - Supplemental material for Mid-upper arm circumference (MUAC) measurement usage among children with disabilities: A systematic review
Supplemental material, sj-docx-1-nah-10.1177_02601060231181607 for Mid-upper arm circumference (MUAC) measurement usage among children with disabilities: A systematic review by Julia Hayes, Michael Quiring, Marko Kerac, Tracey Smythe, Cally J Tann, Nora Groce, Zerihun Gultie, Lydia Nyesigomwe and Emily DeLacey in Nutrition and Health
Supplemental Material
sj-docx-2-nah-10.1177_02601060231181607 - Supplemental material for Mid-upper arm circumference (MUAC) measurement usage among children with disabilities: A systematic review
Supplemental material, sj-docx-2-nah-10.1177_02601060231181607 for Mid-upper arm circumference (MUAC) measurement usage among children with disabilities: A systematic review by Julia Hayes, Michael Quiring, Marko Kerac, Tracey Smythe, Cally J Tann, Nora Groce, Zerihun Gultie, Lydia Nyesigomwe and Emily DeLacey in Nutrition and Health
Footnotes
Acknowledgments
Ali Murray, Mihret Berhanu, Iqra Ilyas.
Author contributions
Study design, E.D., J.H., M.Q., and M.K.; title and abstract review, J.H. and E.D.; full-text reviews, J.H., E.D., and M.Q.; methods, data analysis and quality control, J.H., M.K., T.S., M.Q., C.T., N.G., Z.G., L.N., and E.D.; data analysis and writing—original draft preparation, J.H. and E.D.; writing—review and editing, J.H., M.K., T.S., M.Q., C.T., N.G., Z.G., L.N., and E.D. All the authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the London School of Hygiene and Tropical Medicine.
Ethical Review Statement
Ethical review and approval were waived for this study from the London School of Hygiene and Tropical Medicine (25468 /RR/23165). Research was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments or comparable standards.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.