
Abstract
Keywords
Introduction
Americans are not meeting dietary recommendations leading to additional medical costs and increased risk for chronic diseases. High diet quality, which includes the quality and variety of foods and beverages consumed (Wirt and Collins, 2009), is rarely achieved by Americans. According to the National Health and Nutrition Examination Survey (NHANES), the average diet quality of Americans as measured by the Healthy Eating Index (HEI) is 57.7 out of 100 (U.S. Department of Health and Human Services and U.S. Department of Agriculture, 2015). Improving the diet quality of Americans could save over $50 billion dollars annually in medical costs related to cardiometabolic disease alone (Jardim et al., 2019). In addition to decreasing medical costs, high diet quality has been associated with a reduced risk of mortality, type 2 diabetes, cancer, mortality among cancer survivors, and cardiovascular disease (Morze et al., 2020). Thus, interventions that increase diet quality are essential.
Weight-neutral or non-diet interventions (e.g. intuitive eating, mindful eating, eating competence, and Health at Every Size® (HAES)) that promote adaptive eating behaviors have become a growing area of research and practice, with evidence of positive health benefits (Clifford et al., 2015; Warren et al., 2017). However, research in community samples and interventions connecting these adaptive eating behaviors with diet quality is limited and inconclusive (Camilleri et al., 2017; Grider et al., 2021; Horwath et al., 2019). Alternatively, traditional behavior change interventions focus on weight reduction, requiring adherence to external recommendations and reliance on dietary restriction.
The Embodied Self Model differentiates the two approaches as either adaptive (e.g. weight-neutral or non-diet) or maladaptive (e.g. restriction) according to the process of attunement (Cook-Cottone, 2015, 2020). The Embodied Self Model describes two systems: the internal system (physiological, emotional, and cognitive needs of the body), and the external system (family, community, and culture). The process of attunement occurs with the alignment between internal and external systems (Cook-Cottone, 2015). Based on this perspective, adaptive eating behaviors are guided by internal cues rather than external expectations or guidance. Alternatively, maladaptive eating behaviors abandon internal cues, reject the internal self, and rely on external factors for motivation (Cook-Cottone, 2015). Described as misattunement, this process disregards functionality and embodiment, placing importance on external influences to guide behavior. According to the Embodied Self Model, attunement and adaptive behaviors may support diet quality (Tribole and Resch, 2020).
Body image may be an important factor due to its close relationships with adaptive and maladaptive eating behaviors (Avalos and Tylka, 2006; Stice, 2002). According to the Embodied Self Model (Cook-Cottone, 2015), influences from external and/or internal systems can contribute to misattunement, prompting the individual to see the self as unacceptable, and the body as something to control or change, rather than honor and embody (Cook-Cottone, 2015). Alternatively, appreciation of the body may lead to attunement and adaptive behaviors; honoring the internal aspects of the self.
Body image and diet quality
The field of body image has expanded beyond a pathological focus to that of a multidimensional concept, encompassing body-related attitudes and perceptions of the self, including feelings, thoughts and behaviors (Cash, 2004), Historically, body image and eating behavior research focused on negative constructs such as body dissatisfaction and eating disorders (Stice, 2002). However, recent research suggests positive and negative body image are two qualitatively different constructs (Halliwell, 2015; Tiggemann and McCourt, 2013). Negative body image includes dissatisfaction and a negative valuation of the body, while positive body image is defined as an overarching respect and appreciation for the body and its functionality, including acceptance of the body, a feeling of beauty, comfort, and confidence and the ability to interpret information using a body-protective manner (Halliwell, 2015). Negative body image is closely related to disordered eating, restriction, and eating disorders (Stice, 2002; Stice and Shaw, 2002), while positive body image is related to adaptive eating behaviors (Homan and Tylka, 2018; Tylka and Kroon Van Diest, 2013). While relationships between body image and eating behaviors have been established in previous research, the relationships between body image and diet intake are less well known.
We identified two studies that assessed the relationship between negative body image and diet quality, with mixed findings (Anton et al., 2000; Contento et al., 2003). One study of female college students found a larger discrepancy between actual and ideal body size was associated with the consumption of less healthy foods (Anton et al., 2000). Alternatively, in Latina mothers, higher body dissatisfaction was associated with healthier intake (Contento et al., 2003).
We were unable to identify any studies exploring positive body image and diet quality. However, in college students body appreciation was positively associated with self-reports of following a low-fat, low-salt diet (Thomas and Warren-Findlow, 2020) and negatively associated with less healthful behaviors including taking weight loss supplements in women (Andrew et al., 2016).
Eating behaviors and diet quality
Research has begun to assess whether adaptive and maladaptive eating behaviors are qualitatively different or on opposite ends of a continuum (Barrada et al., 2018; Kerin et al., 2018; Ruzanska and Warschburger, 2017). While the findings are not definitive, the exploration of both adaptive and maladaptive eating behaviors is becoming more common to provide a thorough understanding of eating behaviors (Strodl et al., 2020).
The TFEQ includes three maladaptive eating behaviors: cognitive restraint, uncontrolled eating (or disinhibition), and emotional eating (Cappelleri et al., 2009). Cognitive restraint is the degree of conscious control or restriction of diet intake to control body weight or promote weight loss; uncontrolled eating reflects the loss of control in intake and the tendency to eat more than usual; and emotional eating, which has shifted from the initial validation studies of the TFEQ and includes eating in response to (negative) emotions (Cappelleri et al., 2009; de Lauzon et al., 2004). Previous research has identified relationships between maladaptive eating behaviors and diet intake. Restraint was associated with increased diet quality and lower intake of fat (Ard et al., 2006; Contento et al., 2005; de Lauzon et al., 2004; Lawless et al., 2020) or no association (Stevenson, 2017). Uncontrolled eating has been associated with poorer diet quality, including the consumption of fat and salty foods (Bryant et al., 2008; Contento et al., 2005; de Lauzon et al., 2004; Jaakkola et al., 2013; Stevenson, 2017). Emotional eating has been consistently associated with increased intake of energy dense foods, a higher intake of snack foods, and lower diet quality (Bongers et al., 2016; de Lauzon et al., 2004; Lopez-Cepero et al., 2019; Stevenson, 2017; Wallis and Hetherington, 2009).
Intuitive eating, as measured by the Intuitive Eating Scale (IES-2) includes four domains: unconditional permission to eat (UPE), eating for physical rather than emotional reasons (EPR), reliance on internal hunger and satiety cues, and body-food choice congruence (B-FCC) (Tylka and Kroon Van Diest, 2013). UPE reflects the ability to eat when hungry and a lack of labeling foods as forbidden. EPR includes consumption as a response to hunger rather than coping with emotions (e.g. loneliness, anxiety). Reliance on hunger and satiety cues (RHSC) reflects trusting the bodily cues and a reliance on those cues to guide eating behaviors. Lastly, B-FCC measures the alignment of choices with the needs of the body. The relationship between intuitive eating and diet quality in community samples is not conclusive. UPE was negatively correlated with diet quality in men and women, while RHSC was positively associated with diet quality in women only (Horwath et al., 2019). Using the original three-subscale measure of intuitive eating, UPE was associated with reduced intake of fruits, vegetables, and whole grains (Camilleri et al., 2017). EPR was associated with less sweet and high fat foods, and RHSC was associated with more whole grains in women, and a lower consumption of dairy, meat, fish and eggs in women and men.
There have been five intuitive eating interventions that investigated a relationship with diet quality, all of which have excluded men. Three of the five intuitive eating interventions found positive associations between intuitive eating and higher diet quality (Carbonneau et al., 2017; Hawley et al., 2008; Mensinger et al., 2016), while two studies found no significant difference in diet quality (Cole and Horacek, 2010; Leblanc et al., 2012).
Current study
To better understand mechanisms that support diet quality, we explored the relationships between positive and negative body image, maladaptive and adaptive eating behaviors, and their relationship to diet quality after controlling for age and sex in a community sample. Our research questions include:
What are the relationships among body image, eating behavior, and diet quality? Does eating behavior mediate the relationship between body image and diet quality?
We hypothesized positive body image and adaptive eating behaviors would be associated with higher diet quality, and negative body image and maladaptive eating behaviors would be associated with lower diet quality. We also hypothesized that adaptive eating behaviors would mediate the relationship between positive body image and diet quality, while maladaptive eating behaviors would mediate the relationship between negative body image and diet quality.
Methods
Participants and procedures
Adults (18 years and older) living in the United States who completed the first wave of data collection of a larger, longitudinal study assessing the impacts of the COVID-19 pandemic on health behaviors were invited to participate in the current study (Weaver et al., 2021). At Wave 1, we recruited a representative sample (by age, sex, and ethnicity) of 395 participants who were 18 years and older and living in the US using Prolific Academic. Participants were paid $10.50 to complete a second wave of data collection. Data were collected between July 16 and August 1, 2020. Of the 395 participants who completed Wave 1 and were invited to participate, 288 completed the survey and met inclusion criteria including: accurate completion of at least half of the ten attention checks or they did not complete the survey in less than three standard deviations of the mean completion time (Peer et al., 2017). The study was certified as Exempt by the Washington State University Institutional Review Board.
Measures
Demographics
We collected age, sex, ethnicity, marital status, level of education, and household income.
Body image
Negative body image
To assess body dissatisfaction, or the negative evaluation and investment in appearance (Stice, 2002), we used the Body Shape Questionnaire (BSQ-8) (Dowson and Henderson, 2001; Evans and Dolan, 1993). A recent systematic review of measures of body image suggests the BSQ has strong evidence of internal consistency, content validity, structural validity, and moderate evidence for reliability (Kling et al., 2019). To reduce participant burden, we used the eight-item version of the BSQ (Dowson and Henderson, 2001; Evans and Dolan, 1993). Items include “has seeing your reflection made you feel bad about your shape?” and “Have you been particularly self-conscious about your shape when in the company of other people?” Response categories range from 1 (never) to 6 (always) with higher scores indicating higher negative body image (Dowson and Henderson, 2001; Evans and Dolan, 1993). Reliability was good (Cronbach's alpha = 0.93).
Positive body image
We used the functionality appreciation scale (FAS) and body appreciation scale (BAS-2) to assess positive body image. Functionality appreciation is defined as appreciating, respecting, and honoring the body for what it is capable of doing (Alleva et al., 2017). Response categories included a five-point scale from 1 (strongly disagree) to 5 (strongly agree), with higher scores reflecting higher appreciation of body functionality. The FAS includes seven items and is a gender invariant, unidimensional scale with high internal consistency and stability, and has demonstrated criterion, convergent, discriminant, and incremental validity (Alleva et al., 2017). Reliability was consistent with previous research (Cronbach's alpha = 0.92) (Alleva et al., 2017).
Body appreciation is defined as accepting, holding favorable opinions toward, and respecting the body while rejecting media-promoted appearance ideals (Tylka and Wood-Barcalow, 2015). We assessed body appreciation using the BAS-2 (Tylka and Wood-Barcalow, 2015). The BAS-2 is a ten-item unidimensional scale that includes items such as “I respect my body.” Response categories include a five-point scale from 1 (never) to 5 (always), with higher scores reflecting higher body appreciation. Among college and community samples, internal consistency, test-retest reliability, and construct validity were supported for the BAS-2 (Tylka and Wood-Barcalow, 2015). Cronbach's alpha (0.96) was consistent with previous research (Tylka and Wood-Barcalow, 2015).
Eating behaviors
We used the Three Factor Eating Questionnaire (TFEQ-R18) to measure maladaptive eating behaviors, and the IES-2 to measure adaptive eating behaviors.
Three factor eating questionnaire (TFEQ-R18)
The TFEQ-R18 was used to assess uncontrolled eating, cognitive restraint, and emotional eating (de Lauzon et al., 2004; Karlsson et al., 2000). The TFEQ-R18 includes 18 items with response categories ranging from 1 (definitely false) to 4 (definitely true). We averaged items for each of the three subscales with higher scores indicating higher levels of each maladaptive behavior (Karlsson et al., 2000). Studies in adults with obesity indicate internal consistency, and convergent and discriminative validity for the three subscales (Cappelleri et al., 2009; de Lauzon et al., 2004; Karlsson et al., 2000). Cronbach's alpha was acceptable for all three scales: Cognitive restraint (0.81), uncontrolled eating (0.87), emotional eating (0.95).
Intuitive eating scale (IES-2)
The IES-2 includes a total score and four subscales: UPE, EPR, RHSC and B-FCC. The IES-2 includes 23 items with a 5-point response scale (1 = strongly disagree to 5 = strongly agree), with higher scores indicating more intuitive eating behaviors. Psychometric testing of the IES-2 indicated that three-week reliability, construct, discriminant, and incremental validity were upheld in college women and men (Tylka and Kroon Van Diest, 2013). Cronbach's alpha for IES-2 total score as good (0.89) and aligned with previous research, subscale reliabilities calculated for the current sample are included in Table 3.3 (Tylka and Kroon Van Diest, 2013).
Diet quality
We modified the validated dietary screener questionnaire (DSQ) (Thompson et al., 2017) to assess intake over the past week rather than the past month due to the changes in food availability since the COVID-19 pandemic (International Food Information Council, 2020). No other modifications to the questionnaire were made. Responses were converted to estimated intake of dietary components using the scoring procedures provided by the National Cancer Institute (Thompson et al., 2017).
We used the scoring procedures provided by the National Cancer Institute to convert frequency of intake to mean intakes based on age and sex from the National Health and Nutrition Examination Survey (NHANES 2009–2010) (Thompson et al., 2017). Next, we developed an overall measure of diet quality based on scoring from previous publications (Horwath et al., 2019; Mötteli et al., 2017) (see Supplementary Materials for scoring procedures). Participants received one point if their estimated intake was equal to or above the mean intake for their sex: fruit, vegetables, whole grains, and calcium. Participants received one point if their intake of added sugar was equal to or below the mean for their sex. Participants received one point if they consumed less than one serving per week of processed meat (World Cancer Research Fund/American Institute for Cancer Research, 2018). Scores for each dietary component were summed to a measure of diet quality ranging from lower diet quality (0) to higher diet quality (6).
Analysis
We assessed means, standard deviations, missingness, and skewness and kurtosis to determine normality of the data and examined the data for univariate and multivariate outliers (Mahalanobis distance, Cook's distance, and centered leverage values) using SPSS® (Version 26, Chicago, IL). We examined scale reliabilities and bivariate correlations among body image, eating behavior, and diet quality variables. To test the relationships between body image, eating behaviors, and diet quality, we ran a series of hierarchical linear regressions in SPSS. An a priori sample size calculation using G*Power with twelve tested predictor variables based on a middle effect size (f2 = 0.15), power = 0.95 and α = 0.05 resulted in a minimum sample size of 184 participants (Faul et al., 2007). Age and sex were included as covariates as eating behaviors and body image may differ across the lifespan and by sex (Horwath et al., 2019; Keirns and Hawkins, 2019; Kling et al., 2019; Van Dyke and Drinkwater, 2014). Each model included three steps: (1) covariates including: age and sex, (2) body image variables, and (3) eating behavior variables. Our outcome variable was diet quality. Mediation analyzes were conducted using the Sobel test which indicates mediation can occur in the absence of a significant relationship between the independent and dependent variable (Hayes, 2009). The Sobel test includes regression coefficients of the pathway between the independent variable and mediating variable, and mediating variable and dependent variable. To test for mediation, we used the PROCESS Macro in SPSS with a 95% bias-corrected confidence interval with 5000 bootstrap samples to determine if eating behaviors mediated the relationship between body image and diet quality. Age and sex were included as covariates in mediation analyzes. We used the F statistic to assess significance of R2 change to determine if each step improved model fit and a p-value of ≤0.05 to indicate statistical significance.
Results
Demographic data is presented in Table 1. Participants were primarily White (69.4%), an average of 48 years old (SD = 15.40), nearly half women and men, and more than half of the participants were married or in a committed relationship (54.5%). Data were normally distributed. Two cases had a large Mahalanobis distance suggesting the cases were multivariate outliers and were excluded from analyzes. Overall, missingness was not an issue (three participants indicated their sex as “other,” one participant did not include age); missing data were handled using listwise deletion. Bivariate correlations (Table 2) were largely in the expected directions. Diet quality had a small, positive correlation with cognitive restraint, a medium, positive correlation with B-FCC, and a small, negative correlation with UPE.
Sociodemographic characteristics of the sample.
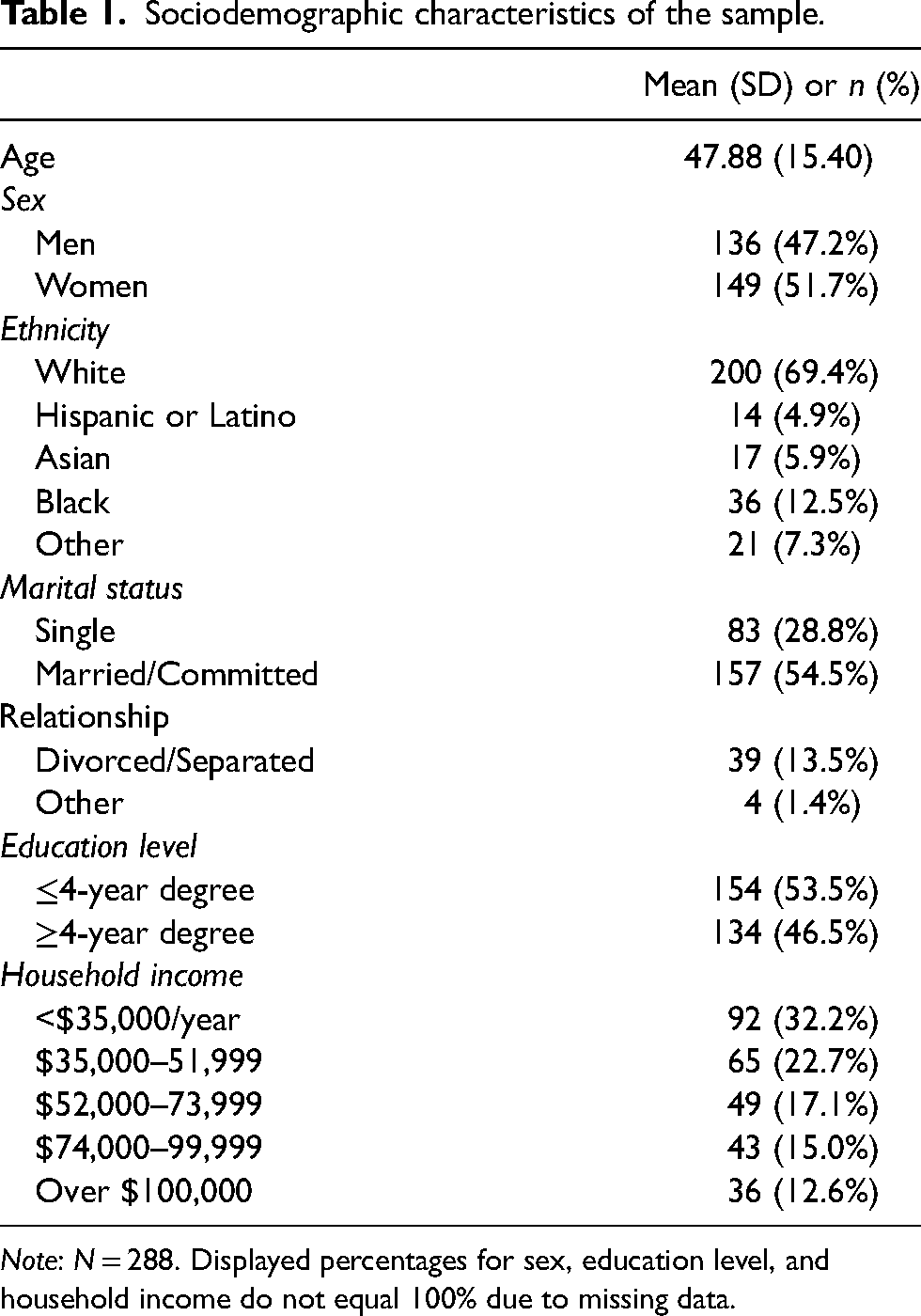
Note: N = 288. Displayed percentages for sex, education level, and household income do not equal 100% due to missing data.
Means, reliabilities, and correlations for body image, eating behaviors, and diet quality.
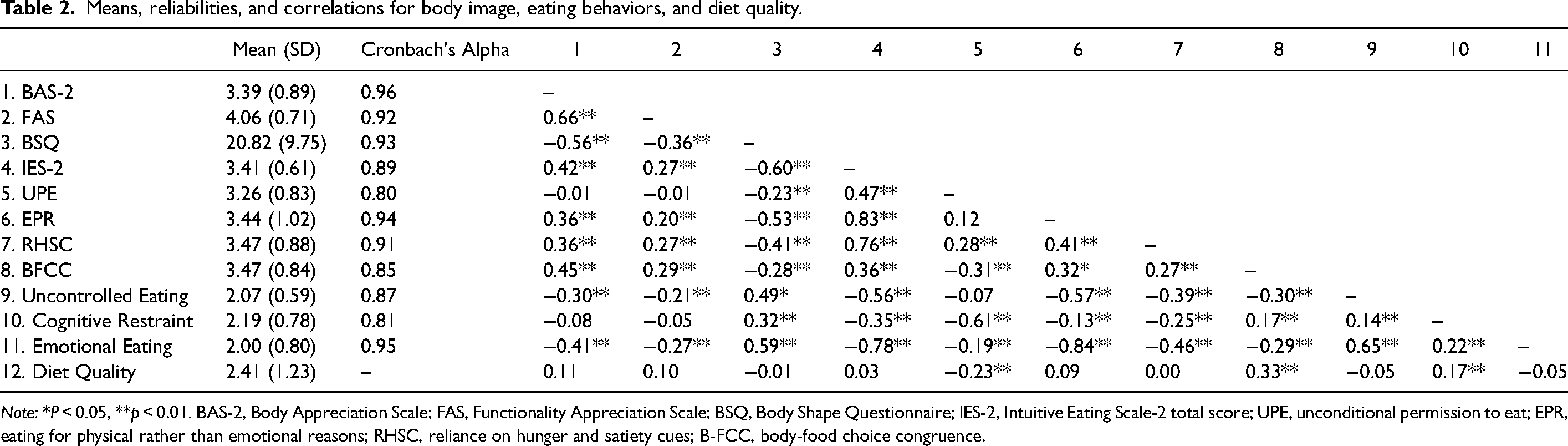
Note: *P < 0.05, **p < 0.01. BAS-2, Body Appreciation Scale; FAS, Functionality Appreciation Scale; BSQ, Body Shape Questionnaire; IES-2, Intuitive Eating Scale-2 total score; UPE, unconditional permission to eat; EPR, eating for physical rather than emotional reasons; RHSC, reliance on hunger and satiety cues; B-FCC, body-food choice congruence.
Results from the hierarchical linear regression are included in Table 3. Due to the large, significant negative correlation between emotional eating and EPR (r = −0.84, p < 0.01), we excluded emotional eating from all regression analyzes.
Associations of body image and eating behavior with diet quality.
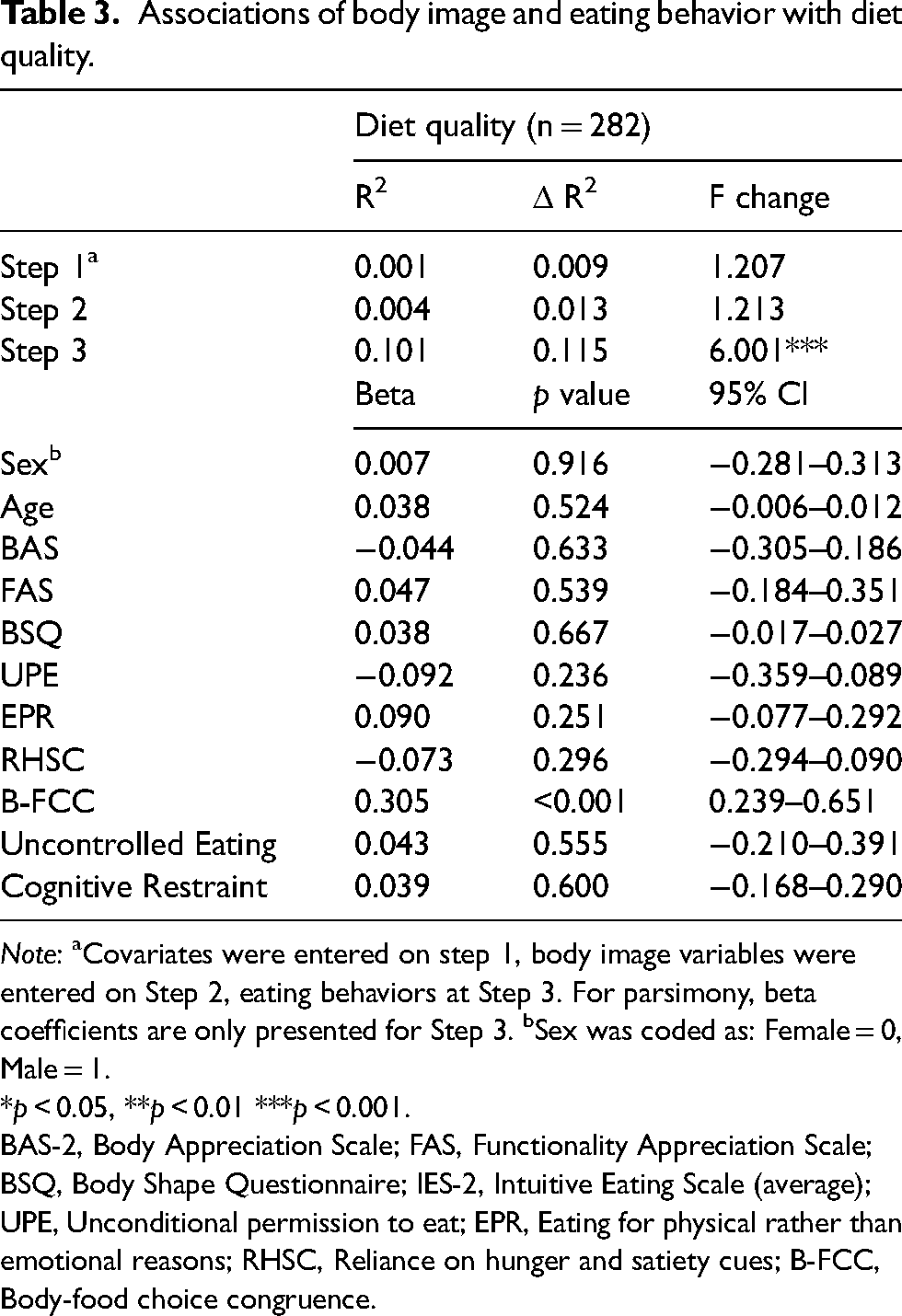
Note: aCovariates were entered on step 1, body image variables were entered on Step 2, eating behaviors at Step 3. For parsimony, beta coefficients are only presented for Step 3. bSex was coded as: Female = 0, Male = 1.
*p < 0.05, **p < 0.01 ***p < 0.001.
BAS-2, Body Appreciation Scale; FAS, Functionality Appreciation Scale; BSQ, Body Shape Questionnaire; IES-2, Intuitive Eating Scale (average); UPE, Unconditional permission to eat; EPR, Eating for physical rather than emotional reasons; RHSC, Reliance on hunger and satiety cues; B-FCC, Body-food choice congruence.
Covariates (age and sex; Step 1) and body image variables (Step 2) were not related to diet quality. After including eating behavior variables (Step 3), 10% of the variance was explained. B-FCC was the only significant variable; as B-FCC increased, so did diet quality. We tested if the relationship between positive and negative body image and diet quality was mediated by B-FCC. After controlling for sex and age, B-FCC mediated the relationships between body appreciation (β = 0.15 CI [0.090, 0.215], functionality appreciation (β = 0.08 CI [0.042, 0.140]), body dissatisfaction (β = −0.10; CI [−0.158, −0.054]) and diet quality.
Discussion
We explored the relationships between positive and negative body image, adaptive and maladaptive eating behaviors, and diet quality. Surprisingly, and contrary to our hypotheses, other than a small, positive correlation between cognitive restraint and diet quality, body image and maladaptive eating behaviors were not associated with diet quality. In alignment with our hypotheses, adaptive eating behaviors were positively associated with diet quality. B-FCC was positively associated with diet quality. Cross-sectional mediation analyzes suggest B-FCC may mediate the relationship between body dissatisfaction, body appreciation, and functionality appreciation with diet quality. While the effect sizes are small, our findings provide preliminary data suggesting body and functionality appreciation may positively influence diet quality while body dissatisfaction may negatively relate to diet quality through B-FCC, rather than having a direct influence on intake. Thus, our findings offer additional support for weight-neutral interventions in community samples.
The indirect effects of body image through B-FCC, along with the strong correlations between positive body image and adaptive eating behavior, and conversely negative body image and maladaptive eating behavior, continue to support the concept of attunement or embodiment described by the Embodied Self Model and previous literature indicating body image is closely related to eating behavior (Avalos and Tylka, 2006; Cook-Cottone, 2015; Stice, 2002). The indirect effects between body image and diet quality suggest positive body image may be relevant in encouraging B-FCC, which promotes diet quality. Alternatively, negative body image may decrease B-FCC and thus decrease diet quality. While we did not find a direct relationship between body image and intake, our findings continue to align with previous research indicating positive body image promotes positive health behaviors (e.g. adaptive eating) (Avalos and Tylka, 2006; Homan and Tylka, 2018).
Our findings suggest continued exploration of adaptive and maladaptive eating behaviors simultaneously. The strong, negative correlation between emotional eating and EPR aligns with previous research suggesting these concepts may be on alternative ends of a single continuum (Barrada et al., 2018; Kerin et al., 2018; van Dyck et al., 2016). Excluding emotional eating, our findings indicate adaptive and maladaptive eating behaviors may be qualitatively different behaviors and have differing relationships with intake. The lack of a relationship between maladaptive eating behaviors and diet quality was surprising. Our findings support previous literature suggesting no association between restraint and intake (Stevenson, 2017). Alternatively, the lack of findings between uncontrolled eating with diet quality are inconsistent with previous research (Bryant et al., 2008; Contento et al., 2005; de Lauzon et al., 2004; Jaakkola et al., 2013; Stevenson, 2017). This may be attributed to our measurement of diet quality. Previous research indicates uncontrolled eating was associated with poorer diet quality, and specifically high fat and salty foods, two foods we did not include in this analysis. As these results contradict previous research, additional research is warranted.
In the development and implementation of approaches to improve diet quality and health, our research provides additional evidence for interventions that promote positive body image and intuitive eating while decreasing negative body image in a community sample. While prior research indicates positive body image and intuitive eating, weight neutral, and/or mindful eating interventions either perform equally or better than traditional weight loss interventions in improving health-related outcomes (Dugmore et al., 2020; Grider et al., 2021; Guest et al., 2019), the majority of intervention research is in women. To improve health and diet quality, it is imperative that body image and intuitive eating interventions include more diverse samples. On the other hand, while our findings indicate that restraint was not associated with higher diet quality, the negative health outcomes associated with restraint including weight cycling, disordered eating, and thus increased mortality suggest transitioning away from interventions that encourage restriction (Arcelus et al., 2011; Field et al., 2004; Garner and Wooley, 1991; Mann et al., 2007; Rzehak et al., 2007; Tomiyama et al., 2013). Considering the multiple benefits of promoting positive body image and intuitive eating on health, and potential harms of encouraging maladaptive eating behaviors, we encourage future preventive and clinical interventions consider promoting adaptive eating behaviors to improve diet quality.
Limitations of this study include the collection of data during the COVID-19 pandemic. In late July 2020, when we collected data, concerns about food availability had decreased (International Food Information Council, 2020) and all states were reopening (Raifman et al., 2020). We used the diet screening questionnaire, which, while a validated measure of intake, only assesses the frequency of intake and does not include amount of food consumed. In addition, we modified this measure to capture intake over the past week rather than month, due to potential changes in access to food during the pandemic. To better assess diet quality, we suggest using alternative measures of diet intake (e.g. multiple 24-h recalls). Lastly, the data collected were self-reported and cross-sectional, limiting the ability to determine directionality or causality. We were able to analyze data from an adequate sample size of individuals from a community population, which supports generalizability. However, the sample was nearly 70% White.
Future research could benefit from qualitative research to describe the relationships between eating behavior and diet quality, longitudinal data collection, and continued testing of the effectiveness of weight-neutral interventions that promote positive body image and adaptive eating behaviors in community samples. While we identified relationships between body image, eating behavior, and dietary intake in a community population, qualitative data could help to explain these relationships, how these relationships may change over the lifespan and further inform preventive interventions that promote diet quality and health. Similarly, longitudinal data collection can help to understand how body image and eating behaviors change over the lifespan. Lastly, as the majority of interventions have excluded men, it is critical that future research include diverse samples to explore the effectiveness of body image and intuitive eating interventions.
Our findings suggest adaptive eating behaviors (e.g. B-FCC) may be an important mechanism to directly encourage diet quality in community samples. Interventions to support diet quality may benefit from promoting positive body image and reducing negative body image, leading to higher B-FCC. The lack of association between maladaptive eating behaviors and diet quality suggest restriction may not be effective in encouraging diet quality.
Supplemental Material
sj-docx-1-nah-10.1177_02601060221090696 - Supplemental material for Associations between body image, eating behavior, and diet quality
Supplemental material, sj-docx-1-nah-10.1177_02601060221090696 for Associations between body image, eating behavior, and diet quality by Alexandra Malia Jackson, Louise Parker, Yoshie Sano, Anne E Cox and Jane Lanigan in Nutrition and Health
Footnotes
Acknowledgements
The authors wish to thank the study participants and members of the Washington State University COVID-19 and health behaviors study team including Alana Anderson, Linda Eddy, Anaderi Iniguez, Thomas G. Power, Raven Weaver, and Elizabeth Weybright for their support.
Author contributions
AMJ and JL designed the study and were responsible for data collection. AMJ analyzed the data. All authors participated in writing the paper, and all authors read and approved the final manuscript.
Availability of data and materials:
Due to current approvals from the Institutional Review Board, we are unable to share original data at this time. If data are requested, we will revise our application to share data requested. Study and analysis materials including questionnaires and analysis procedures are available upon request.
Consent for publication
All authors have reviewed the content of this manuscript and approve the submission of this manuscript for review. This manuscript has not been published or submitted for publication elsewhere.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was certified as Exempt by the Washington State University Institutional Review Board (IRB# 18251-001). All participants provided written informed consent prior to starting the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Washington State University Vancouver, Washington State University (Vancouver Mini-grant, Collaborative Grant, Nelson McLeod Scholarship).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.