
Abstract
INTRODUCTION
Resting metabolic rate (RMR) is a single value (kcal/day) that integrates the energy expenditure of all of the body's organs and tissues and it is typically assessed indirectly through assessment of respiratory gases (Heymsfield et al., 2021). Metabolic stressors can affect RMR status (Heymsfield et al., 2021) and energy deficit and low energy availability (Areta et al., 2021) may result in adaptive thermogenesis and suppression of normal RMR (Müller and Bosy-Westphal, 2013; Staal et al., 2018; Strock et al., 2019). The magnitude of RMR suppression also appears to be proportional to the degree of energy conservation (De Souza et al., 2007). Therefore, monitoring of RMR longitudinally provides a practical parameter for research and clinical practice to detect suppression of RMR (Langan-Evans et al., 2021) and its severity (De Souza et al., 2007).
To accurately detect longitudinal changes in RMR, however, it is essential to quantify measurement error to determine reliability of measurements. Typically, the error of measurement of RMR using different equipment and methodology, expressed coefficient of variation, falls between 4 and 8% (Bone and Burke, 2018; Cooper et al., 2009; Roffey et al., 2006; Woods et al., 2016). The Vyntus CPX system is a new automated indirect calorimetry system that takes the place of the popular (but now discontinued) Oxycon-Pro by the same manufacturer (Groepenhoff et al., 2017), and no assessment of reliability of RMR has been reported on this equipment.
Moreover, comparisons of RMR against predictive RMR formulas represent potential markers of RMR suppression when RMRmeasured/RMRpredicted (RMRratio) is under a certain threshold value (Staal et al., 2018; Strock et al., 2019). Prediction equations have utility in clinical settings, as allow estimation of resting energy needs of individuals in normal conditions, but the accuracy of these equations is variable and some equations are more suited to different populations (Balci et al., 2021; Flack et al., 2016; Schofield et al., 2019), which, in turn, can impact RMRratio. Moreover, the accuracy of metabolic carts to measure RMR can be variable (Cooper et al., 2009; Kennedy et al., 2014), ensuring RMRratio may also be impacted by the selection of equipment. Nonetheless, how the measurements provided by this equipment compare to popular RMR predictive formulas on a group of healthy individuals, is unknown.
Finally, the reliability of measurements have also shown to be affected by test duration. Shorter tests make them more practical and suitable for a wider range of situations optimising use of limited time and equipment, but measurement artifacts —which can be reflected in a disturbance of respiratory gases stability (Feurer and Mullen, 1986) — can have a heavier weight on the extrapolation to the daily energy expenditure and also affect reliability of measurement (Leff et al., 1987). We have observed previously in pilot testing (Areta et al., 2020) that in healthy population in well-controlled conditions a short protocol yielded comparable levels of reliability to a longer protocol, but we have not assessed this systematically with this new equipment.
With this in mind, the aims of this study were threefold: 1st- to establish the reliability of the Vyntus CPX for RMR assessment following best practice, also addressing the effect of within day variability, 2nd- to compare the measured values against those of common predictive formulas in a young healthy population, 3rd- To assess the reliability of a shorter RMR assessment protocol.
METHODS
Experimental protocol
An outline of the experimental protocol is shown in Figure 1. Briefly, 26 young healthy participants with no known diseases, use of any medication or any dietary supplement that may affect RMR measurements (12 females, 14 males) were recruited (Table 1) to complete 3 RMR tests on two consecutive days. Half of the participants completed two tests on day one and one test on day two, and this was counterbalanced for the other half of the participants. Measuring twice on the same day and once on consecutive days allowed to investigate variation in measurement during the morning and the effect of measuring at different times in the morning on separate days. This study was coupled with a DXA reliability study (results not presented here) and participants were required to walk ∼250 m after each RMR test towards the DXA equipment and return afterwards for a second RMR assessment when relevant. This is approximately the same distance that the participants had to walk prior to the first RMR each morning from parking lot/public transport stop to our laboratory. Therefore, the amount and intensity of physical activity immediately prior to the test was kept to a minimum and comparable for all assessments.
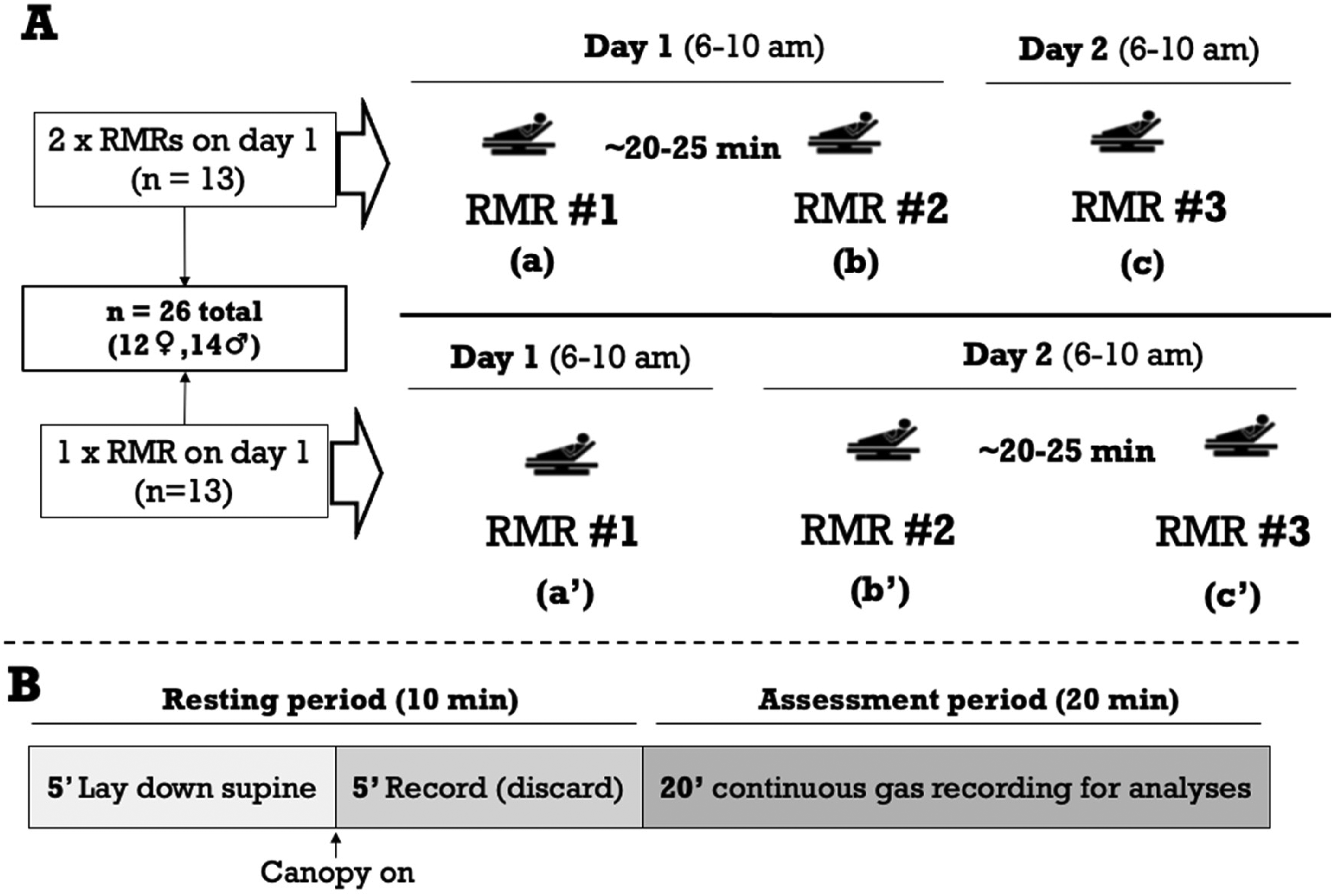
Experimental protocol (A), and details of order of events and duration the RMR assessment (B). A total of 26 young and healthy participants (12 females, 14 males) completed 3 RMR assessments each on two consecutive days. Half of the individuals completed two assessments on the first day and one on the second day, and this was counterbalanced for the other half. We performed pairwise comparisons between days, at the same time (a-c and a’-b’), between days, at different times (b-c and c’-a’), and within days, consecutive measurements (a-b and b’-c’).
Participants characteristics.
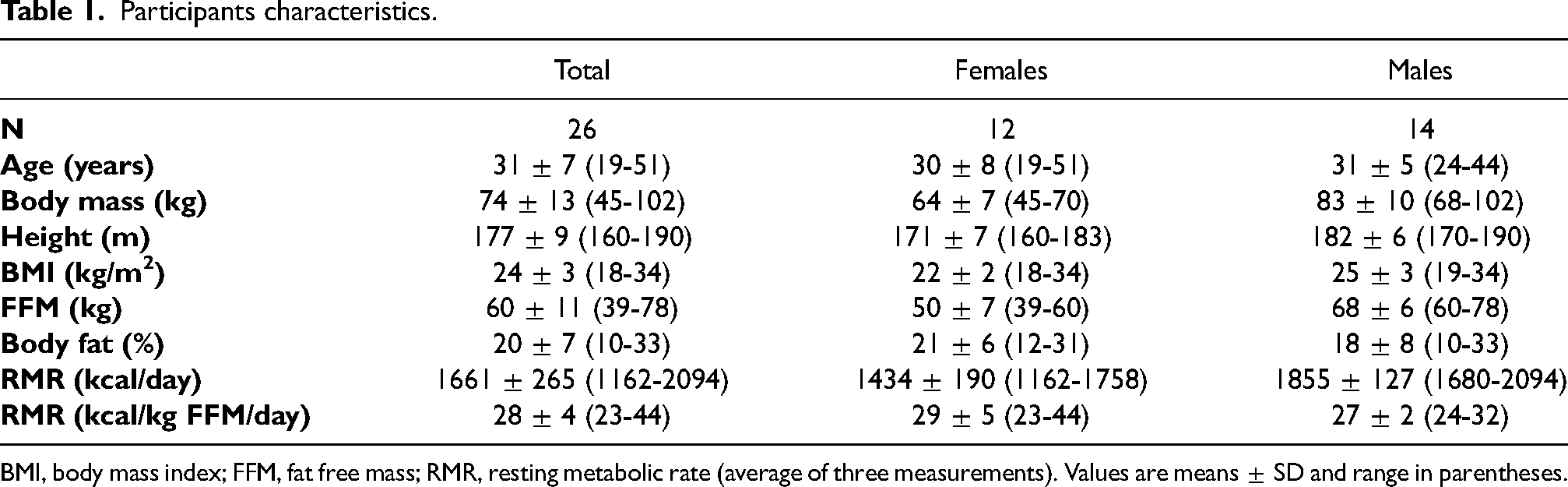
BMI, body mass index; FFM, fat free mass; RMR, resting metabolic rate (average of three measurements). Values are means ± SD and range in parentheses.
Ethical approval
The experimental protocol was approved the Regional Ethics Committee south-east of Norway under reference number 2017/2160 REK sør-øst D, in accordance with the declaration of Helsinki.
Dietary and exercise control
The day prior to the first assessment, participants were required to document all food and fluid consumed as well as physical activity. Structured exercise was allowed before 12 noon the day prior to testing. Participants were instructed to reproduce any food, fluid and physical activity in the 24 hs prior to day 1 and 2. Participants remained fasted after the last meal of the day prior to RMR measurements until after the measurements. On the day of assessment, participants were instructed to arrive at the laboratory by means of public transport or car and minimise any form of locomotion/physical activity. Participants remained fasted for the tests, and refrained from consuming any form of caffeine, nicotine and water on the morning of the tests.
Body composition assessment
All DXA scans were undertaken in the total body mode on a narrow fan beam DXA scanner scanner (Lunar iDXA, GE Healthcare, Madison, WI) with analysis performed using GE enCORE v.13.60 software (GE Healthcare). The scans were performed according to a protocol developed that emphasises a consistent positioning of subjects on the DXA scanning bed (Nana et al., 2012).
RMR assessment
The RMR tests were undertaken between 6 and 10 am each day via indirect calorimetry using a VyntusTM CPX metabolic cart (Vyaire, Mettawa, Illinois, USA) set up with a ventilated hood. The equipment was calibrated prior to each test as per manufacturer's directions using standard gases. Tests were carried in a dedicated room under standard laboratory conditions at 21–22 °C, and lasted a total of 30 min. Participants remained supine throughout, with the canopy positioned after laying down for 5 min, and data capture initiated immediately thereafter for 25 min, with the first 5 min of data discarded and remaining 20 min used for subsequent analysis. Participants were instructed to remain still but not fall asleep while a researcher remained present for the duration of each test The lights were dimmed, and noise kept to a minimum throughout all tests. The values of
Comparison against predictive equations
We compared our RMR measured values for each individual with those estimated from the following predictive formulas: Nelson equation 25.8 x FFM (kg) + 4.04 x fat mass (kg) (Nelson et al., 1992), Mifflin-St Jeor equation: 9.99 x body mass (kg) + 6.25 x height (m) – 4.92 x age + 166 x sex (men, 1; women, 0) – 161 (Mifflin et al., 1990), Harris-Benedict: men: 66.47 + 13.75 x body mass (kg) + 5 x height (m) – 6.76 x age (y), women: 655.1 + 9.56 x body mass (kg) + 1.85 x height (m) – 4.68 x age (y) (Harris and Benedict, 1918), Cunningham, 1980 equation: 500 + 22 x lean body mass (kg) (Cunningham, 1980) (where lean body mass is defined as total body mass, minus fat free mass, minus bone mass), Cunningham, 1991 equation: 370 + 21.6 x Fat Free Mass (Cunningham, 1991), and a DXA-derived estimation based on contribution of 5 components (Hayes et al., 2002).
Twenty-minute protocol exploration
Given that available time in clinical practice is often limited, we used our data set to explore the potential of undertaking a test incorporating 5 min of supine rest, and 15 min RMR measurement with the first 5 min of gases discarded and the remaining 10 min of data analysed. We assessed reliability for same time between days of this shorter twenty-minute protocol as well as compared the results against the full thirty-minute protocol described above (and in Figure 1).
Statistical analysis
Reliability of measurements between and within day were evaluated through determination of systematic bias (mean change), typical error of measurement and intraclass correlation via an online available tool (http://sportsci.org/2015/ValidRely.htm) following guidelines outlined by Hopkins (Hopkins, 2015). Comparisons were performed pairwise for between days, at the same time (BDST), between days, at different times (BDDT) and within same day, consecutive measurements (WDCM; see Figure 1 for further details). Pearson correlation tests were undertaken to determine association between the full-length 30 min protocol and the shorter 20 min protocol. Data were analysed in Microsoft Excel (Microsoft Corporation, Washington, USA). Data were tested for normality prior to analysis. Paired t-tests were used to compare predicted versus measured RMR values and threshold for statistically significant difference was set at p = 0.05. Data are reported as means ± SDs, and 95% confidence limits (CL) detailed where relevant.
RESULTS
Reliability of measurements
The 20 min of analysed data showed low variability in respiratory gasses within measurements (CV% 5.2, 6.6 and 3.2 for

Bland-Altman plots of resting metabolic rate values from between-day comparisons, same time (ST; A), within-day comparisons, different times (B) and between-day (DD), different times (C). Dotted lines are 95% confidence limits.
Parameters of reliability for comparisons between consecutive days at the same time, within days for consecutive measurements, and between days at different times.
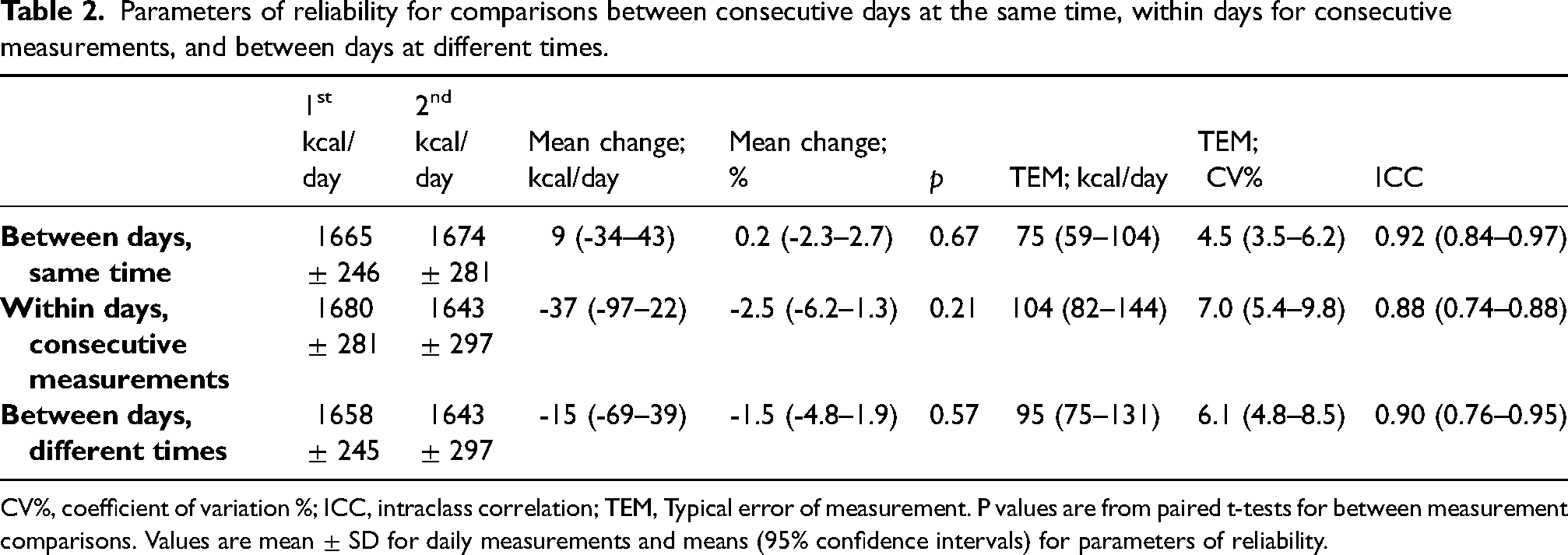
CV%, coefficient of variation %; ICC, intraclass correlation; TEM, Typical error of measurement. P values are from paired t-tests for between measurement comparisons. Values are mean ± SD for daily measurements and means (95% confidence intervals) for parameters of reliability.
Comparison against predictive equations
Except for the Cunningham1980 equation (Cunningham, 1980) and DXA-predicted equation (Hayes et al., 2002), the other equations’ predictive values were not different from measured values for the whole cohort, or amongst females and males (Table 3). The Cunningham1980 equation (Cunningham, 1980) predicted values were on average ∼5% higher, resulting in a RMRratio of 0.95 ± 0.11 (p = 0.01) for the whole cohort, which did not reach statistically significant difference in females 0.93 ± 0.14 (p = 0.08) or males 0.95 ± 0.05 (p = 0.07). The DXA-predicted equation predicted values ∼4% higher resulting in a RMRratio of 0.96 ± 0.13 (p = 0.03), seemingly from higher value in males (RMRratio 0.94 ± 0.07, p = 0.04) and not in females (RMRratio 0.99 ± 0.16, p = 0.28).
Comparison of measured resting metabolic rate against predictive equations.
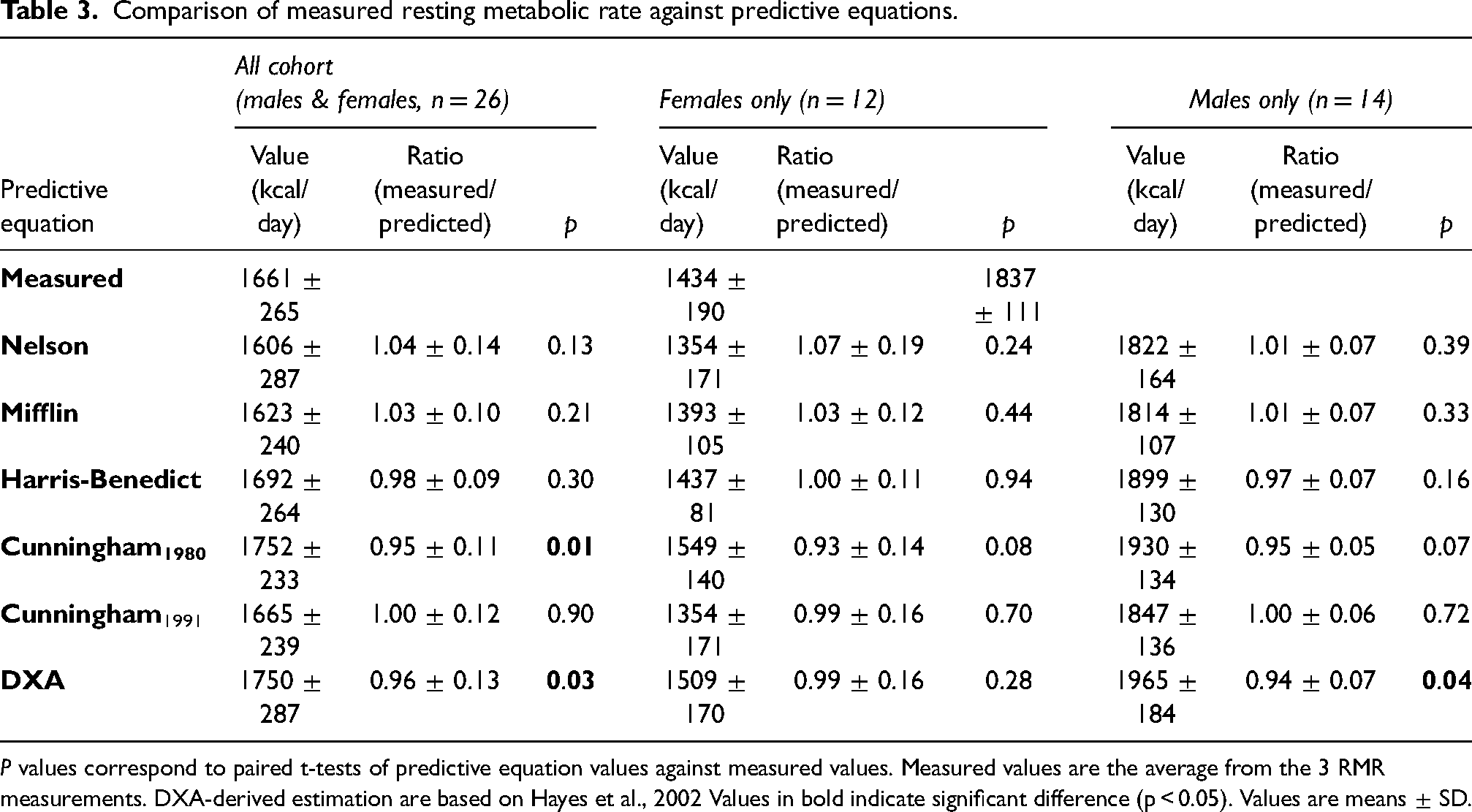
P values correspond to paired t-tests of predictive equation values against measured values. Measured values are the average from the 3 RMR measurements. DXA-derived estimation are based on Hayes et al., 2002 Values in bold indicate significant difference (p < 0.05). Values are means ± SD.
Twenty-minute protocol assessment
The shorter protocol showed excellent reliability, comparable to that of the 30-min protocol BDST (Table 2), with a change in mean (95% CLs) of 2.7 (-40.2 — 45.5) kcal/day or 0.1 (-2.5 — 2.3) %, intraclass correlation of 0.93 (0.85 — 0.97) and typical error of measurement of 4.3 (3.3 — 5.9)%. The 10-min analysed data of the shorter protocol also showed low variability in respiratory gases within measurements (CV% 4.8, 6.3 and 2.9 for
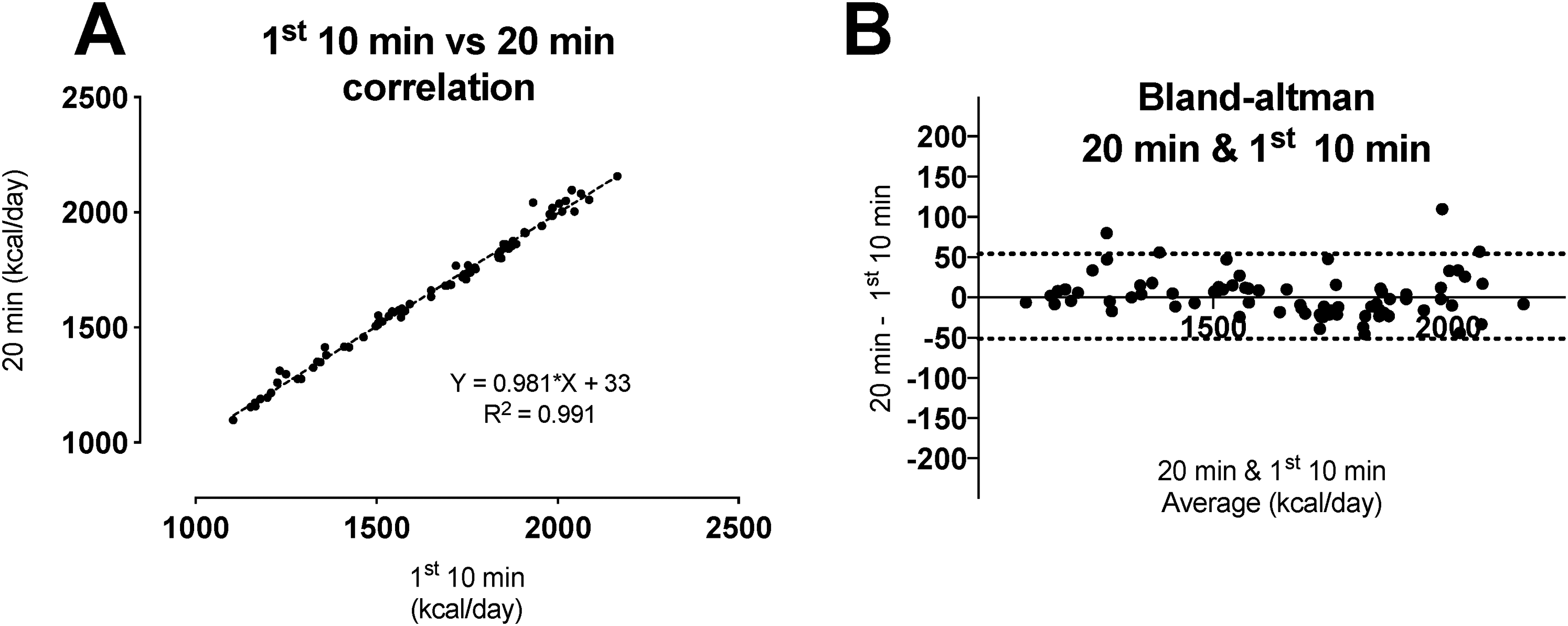
Correlation between 1st 10 min vs 20 min of measurement (A) and respective bland-altman plot (B, dotted lines are 95% confidence limits).
DISCUSSION
The main findings of this study established 1) The reliability of the Vyntus CPX system for measurements of RMR in a cohort of young healthy adults; 2) That parameters of reliability are better when conducted on separate days at the same time compared to separate days at different times; 3) That the measured results are comparable to predictive values from the formulas of Nelson, Mifflin and Harris-Benedict, but lower than that of the Cunningham1980 formula and a DXA-derived formula, and; 4) A 20-min RMR protocol yields no different results from a 30-min RMR protocol and is as reliable. To the best of our knowledge, this is the first study systematically investigating the reliability of the Vyntus CPX system for RMR measurements and comparing these results against predictive equations.
The reliability we report for the Vyntus CPX system is in line with what has previously been reported in the literature using a variety of systems and protocols. The typical error of measurement reported herein for between day same time comparison (Table 2) is comparable to that of other studies assessing the reliability using slightly different methodologies and systems like ParvoMedics TrueOne 2400 by Woods et al. (2 × 10 min gas analysis, Hans-Rudolph mouth piece, CV 6.3%) (Woods et al., 2016) and Cooper et al. (2–10 min gas analysis, ventilated canopy, CV 4.8%) (Cooper et al., 2009), Deltatrac II (10 min gas analysis, ventilated canopy, CV 5.3%) (Roffey et al., 2006), Moxus Modular (10 min gas analysis, Hans-Rudolph mouthpiece, CV 7.3%) (Roffey et al., 2006), Douglas bags by Woods et al. (2 × 10 min gas analysis, Hans-Rudolph mouthpiece, CV 6.6%) (Woods et al., 2016), and by Bone & Burke (2 × 10 min gas analysis, Hans-Rudolph mouthpiece, inpatient CV 4.9%, outpatient inpatient CV 5.9%) (Bone and Burke, 2018). This suggests that the reliability of the Vyntus CPX system is comparable to other widely used equipment for assessment of RMR in research and clinical practice. Importantly, the system reports similar reliability compared to the Douglas Bags method which is typically used as a criterion for validation of respiratory measurements (Bone and Burke, 2018; Woods et al., 2016; Wüst et al., 2008). Though we were unable to compare our data against first principles, due to the nature of the methodology (i.e. ventilated hood), and we are unaware of other studies of measuring validity of the Vyntus CPX, our measures show the equipment has an in inter-day reliability comparable of other equipment previously investigated.
We further investigated whether there would be diurnal variations when measured in the morning at different times, separated by ∼30 min. In clinical practice, ∼30 min time difference between measurements on different days are not uncommon and we were unsure whether this would affect reliability, even under the measurement are performed in standardised conditions. Though research suggests that within-day variations of RMR do not result in significant differences (Leff et al., 1987; Weststrate et al., 1989), detailed effects of measuring RMR in the morning at different times on reliability were unknown to us. Our results show no statistically significantly differences at different times on consecutive measurements or in different days (Table 2), but suggest that when conducting RMR measurements on separate days, performing them at the same time of the day yields more reliable results.
Comparison of predicted versus measured RMR (RMRratio) values is an approach that is used to determine the presence of RMR suppression following adaptive thermogenesis and as a key clinical sign of the ‘relative energy deficiency in sport’ syndrome and the ‘female athlete triad’ condition (Staal et al., 2018; Strock et al., 2019), and normal values of RMRratio for the Vyntus CPX have not been established. Typically, a threshold of 0.9 measured/predicted RMR (RMRratio) is considered to determine if an individual's RMR is suppressed as a consequence of chronic low energy availability (LEA) and adaptive thermogenesis in this population in females, though an appropriate cut off in males remains to be confirmed (Staal et al., 2018; Strock et al., 2019). Beyond the applicability of different formulas for different populations (Schofield et al., 2019), the use of different formulas has been found to be an important factor in determining which individuals fall under this threshold (Staal et al., 2018; Strock et al., 2019), but normal values with the use of this equipment and in this population have not been established. Our comparison showed no differences against the Nelson, Mifflin, Harris-Benedict and Cunningham1991 equations but reported lower values than the Cunningham1980 and DXA-derived equations, which is similar to findings reported by others using different metabolic systems and different predictive equations (Staal et al., 2018; Strock et al., 2019).
A brief overview of relevant research shows that Cunningham1980 equation tends to result in higher predictive values than the measured values (Balci et al., 2021; Flack et al., 2016; Staal et al., 2018; Strock et al., 2019), Cunningham1991 closely matching the measured values (Strock et al., 2019), Harris-Benedict shows typically to be closer to the measured (Balci et al., 2021; Flack et al., 2016; Staal et al., 2018; Strock et al., 2019) and Nelson tends to be lower (Balci et al., 2021; Flack et al., 2016). Different to us, prior comparisons using DXA-derived RMR showed close predictions (Koehler et al., 2016; Strock et al., 2019) but these studies were on ovulatory exercising women but did not assess RMR in men. All in all, the RMR values determined with the current methodology and equipment are in accordance with that reported in similar populations, providing support to the use of this equipment as a useful tool for assessment of RMR following best-practice in data collection.
We must acknowledge that we did not assess other markers of energy preservation to cross-check against RMR measurements and we have no means to unequivocally prove that these individuals had not undergone adaptive thermogenesis Additionally, phase of menstrual cycle has been shown to result in a small but significant increase of RMR during the luteal phase compared to the follicular phase (Benton et al., 2020) and use of contraceptive pills can also result in a small reduction in RMR (Diffey et al., 1997). We did not control or record the status of these, however the impact of these variables on data from our female volunteers was considered to be negligible, given data capture occurred over approximately a 24 h period. Our findings, as those of others (Staal et al., 2018; Strock et al., 2019), call for caution when using predictive formulas to determine likelihood of RMR being suppressed when using this —or other— system, and further research is needed to establish definite cut-off values for different sexes and populations.
Finally, given that it is unclear for how long respiratory gases should be collected to achieve reliable RMR measurements (Compher et al., 2006; Fullmer et al., 2015), we explored how shortening the data collection protocol would affect the measurements or reliability of measurements compared to the longer, more reliable, between-days same time measurement (Table 2). Shortening the measurement period from 20 to 10 min (total assessment time 20 min, when including resting and discarded data periods), resulted in a time-efficient protocol that was not different in absolute daily energy expenditure values and resulted in very similar values for all parameters of reliability.
In conclusion, our findings show that 1) the Vyntus CPX is a reliable equipment for RMR measurements when measurements are conducted in standardised conditions with healthy population, 2) between-day measurements at the same time show better absolute measures of reliability, 3) the Cunningham1980 and DXA-derived RMR formulas overestimate RMR compared to measured values in young healthy active population, and 4) a 20-min protocol yields comparable results that are as reliable as those of a 30-min protocol for RMR
Footnotes
Acknowledgements
The authors want to thank all participants for their time and commitment to the study demands.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Consent and ethical approval were not needed for the present manuscript.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.