
Abstract
‘For after all, the best thing one can do when it is raining is, let it rain.’ (Longfellow, 1906)
Mental health conditions, including depression, anxiety, and stress, affect a sizable proportion of university students. Yet, little is known regarding the incidence of mental health issues among Indian university students. These mental health issues are generally caused by a range of factors, including academic demands, interpersonal connections (Steptoe, 2007), future prospects, competitive exams, peer pressure, and professional considerations (Beiter et al., 2015). One of the most important mental health problems impacting a large population across India and the world is depression, leading to physical diseases, suicidal thoughts, and suicide, among other negative outcomes (Gururaj et al., 2016). According to the NCRB Report, 2021, the two age groups most susceptible to suicide were between 18 and 30 and 30 and 44. Suicide rates in both age categories were 34.5% and 31.7%, respectively. Family issues (3,233 victims), romantic relationships (1,495 victims), and illness (1,408 victims) were the three leading factors in suicides below 18 years of age, while the victims that were either students or unemployed made up 8.0% (13,089 victims) and 8.4% (13,714 victims) of all suicides, respectively. The objectives of this study were to understand and add to the body of knowledge on the role of mindfulness concerning depression, anxiety, and stress amongst university students; the role of mindfulness concerning avoidant behaviours amongst university students; and the mediating role of acceptance in the relationship between mindfulness and depression, anxiety, and stress amongst university students. The results of the study revealed that depression, experiential avoidance, and mindfulness are all strongly and negatively connected. The study discovered a strong correlation between experiential avoidance and depression, anxiety, and stress (psychological distress). Mindfulness had a considerable impact on the mediator, experiential avoidance, which was postulated.
A significant number of university students suffer from various mental health challenges, such as depression, anxiety or moderate to extreme stress. However, not much is known about the prevalence of mental health challenges among university students in India. Broadly, these mental health challenges stem from a variety of factors, such as academic obligations, interpersonal relationships (Steptoe, 2007), future prospects, competitive examinations, peer pressure, and career considerations (Beiter et al., 2015). As a result, the young population studying in various universities finds themselves vulnerable to depression, anxiety, and stress. Depression has been reported as one of the most serious mental health challenges globally and in India, which affects a large segment of the population and may have multiple adverse consequences, such as physical ailments, suicidal thoughts, and suicide (Gururaj et al., 2016). Thus, it is prudent to identify symptoms at an early stage and take necessary precautionary measures. Earlier studies (Judd et al., 2000) have reported that concerns like loss of function and psychological distress can be significantly reduced if identified at an early stage (Judd et al., 1998; Zajecka, 2013) through measures such as identifying mood disorder (McClung, 2007), sleep pattern, eating disorder (Lee et al., 2014; Lazarevich et al., 2013), and anxiety (Bayram & Bilgel, 2008; Eisenberg et al., 2007). Experiential avoidance was one of the coping strategies adopted in several studies (Gross & John, 2003; Hayes et al., 1996; Kortte et al., 2009; White et al., 2006) to deal with mental health issues such as depression and those arising from chronic disease or prolonged illness where a person is unwilling to be in touch with disturbing private experiences and take measures to change these negative experiences, even if this alteration proves harmful (Hayes et al., 2004). Individuals may indulge in practices like thought suppression or experiential avoidance to escape from undesired experiences. They may attempt to interrupt emotional processing with the consideration that it can be helpful while they unconsciously reinforce avoidant behaviour (Abramowitz et al., 2001; Campbell-Sills et al., 2006; Chapman et al., 2006; Wegner & Zanakos, 1994; Wenzlaff & Wegner, 2000); however, this has negative consequences.
Experiential avoidance is a negatively reinforced strategy or response tendency that aims to reduce or end a particularly distressing experience and is maintained through escape conditioning (Chapman et al., 2006). On the other hand, acceptance means wilfully accepting both positive and negative experiences without any intention to avoid them (Hayes, 2004). Being aware, non-judgmental, and accepting are the quintessential attributes of being mindful. Due to such attributes, mindfulness has received noteworthy attention in the literature concerning mental health, management, psychology, healthcare, and the like over the past couple of years. Recent research demonstrates that mindfulness practices negatively relate to psychological symptoms like depression, anxiety or stress (Baer et al., 2006; Brown & Ryan, 2003) and have helped those suffering from emotional disorders (Goldin & Gross, 2010; Grossman et al., 2004; Hofmann et al., 2010). Research studies have provided evidence that cultivating mindfulness helps enhance acceptance and reduce avoidant coping strategies (Hayes, 2004; Schure et al., 2008).
A representative sample survey conducted by the Government of India (National Mental Health Survey, 2015–2016) found that one in twenty people in India suffers from depression. 1.3% of respondents from the primary education group were found vulnerable to either suicide ideation or suicide. The study found a prevalence of mental morbidity among the productive age group; 7.5% in the age group of 18–29 years and 14.6% in the 30–39 years age group (Gururaj et al., 2016). According to the National Crime Records Bureau Report of 2021 (NCRB Report, 2019–2021), the two age groups that were most susceptible to suicide were those between 18 and 30 and 30 and 44. Suicide rates in both age categories were 34.5% and 31.7%, respectively. Family issues (3,233 victims), romantic relationships (1,495 victims), and illness (1,408 victims) were the three leading factors in suicides below 18 years of age while the victims who were either students or unemployed made up 8.0% (13,089 victims) and 8.4% (13,714 victims) of all suicides, respectively.
While studies have been conducted for university-level students in the West, a review of the extant literature exhibited an absence of studies in the Indian context related to the variables of interest such as acceptance, mindfulness, and depression among undergraduate and postgraduate students.
The present study aims to contribute to the literature in the following three ways: (a) examine the role of mindfulness regarding depression, anxiety, and stress among university students, (b) examine the role of mindfulness concerning avoidant strategies among university students, and (c) examine the mediating role of acceptance in the relationship between mindfulness and depression, anxiety and stress among university students. Empirical studies in developing economies related to these constructs, including the Indian subcontinent, is of relevance due to two important factors: (a) India is home to a sizeable number of the world’s population, (ii) the empirical findings from developed nations, where the government-sponsored social security system is in prevalence, may not relate to the context of developing nations (Burgess & Steenkamp, 2006). Thus, the outcomes from this study will help understand the role of mindfulness and experiential acceptance in reducing depression, stress, and anxiety with special reference to university students. It will also pave the way for future research related to university students in India.
RESEARCH HYPOTHESES AND CONCEPTUAL FRAMEWORK
The psychological health of an individual is determined by its detrimental and positive dimensions. In this study, we considered the detrimental dimensions as depression, anxiety, and stress; while the positive dimensions were acceptance, psychological flexibility, and mindfulness. Subsequently, the choice of instruments to measure these constructs is guided by the results obtained from the previous studies. In previous studies, these scales have been used to understand the role of mindfulness, experiential avoidance, and psychological flexibility (Hayes et al., 2004; Leahy, 2007; Roemer & Orsillo, 2003) and their impact on behaviour, emotions, and experiences (Arch & Craske, 2006; Chambers, et al., 2009; Hayes et al., 1996; Hofmann, et al., 2010; Jha, et al., 2010; Leahy, 2002; Mitmansgruber et al., 2009).
One common phenomenon related to depression is avoidant behaviour to cope when suffering (Iwamitsu et al., 2003). In addition to behavioural avoidance, which has been researched extensively, experiential avoidance is now being widely researched, especially to shape people’s emotional wellbeing (Hayes et al., 1996; Hayes et al., 1999). In a meta-analysis of 32 studies which comprised 62 correlations between experiential avoidance and psychological outcomes, it was found that negative effects such as depression, increased hopelessness, negative feelings, low levels of spiritual wellbeing were associated with greater experiential avoidance (Hayes et al., 2006; Kortte et al., 2009).
Dispositional Mindfulness
Mindfulness, during the past couple of years, has emerged as a powerful remedy to mental health challenges for a wide range of populations across cultures. Studies on mindfulness have obtained a significant role, majorly because of its psychotherapeutic benefits (Valerio, 2016). Mindfulness owes its roots to Buddhist philosophy and other introspective traditions where much attention is given to conscious attention and awareness, which are actively cultivated as well (Brown & Ryan, 2003). It was primarily used to treat terminally ill patients. However, mindfulness practices have acquired widespread prominence, especially in western countries and a significant number of populations have gained from its positive psychological and physical outcomes (Shapiro & Schwartz, 2000), such as a reduction in depression, and anxiety (Hofmann et al., 2010), a reduction in stress levels (Khoury et al., 2015), improved attention and memory (Jha et al., 2007; Kilpatrick et al., 2011), improved immune functions (Davidson et al., 2003), an increase in empathy and self-compassion (Chiesa & Serretti, 2009; Evans et al., 2018). According to Brown and Ryan (2003), mindfulness may improve psychological wellbeing due to its association with optimal moment-to-moment experiences. Mindfulness is defined as the state of being attentive to and aware of current events. Mindfulness facilitates moment-to-moment awareness in a non-judgmental manner and has both state and trait-like qualities (Brown & Ryan, 2003; Kabat-Zinn, 1994). Trait quality is defined as between-persons and their tendency to act in a typical way, whereas state quality is within-person (Reis et al., 2000). Mindfulness practice encourages an attitude of acceptance allowing for attention towards physical sensations, feelings, and thoughts, without judging one’s experience, disengaging individuals from automatic thoughts, hence ensuring informed and self-endorsed behavioural regulation, something which has long been associated with the enhancement of wellbeing and happiness (Brown & Ryan, 2003; Ryan & Deci, 2000). Research has proved that cultivating mindfulness through various mindfulness meditation practices aids in a variety of wellbeing outcomes and positively affects psychological and physical health in general and clinical populations (Baer, 2003; Grossman et al., 2004;). Since mindfulness has several proven benefits on emotional disorders, psychological wellbeing, and psychological flexibility, there has been a growing interest in areas such as experiential acceptance, experiential avoidance, stress, anxiety, and depression (Hayes, et al. 2004; Leahy, 2007; Roemer & Orsillo, 2003). These are complex processes that have been studied so we may understand their relationship with emotions, behaviour, and experience (Arch & Craske, 2006; Chambers et al., 2009; Hayes et al., 1996; Hofmann et al., 2010; Jha et al., 2010) and have been found to be beneficial in psychological treatments through mindfulness interventions (Blackledge & Hayes, 2001; Gupta & Kumar, 2021; Hayes et al., 1999, Leahy et al., 2011; Roemer et al., 2009;).
The natural capacity to inhabit attitude is described as dispositional mindfulness (Hofmann et al., 2010; Leahy et al., 2011). It has been associated with the ability to obstruct ruminative or depressive thought processes (Coffey & Hartman, 2008; Teasdale, 1999), and positively deal with negative affect (Arch & Craske, 2006; Coffey & Hartman, 2008; Lakey et al., 2008), cope with some risk factors like anxiety to decrease susceptibility to a host of psychological symptoms and problems (Vujanovic et al., 2007) and has been found to be negatively correlated with psychological distress and emotional disorders (Baer et al., 2006; Coffey & Hartman, 2008). Mindfulness has been reported to help in enhancing psychological flexibility. Psychological flexibility is the willingness to fully experience the present moment without defence (Hayes et al., 2011) and broadly covers psychological health and psychopathology (Hayes et al., 2011). It has been found that psychologically flexible individuals exercise less control over negative private events, that is, experiential avoidance, and may rather stick to their personal values (Hayes et al., 2006).
Experiential Avoidance
Experiential avoidance is defined as the refusal to experience sensations, feelings, and thoughts and engage in efforts to change these inner experiences. Experiential avoidance plays a central role in psychopathology (Hayes et al., 1996; Zvolensky et al., 2006). It has been found that experiential avoidance lasts only for some time, results in increased symptomatology, and is detrimental in the long run (Hayes et al., 1996). Regular use of experiential avoidance may lead to poor recovery from and heightened levels of negative affect, low levels of positive affect, decreased wellbeing, and poor social adjustment (Campbell-Sills et al., 2006; Gross & John, 2003,). Research has demonstrated that experiential avoidance is responsible for several clinical disorders and problems such as deliberate self-harm behaviour (Chapman et al., 2006), post-traumatic stress disorder (Kashdan et al., 2010; Marx & Sloan, 2005), panic disorder (White et al., 2006), generalized anxiety disorder (Roemer et al., 2008), and substance abuse (Forsyth et al., 2003).
Psychological Flexibility
Experiential acceptance is contrary, yet associated with psychological flexibility. Psychological flexibility means having an open standpoint towards the moment and includes negative thoughts or feelings (Bond et al., 2011). Acceptance is a psychological construct and implies the active non-judgmental acceptance of experience in the present moment, and letting things be without using escape behaviours (Bishop, 2002; Brown et al., 2007; Hayes, 2004;). It is considered a key component of mindfulness (Baer et al., 2006; Bishop et al., 2004; Brown & Ryan, 2003) and an extension of non-judgment. Acceptance is considered a central trans-diagnostic process that can explain a good proportion of the difference in various mood disorders (Kashdan et al., 2006). The psychological flexibility model also explains acceptance as a trans-diagnostic process that is vital in psychopathology (Hayes et al., 2006). Acceptance is central to mindfulness as well since the importance of practicing mindfulness lies through acceptance which allows one to have richer and more meaningful life experiences and it has been found that experiential acceptance helped predict general mental health, anxiety, and depression in different populations such as students and bank employees (Bond et al., 2011; Hayes, 2004; Sedlmeier et al., 2012).
Rationale of the Study
Since research has proved that acceptance is a trans-diagnostic process that has a significant role in psychopathology and in improving general mental health, we considered taking experiential avoidance, emotional disorders, and mindfulness in our study as there is a need to establish a relationship between all the constructs with respect to undergraduate and postgraduate students in India. To the best of our knowledge, this relationship between acceptance, mindfulness, and emotional distress has not been established in previous studies for this population. Hence, this study may be the first to consider these measures for students in India. Students face various kinds of challenges which are detrimental to their mental health and may adopt various coping strategies. To understand their mindfulness, psychological flexibility, and coping behaviours, we used measures such as self-reporting questionnaires that are widely used. It was assumed that students with high mindfulness would display a positive mood and low levels of depression. While students with low mindfulness would be prone to displaying more negative moods and experiencing depression, stress, and anxiety in the face of challenges. Research studies have reported that mindfulness-based interventions have a positive psychological effect on the emotional wellbeing, coping behaviour, and psychological flexibility of individuals. However, this has to be researched in the Indian context as we could not find studies based on such interventions.
The present work examined the relationship among dispositional mindfulness, measured using the Mindfulness Attention Awareness Scale (MAAS; Brown & Ryan, 2003), experiential avoidance, measured by Action Awareness Questionnaire (AAQ-II; Bond et al., 2011), and depression, measured by Depression, Anxiety and Stress Scales (DASS-21; Lovibond &d Lovibond, 1995). The study focuses on the association between experiential and meta-experiential processes associated with emotional suffering and psychopathology, like experiential avoidance, and processes, such as acceptance and mindfulness, which are associated with psychological flexibility.
Meta-experiential processes such as mindfulness and acceptance provide an unbiased, non-judgemental, and open experience to individuals. This, in turn, allows them to respond to situational challenges more flexibly and adaptively while simultaneously prohibiting maladaptive behaviours such as experiential avoidance. Building upon the preceding rationale and the existing literature, given the role of psychological flexibility, experiential avoidance, and mindfulness in coping with emotional distress like depression, we present the following hypothesis:
H1: Mindfulness is negatively associated with depression, stress, and anxiety.
Since mindfulness means being aware, in the present moment and non-judgemental, we hypothesized that mindfulness should correlate negatively with depression, anxiety, and stress.
H2: Mindfulness is associated negatively with experiential avoidance.
Since experiential avoidance promotes the occurrence of negative experiences which are detrimental to emotional processing and unknowingly reinforces emotional response and avoidant behaviour (Abramowitz et al., 2001; Campbell-Sills et al., 2006; Chapman et al., 2006; Purdon & Clark, 2001; Wegner & Zanakos, 1994; Wenzlaff & Wegner, 2000), we hypothesized that mindfulness is associated negatively with experiential avoidance, the latter being an avoidant coping behaviour contrary to mindfulness—which is an acceptance behaviour.
H3: Experiential avoidance is associated positively with depression, anxiety, and stress.
We hypothesized that experiential avoidance is positively associated with depression since it has been found through various studies that people tend to get solace from depressive thoughts, though momentarily, by practicing experiential avoidance. In their study, Hayes et al. (2006) found that experiential avoidance was associated with increased levels of depression, anxiety, psychological distress, and post-traumatic stress disorder symptoms in a community sample as well as in psychiatric populations.
H4: Experiential avoidance mediates the relationship between mindfulness and emotional distress.
We hypothesized that experiential avoidance is expected to reduce and may subsequently reduce depression in the presence of mindfulness, psychological flexibility, and acceptance. To cope with depression, people generally adopt avoidant strategies (Hayes et al., 2006; Kortte et al., 2009). Mindfulness, on the other hand, has been reported to have a positive effect on the psychological as well as physical health of a population (Baer, 2003), is reported to moderate the effect of neuroticism on depressive symptoms (Barnhofer et al., 2011), and is related to lower levels of stress, anxiety, depression (Barnhofer et al., 2011; Miller et al., 1995; Weinstein, et al., 2009). Hence, those with a high level of mindfulness do not adopt experiential avoidance as a coping strategy for stressful or demanding situations (Weinstein et al., 2009). Rather, they are found to be more accepting of their emotions, including positive and negative emotions or unwanted stressful thoughts. Since they display high experiential acceptance, they display more positive moods and low depression. Brown and Ryan (2003) reported an inverse relationship between dispositional mindfulness and anxiety. Mindfulness is being widely included in the treatment strategy for depression and anxiety in western nations. It has been reported in meta-analysis findings that mindfulness-based meditation practices or treatments like Mindfulness-based Stress Reduction improved depressive as well as anxiety disorder symptoms in individuals (Hofmann et al., 2010). Simultaneously, individuals who display high acceptance levels experience less anxiety and depression (Bond et al., 2011).
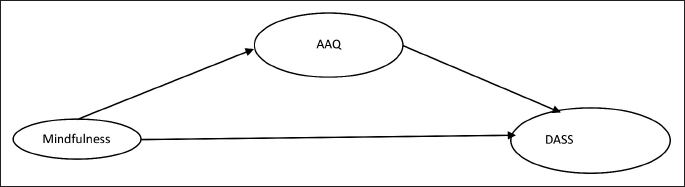
In sum, we propose the following conceptual model (Figure 1) for the study.
Conceptual Model of the Study.
MATERIALS AND METHODS
Sample and Data Collection
The questionnaire was circulated through Google Forms to randomly selected 1,000 undergraduate, postgraduate, and doctoral students studying in both state and private universities in Uttar Pradesh. We received 709 responses. However, 54 responses were not considered due to missing information; hence, a total of 655 responses were considered for analysis, thus giving it a response rate of 65.5%. We calculated the required number of participants in advance using GPower v3. The sample size was required to be 121 (effect size = 0.15, α = 0.01, power = 0.9, predictors = 2).
A total of 655 undergraduates (77.4%) and postgraduates (20.6%), above post-graduation (2%) students participated in the study, out of which 52.2% were males, and 47.8% were females, 89.6% were up to 25-years old and remaining were older than 25 years. 92% of the respondents had less than five years of work experience, and 5% had 5–10 years of work experience.
Measures
Mindful Attention Awareness Scale
The 15-items MAAS (Brown & Ryan, 2003) is a self-report questionnaire measuring dispositional mindfulness (e.g., ‘I rush through activities without being really attentive to them,’ ‘I drive places on “automatic pilot” and then wonder why I went there’). The items are distributed across cognitive, emotional, physical, interpersonal, and general domains (Brown & Ryan, 2003). The MAAS has a single-factor format and produces a single total score. It uses a six-point Likert scale (1 = almost always, 6 = almost never). Higher scores indicate greater mindfulness, high-order attention to the present moment, and a higher level of dispositional mindfulness. The scale demonstrates satisfactory internal consistency ranging from 0.82 to 0.86 (Baer et al., 2006; Brown & Ryan, 2003). The scale shows good convergent, discriminant, and incremental validity and strong psychometric properties. It has been validated with samples from college students, working professionals, community, general adults, and cancer patients (Baer et al., 2006; Brown & Ryan, 2003;). The MAAS taps consciousness which is positively correlated with psychological awareness, wellbeing, openness to experience, and emotional intelligence. It is inversely correlated with negative emotions like rumination and avoidance behaviours (Baer et al., 2006; Brown & Ryan, 2003).
The Acceptance and Action Questionnaire-II
The Acceptance and Action Questionnaire-II (AAQ-II) (Bond et al., 2011) was developed to improve upon the psychometric properties of its predecessor, the AAQ (Bond et al., 2011). It is a seven-item self-report questionnaire and is a widely used measure of experiential avoidance and psychological inflexibility. The AAQ-II, a uni-dimensional measure (Bond et al., 2011), examines the individual’s need for emotional and cognitive control, experiential avoidance, actions taken in the face of such events, and the evaluations made regarding these private experiences. It uses a 7-point Likert scale (1 = never true, 7 = always true) with a single total score. A higher score on the AAQ-II means a low level of acceptance and psychological inflexibility, which relates to greater emotional distress, poor general mental health, and higher levels of depression, anxiety, and stress, whereas lower scores mean greater experiential acceptance and behavioural flexibility. The AAQ-II possesses good internal consistency (Cronbach’s alpha: 0.76–0.82; Monestès et al., 2009), adequate reliability (mean ɑ coefficient = 0.84), and appropriate validity in six large and diverse samples across a wide range of regions (Bond et al., 2011) and has demonstrated strong correlation with measures of anxiety (r = 0.43) and depression (r = 0.65) (Berman et al., 2010).
The Depression Anxiety and Stress Scales
The DASS-21 (Lovibond & Lovibond, 1995), a modified version of DASS-42, consists of 21 self-report items divided equally into three scales of seven items each for depression, anxiety, and stress and is on a 0–3-point Likert scale (0 = Did not apply to me at all, 3 = Applied to me very much, or most of the time). The depression scale (DASS-D) assesses feelings of dysphoria, devaluation of life, and lack of interest or involvement. The anxiety scale (DASS-A) measures engagement in worrying, feelings of uncertainty, and physical symptoms indicative of autonomic arousal. The stress scale (DASS-S) assesses difficulty relaxing, feelings of agitation, irritability, and over-reactivity (Lovibond & Lovibond, 1995). Higher scores on each scale reflect higher levels of psychological distress. The DASS-21 has demonstrated good reliability and internal consistency for both clinical and non-clinical samples (Antony et al., 1998; Clara et al., 2001; Lovibond & Lovibond, 1995).
RESULTS
Table 1 reports the descriptive statistics, reliabilities, and bivariate correlations (using SPSS v24) of the constructs used in the study. Results exhibited that mindfulness is negatively related to the dependent variable DASS (r = −0.133, p = .001) and the proposed mediator of the study AAQ (r = −0.126, p = .001). AAQ and DASS were positively related to each other (r = 0.470, p < .001).
Descriptive Statistics, Reliability, and Correlation Matrix (n = 655).
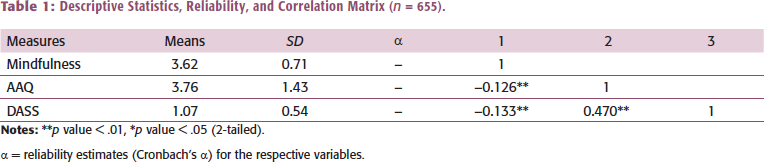
α = reliability estimates (Cronbach’s α) for the respective variables.
Further, to test the relationship between the constructs, we computed the regression coefficients. The objective was to examine the determinants of DASS among the measures employed in the study. First, the impact of mindfulness on DASS was tested. The linear regression model exhibited that mindfulness predicted DASS (β = −0.133, p = .001, 95% CI = (−0.160, −0.042)). Second, we tested the effect of AAQ on DASS. The regression model exhibited that AAQ was a significant predictor of DASS (β = 0.470, p < .001, 95% CI = (0.152, 0.205)). Finally, the effect of mindfulness on the proposed mediator AAQ was found significant (β = −0.126, p = .001, 95% CI = (−0.408, −0.098)). Thus, AAQ was considered as the potential mediator between mindfulness and DASS relationship for further analysis.
To examine the mediation analysis, we used the SPSS PROCESS macro (model 4) advanced by Preacher and Hayes (2008). Results (Figure 2) suggested that mindfulness is negatively associated with the outcome variable depression, stress and anxiety (DASS), thus supporting H1. Mindfulness was negatively associated with experiential avoidance (AAQ), thus supporting H2.
Final Path Model.
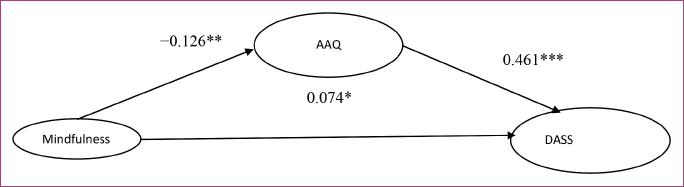
The experiential avoidance was positively associated with depression, stress and anxiety, thus supporting H3. The relationship between mindfulness and depression, stress and anxiety was partially mediated by experiential avoidance, supporting H4. The results exhibited that the direct effect of mindfulness on depression, stress and anxiety became weaker (β = −0.074, p = .03) when experiential avoidance as the mediator was added to the model, thus recommending a partial mediation by experiential avoidance.
Final Path Model (std. estimates) exhibiting DASS as a function of mindfulness and AAQ (*p < .05, **p < .01, ***p < .001). Overall model R2, which is a measure of variance explained in the endogenous variable, was 0.226, meaning that mindfulness and AAQ explained 22.6% variance in DASS.
Finally, to verify the mediation analysis results, we deployed bootstrapping method of bias-corrected confidence intervals (CIs) (Preacher & Hayes, 2008). Examination of the 95% bias-corrected CI from 5,000 bootstrap samples supported the mediation effect of AAQ between mindfulness and DASS (Table 2). If the confidence interval does not include zero, then the indirect effect of the mediator is significant, that is, the variable mediates the relationship between the predictor and the endogenous variable. In the current mediation model, we entered mindfulness as the predictor, and AAQ was entered as the mediator with DASS as the dependent variable. The direct effect of mindfulness on DASS was −0.074, and the indirect effect was −0.081. The total effect of mindfulness on DASS was −0.132.
Bootstrapping Analysis Summary.

DISCUSSION
Our study used a non-clinical sample to investigate the effect of mindfulness and experiential acceptance on psychological distress. We studied the relationship between mindfulness measured by the MAAS, experiential avoidance measured by AAQ-II, and psychological distress measured by the DASS. Results exhibited that mindfulness is negatively related to psychological distress and experiential avoidance. The study found that experiential avoidance and psychological distress were positively related. The effect of mindfulness on the proposed mediator, experiential avoidance, measured through AAQ-II was found to be significant. Hence, it was considered the potential mediator in the relationship between mindfulness and psychological distress. We found that the effect of mindfulness on psychological distress became weaker when AAQ-II mediated it. These findings conform to the previous studies which found that depression, stress, and anxiety show a significant decline through mindfulness and experiential acceptance (Silberstein et al., 2012). Based on the analysis, an emerging model will also be helpful for future studies.
Our study had four hypotheses: Mindfulness is negatively associated with depression, stress and anxiety (H1). Results suggested that mindfulness is negatively associated with the outcome variable depression, stress, and anxiety (DASS), thus supporting H1. Our second hypothesis was: Mindfulness is associated negatively with experiential avoidance (H2). The results show that mindfulness was negatively related to experiential avoidance (AAQ), hence supporting H2. Our third hypothesis was: Experiential avoidance is associated positively with depression, anxiety, and stress (H3). Results suggested a positive relation between experiential avoidance and depression, stress, and anxiety, thus supporting H3. Our fourth and final hypothesis was: Experiential avoidance mediates the relationship between mindfulness and emotional distress (H4). The results suggested partial mediation by experiential avoidance between mindfulness and depression, stress, and anxiety; hence, H4 was supported. The results showed that the direct effect of mindfulness on depression, stress, and anxiety became weaker (β = −0.074, p = .03) when experiential avoidance as the mediator was added to the model, thus suggesting a partial mediation by experiential avoidance.
Thus, the results show that experiential acceptance is a potential predictor for depression, anxiety, and stress when it is measured through AAQ-II. The results, as mentioned, are consistent with recent research which suggests experiential avoidance plays a key role in affective disorders (Kashdan et al., 2006) and is the primary source of psychological distress that leads to depression, anxiety, and stress. Its opposite is true in the context of experiential acceptance, which helps individuals to be less susceptible to psychological distress. Yet another dimension to such outcomes may be the socio-cultural background of the students and the phase of life they are in. As per the theory of Emerging Adulthood (Arnett, 2000), the age group of 18–25 is a period of life in which a person is neither an adolescent nor a young adult and can be best described as Emerging Adulthood (Arnett, 2000). Focussing their attention on the factors behind this dilemma, Arnett (2000) posited that the transformation in the socio-cultural background in industrialized societies had given rise to rapid changes and associated responsibilities. Compared to the previous generation, the age bracket for a settled job, marriage, and children has shifted, and with that, consequently, the mindset, due to which neither their parents nor they consider themselves young which leads to the concept of emerging adulthood. Ericson (1950, 1968), another author who contributed significantly to understanding the theory of human development across the course of life, mentions the age group specifically focussing upon young adulthood and adolescence. Thus, both Arnett (2000) and Ericson (1950, 1968) have discussed the impact of industrialized societies related to the age group this study chose, who are termed as neither adolescent nor young.
When looking at the Indian context, the situation remains almost the same, where emerging adults face issues like relationship challenges, career, and peer pressure. Such issues can adversely impact their thought processes which may result in depression, stress, and anxiety inter alia, and they adopt avoidance rather than acceptance as a coping strategy.
IMPLICATIONS FOR THEORY AND PUBLIC POLICY
The findings of the study can help both theory and policy formulation. The study establishes a relationship between mindfulness, emotional disorder, and psychological flexibility among students. This study’s findings may help formulate policy with special reference to students, where mindfulness practices are incorporated into the curriculum to enable them to deal with emotional disorders with acceptance, thereby bringing down their depression, anxiety, and stress levels.
The present study establishes the relationship between the direct and indirect effects of mindfulness and depression, anxiety, and stress (DASS), which has multifaceted implications for individuals and communities. Individuals may engage themselves in a process of self-improvement through mindfulness mediations using online or app-based mindfulness interventions (Bailey et al., 2018; Chittaro & Vianello, 2016), which has the potential to impact their affective responses towards day-to-day circumstances and happenings positively.
The study outcomes present vital implications for public policy. As the importance of positive mental health and the absence of depression, anxiety, and stress is increasingly being recognized by communities, several national governments have initiated an exploration of processes that integrate people’s wellbeing as a nation’s strategic objectives through budgetary methods (Durand & Exton, 2019). The severity of the issue can be understood through the fact that one out of five children and adolescents in India have reported adverse mental health issues during their school years (NIMH, 2015). Children and adolescents who face such issues have shown difficulties in academic functioning (e.g., lower performance, greater behavioural issues in school) and higher dropout rates with respect to the children and adolescents who do not experience such problems (Koller & Bertel, 2006; McLeod et al., 2012). Several experimental and longitudinal studies have demonstrated that mindfulness could be cultivated by various mindfulness interventions (Brown & Ryan, 2003) at different stages of life. Thus, policymakers may design school-based mindfulness interventions which are innovative and cost-effective (Meiklejohn et al., 2012), targeted at children who are going to be future decision-makers.
LIMITATIONS AND FUTURE RESEARCH
The present study was subjected to some limitations. First, though the study provided preliminary evidence of the findings, it was conducted among a non-clinical sample. Future research may examine if the findings of this study can be generalized with a clinical sample of students suffering from depression, stress, and anxiety. Second, the study findings should be interpreted with the usual precautions associated with self-reported cross-sectional data. Future researchers may conduct longitudinal studies involving mindfulness-based interventions. We have presented the preliminary evidence, and we expect future researchers to join this stream of literature and validate the study findings through different study techniques and methods of data collection.
Footnotes
DECLARATION OF CONFLICTING INTERESTS
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author received no financial support for the research, authorship, and/or publication of this article.
e-mails:
e-mail: