
Abstract
Youth with autism spectrum disorder (ASD) demonstrate unhealthy eating behaviors and dietary patterns compared to their neurotypical counterparts. Given the increased risk of unhealthy weight gain and the onset of the COVID-19 pandemic, modified nutrition programs in this population are warranted. The authors independently conducted two virtual pilot interventions during COVID-19 that offered feasible and acceptable alternatives to in-person delivery, providing unique opportunities for participant engagement and family involvement. Future virtual nutrition education programs for adolescents with ASD may include visual and verbal aids through Zoom, more parent/family integration, and accommodations for those with varying ASD severity levels.
Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by social, communication, and behavioral challenges (American Psychiatric Association, 2013). Such challenges may negatively affect health behaviors, such as dietary intake, physical activity, and sleep quality in this population (Matheson and Douglas, 2017). Youth with ASD are more likely to exhibit problematic eating behaviors, such as food selectivity (Marí-Bauset et al., 2014), often leading to nutritional deficiencies and a higher intake of energy-dense foods, compared to their neurotypical (NT) peers (Sharp et al., 2013). As a result, youth with ASD have an estimated 58% increased risk of developing obesity compared to NT youth (Sammels et al., 2022), which could lead to subsequent obesity-related chronic diseases such as cardiovascular disease and metabolic syndrome (Flygare Wallén et al., 2018; Li et al., 2020). Given the prevalence of imbalanced nutrient intake and unhealthy weight outcomes, interventions that promote healthy eating habits in this population are warranted.
Despite the need for nutrition education interventions for adolescents with ASD, there is a lack of interventions aimed at improving long-term healthy eating habits in this population. Many existing interventions for youth with ASD focus on addressing feeding difficulties, such as food selectivity, rather than increasing nutrition self-efficacy, and have primarily focused on young children (Galpin et al., 2018; Marshall et al., 2015; Miyajima et al., 2017; Muldoon and Cosbey, 2018; Sharp et al., 2019; Tanner and Andreone, 2015). Social cognitive theory (Bandura, 1989) has been applied to nutrition interventions for individuals without ASD to target healthy eating self-efficacy (Vilaro et al., 2016).
The onset of the COVID-19 pandemic and subsequent restrictions on in-person activities and programs created additional barriers to engaging in healthy eating and physical activity for adolescents with ASD (Garcia et al., 2021). As a result, alternative methods of providing health promotion programs, such as remote-based delivery, have been suggested. Although virtual interventions have been shown to be well-accepted in ASD populations, the majority of nutrition-related virtual interventions have been limited to NT adolescents (Ajie and Chapman-Novakofski, 2014; Rose et al., 2017). Only a few studies have conducted nutrition interventions in youth with developmental disabilities; however, these studies examined youth with developmental disabilities rather than ASD specifically, have primarily focused on life skills such as grocery shopping rather than nutrition-related topics, and had limited sample sizes (Hansen and Morgan, 2008; Kim and Kang, 2020; Mechling and Cronin, 2006; Mechling et al., 2002).
The current report describes the development, implementation, and evaluation of two novel virtual nutrition education interventions for adolescents with ASD (Buro et al., 2021; Shurack et al., 2021). The authors of both studies documented the feasibility and acceptability of the two virtual pilot programs. Given the need for nutrition interventions for adolescents with ASD, especially with the transition from in-person to virtual delivery of education during COVID-19, it is imperative to share key findings, lessons learned, and implications of these piloted interventions.
Summary
Description of the interventions
Two pilot nutrition education interventions utilized videoconferencing platforms to reach adolescents with ASD while practicing social distancing during COVID-19. One was conducted via Microsoft Teams (“the Teams intervention”), and one was conducted via Zoom (“the Zoom intervention”). Both interventions were developed based on social cognitive theory. Table 1 summarizes the main components of both programs.
Overview of the virtual pilot interventions.
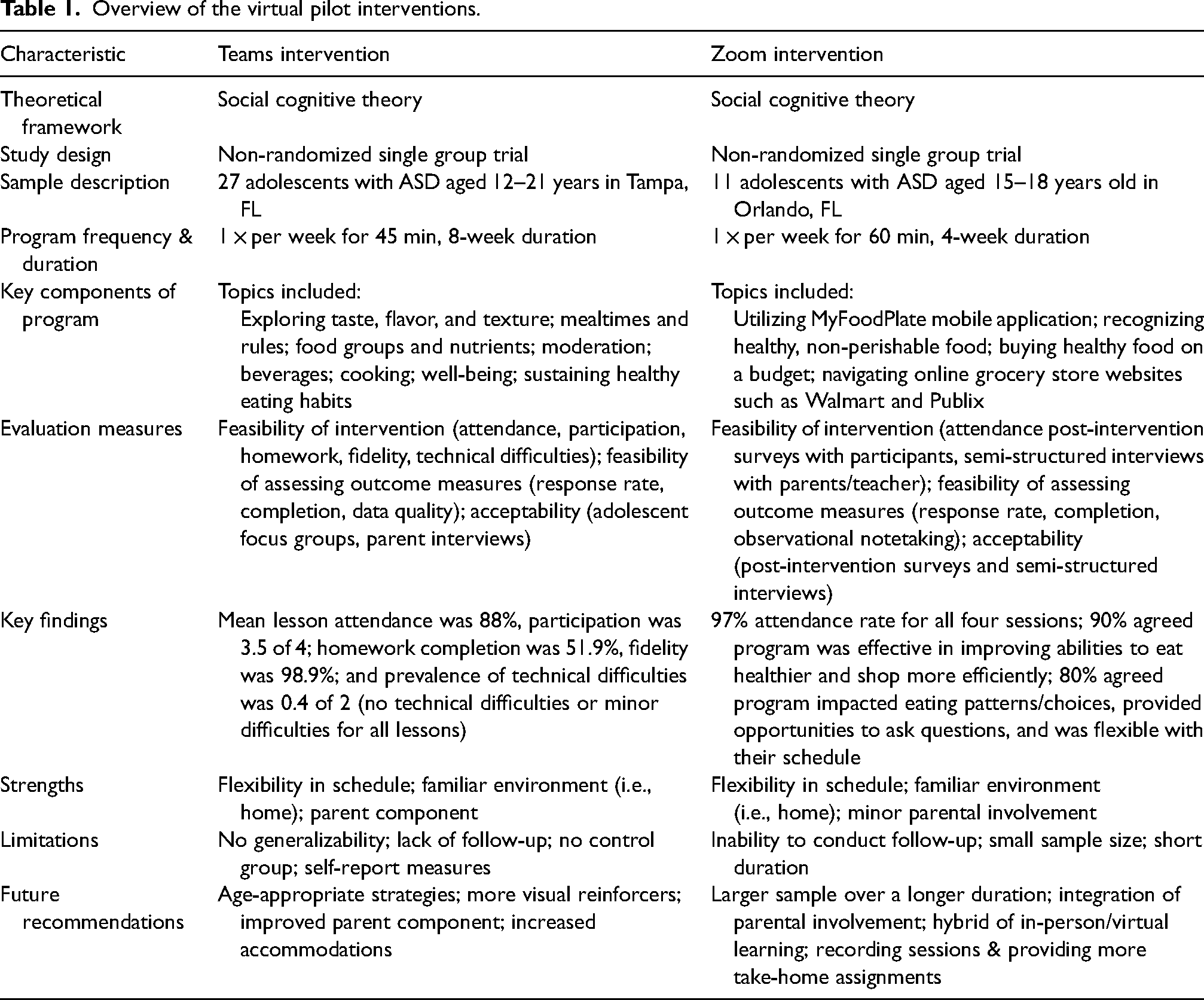
The Teams intervention consisted of eight weekly lessons that were initiated within an in-person setting and adapted for virtual implementation via Microsoft Teams (n = 27, with six groups of 2–7 adolescents aged 12–21 years) (Buro et al., 2021). Sensory activities including food tasting and preparation and visual and verbal prompts in the form of lesson booklets to reference during and between lessons and printed activity cards were utilized to engage participants. The intervention also included a parent component with weekly parent handouts and three parent webinars (at baseline, after Lesson 4, and after Lesson 8). The parent webinars reviewed lesson content and discussed ways that parents could provide social support and opportunities for their children to practice healthy eating habits.
The Zoom intervention was initially a school-based intervention conducted in-person twice a week for six weeks and adapted to a virtual format one session per week for four weeks via Zoom (n = 11, aged 15–19 years) (Shurack et al., 2021). Participants were encouraged to ask and answer questions either by unmuting themselves utilizing the Microphone feature or by writing in the chat box. Visual prompts were mainly utilized to engage participants, with one example including the Screen Share feature on Zoom to display websites for well-known grocery stores to learn online grocery shopping and shopping on a budget. Another instance was the implementation of mobile applications such as the USDA MyFoodPlate application to track nutrition goals and achieving requirements for food group intake.
Description of intervention evaluation
Both nutrition education pilot studies evaluated measures of feasibility and participant acceptability. For the Teams intervention, feasibility was assessed using fidelity checklists to calculate percentage fidelity for each lesson, and engagement records were used to calculate attendance, participation, homework completion, and technical difficulties. Feasibility of outcome measures, such as the Block Kids Food Frequency Questionnaire (Cullen et al., 2008) and participant height and weight measurements, was determined based on response rate, completion, and data quality. Frequency distributions and descriptive statistics were performed for all feasibility measures (Buro et al., 2021). Six adolescent focus groups (n = 12) and 21 parent interviews were audio-recorded, transcribed, and analyzed for themes regarding intervention acceptability, perceived benefits, and unintended consequences using a coding reliability approach to thematic analysis (Buro et al., 2022).
Feasibility and acceptability measures for the Zoom intervention included participant attendance sheets, post-intervention surveys administered to participants, and post-intervention interviews with the parents/caregivers and classroom teacher. Ten participants completed a survey with 11 close-ended question and two open-ended questions that were formatted to measure perceptions of the intervention and the virtual delivery format. Parents/caregivers (n = 9) participated in semi-structured interviews, approximately 10 min in length, that focused on their perceptions of program feasibility and acceptability for their children. The classroom teacher participated in a 60-min semi-structured interview that focused on benefits and limitations of the virtual sessions, feasibility of the program for future classes of students, and suggestions for program improvement. Both parent and teacher interviews were audio-recorded and transcribed verbatim. Means and frequencies were calculated for participant characteristics, attendance, and responses to the post-intervention surveys. Two researchers independently coded the qualitative data, and content analysis was used to quantify the frequency of relevant themes extracted from the participants’ open-ended responses and parent/teacher interviews (Shurack et al., 2021).
Key findings
Both interventions reported the following key findings: (1) high attendance rate; (2) high participant acceptability; and (3) importance of family involvement, which was minimal in our interventions but could be strengthened in future interventions to further promote positive behavior change. Mean attendance for the Teams intervention was 88% (ranging 50–100%), and attendance rate for the Zoom intervention was 97%. All participants in both programs reported that the virtual format was feasible and acceptable, as the virtual setting eliminated the need to travel to and from intervention sessions, providing more flexibility in their schedules for participation. It also allowed for participants to partake in the interventions in the familiarity of their homes, which may be considered as ideal in individuals with ASD who struggle with changes in activity or routine (Lamash et al., 2022). Participants reported that there were adequate opportunities for interaction and engagement in both interventions through the usage of webcams, screen sharing, and chat.
The virtual setting also allowed for greater family involvement, as parents were able to stay informed on what their children were doing in both interventions. Although there was no direct parental involvement during the participants’ sessions in either intervention, parents of adolescents who participated in the Teams intervention were invited to attend three webinars that covered the lessons taught during the sessions and received weekly parent handouts. In both interventions, parents were able to see what was being taught to the participants since the virtual lessons were conducted in the environment of the participants’ homes, and therefore felt encouraged to partake in associated conversation and activities with the participants. Not surprisingly, parents whose children were involved with the Zoom intervention reported in their interviews the desire to be involved in a future program to further encourage their children to practice learned skills. Parents from both interventions further indicated that the virtual format provided a unique opportunity for their children to actively participate. In the Teams intervention, participants reported that the format was convenient and comfortable, especially for those who struggled with crowds or face-to-face interactions. The teacher from the Zoom intervention reported that adolescents who were quiet in-person were more engaged via Zoom, and both parents and the teacher explained that adolescents would participate in more open discussion about nutrition and healthy eating.
Lessons learned
The authors’ pilot interventions provided insights regarding best practices for engaging participants in virtual nutrition education programs, as participant engagement was found to be high in both settings. The virtual format may also be particularly helpful for adolescents with anxiety, as these adolescents may also benefit from virtual accommodations that may not be feasible for in-person settings, such as turning off their webcam or using the chat feature to answer questions instead of turning on the microphone. After the Teams intervention, parents reported that the handouts helped them stay informed but that asynchronous, shorter videos would be more convenient than webinars. Although both videoconferencing applications were easy to access for most participants, many Teams participants said that they were more familiar with Zoom, and Microsoft Teams posed technical barriers for those with netbooks.
Although both programs were reported to be feasible and acceptable to participants, it is important to note that these findings may not be generalizable to participants with greater ASD severity levels. Since the majority of participants in both studies were diagnosed with Level 1 ASD (i.e. requiring minimal support), additional facilitator or parent/caregiver support may be required for similar virtual programs in adolescent populations with Level 2 or 3 ASD (i.e. requiring substantial or very substantial support).
Implications for research and practice
Findings from the two pilot studies demonstrate the feasibility and acceptability of virtual nutrition education programs for adolescents with ASD. The implications of these findings extend beyond the context of the current COVID-19 pandemic and propose a novel format that has the capacity to reach a greater percentage of this population compared to traditional in-person settings. Future virtual nutrition education interventions for this population should consider using visual and verbal prompts to interact with adolescents via Zoom and asynchronous/brief videos or activities to engage parents and families. Additional assistance such as technical support and more facilitators could also be incorporated to adequately meet the needs of their participants.
Footnotes
Author contributions
All authors contributed to writing and editing the manuscript. All authors read and approved the final manuscript.
Author note
Riley H Shurack is currently affiliated with Department of Health Sciences, College of Health Professions and Sciences, University of Central Florida, Orlando, FL, USA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially funded by the University of South Florida Research and Innovation Internal Awards Program under Grant No. 0128126 and the University of South Florida College of Public Health Student Research Scholarship. AWB was supported by the NIH Behavioral Oncology Education and Career Development Grant (T32CA090314, MPIs Vadaparampil/Brandon).