
Abstract
Scholars in health economics have been studying the relationship between healthcare expenditure and health outcomes for the last half-century. Researchers emphasized the increase of public health expenditure towards providing primary healthcare based on the logic that health expenditure has a direct effect on the health outcomes of the people. However, such studies have a lot of inconsistencies. Given the background, the present study has three research objectives. First, to investigate the effect of healthcare spending on multiple health outcomes in SAARC nations after controlling for country-specific health infrastructures and economic conditions. Second, to undertake a differential analysis of the effect of public and private healthcare spending (both aggregate and out of pocket) on specific health outcomes. Third, to explore the presence (if any) of the differential effect of health expenditure and health infrastructure variables on specific health outcome variables, including mortality and morbidity indicators. Based on a 20-year (1993–2012) panel data from seven SAARC countries, health expenditure was found to influence improved health outcomes in SAARC nations. In addition, the differential effect of public, private and out-of-pocket (OOP) health expenditure was observed on different health outcomes. Thus, OOP expenditures was found to be the major influencer of life expectancy, death rate and TB instances, while public expenditure was found to be influential for improving infant mortality rate (IMR). The present study supports the notion that disaggregated effects of health expenditure (by including the effect of public, private and OOP expenditures) are needed to get a complete understanding of the health expenditure–health outcome linkage. In addition, the findings emphasize on the role of proximal predictors of health outcomes (alongside expenditure variables in the same model) as important inclusion in the health expenditure-health outcome investigation.
Researchers have found investment in human capital to be a significant stimulus fostering economic growth and even development in most developing countries (Kim & Lane, 2013; Romer, 1994). The quality of health was found to significantly affect human capital development with the logic based on the endogenous growth model (Romer, 1994) or Grossman’s human capital model (Somi et al., 2009). The same effect was mediated by utility derived from better health conditions and additional human capital (Romer, 1994). In this context, Novignon et al. (2012) found research support for the effect of health status on the current and the future welfare of households.
Scholars in health economics have been studying the relationship between healthcare expenditure and health outcomes for the last half-century (Bokhari et al., 2007; Bradley et al., 2010; Kim & Lane, 2013; Poullier et al., 2002). A major finding that emerged was the role of the composition of public spending (i.e., public/out-of-pocket [OOP] or revenue/capital) in enhancing health outcomes (Bhalotra, 2007; Gani, 2009). Researchers emphasized the increase of public health expenditure towards providing primary healthcare. The rationale behind the same was that such expenditure ameliorated the effect of ailments on the productive lifespan of the individuals (Verhoeven et al., 1999).
While some empirical studies find a significant positive effect of healthcare spending on health outcomes (e.g. Anyanwu & Erhijakpor, 2009; Bradley et al., 2010; Novignon et al., 2012), others note the absence of any significant relationship between the two (such as Burnside & Dollar, 1998; Kumar et al., 2013). Similar inconsistencies could be attributed to multiple factors. First, complex policy structures hampering the utilization of such funds may moderate the disbursement of funds in public spending. Thereby, the effect (and effectiveness) of public health expenditure may not be fully realized on subsequent health outcomes (Grigoli & Kapsoli, 2013; Wagstaff & Claeson, 2004). Thus, monetary expenditure is not directly comparable across different systems that disperse the same money differently and in different patterns. Second, the exclusion of private health expenditure and its effect on health outcomes may result in partial explanation of the impact of health expenditure (Berger & Messer, 2002; Issa & Ouattara, 2005). Third, many variables such as health infrastructure and social factors may influence health outcomes (Bokhari et al., 2007). Notable among these are per capita income (Issa and Ouattara, 2005), access to clean water and proper sanitation facilities (Volpe et al., 2009), availability of trained doctors (Akinkugbe & Mohanoe, 2009) and number of hospital beds relative to the population. Researchers need to incorporate more explanatory variables (beyond health expenditure) to derive conclusive arguments.
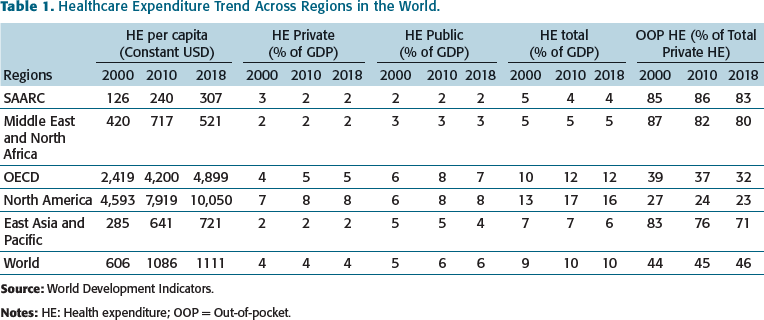
Healthcare Expenditure Trend Across Regions in the World.
The major challenges for public health institutions common in most SAARC countries include high population burden, illiteracy, income disparity and a significant rural–urban divide (Simon et al., 2015). This unequal distribution of health and economic resources affects the poorer sections of society negatively. Additional issues include the unavailability of generic drugs at low prices (Munsur et al., 2009), unsatisfactory levels of immunization facilities and drugs (Poullier et al., 2002), and poor public health infrastructure (Farahani et al., 2010). Most SAARC countries suffer from a shortage of trained health personnel in public health facilities, especially in rural areas. At the policy level, health systems in the SAARC region face hurdles, such as a lack of evidence-based policy framework and low social accountability (Ray et al., 2002).
Researchers have explored the interplay between private and public expenditure on health and found a relation between the share of private and public expenditure and the development of the country. While the rich countries were found to have a higher share of public expenditure, the lower-income countries were found to have a higher proportion of private and OOP health expenditure (Gerdtham & Jonsson, 2000). A lower share of public spending on health may designate a more active private sector in the health space. In very few cases, in countries such as the United States and Switzerland, when the health expenditure and public involvement in health is high, public expenditure majorly replaces private expenditure on health (Poullier et al., 2002; Potrafke, 2010). However, most Organisation for Economic Co-operation and Development (OECD) countries have a mixture of financing sources regarding health expenditures. Even though expenditure on health has been found to positively affect health outcomes, it is poorly correlated with GDP per capita (Linden & Ray, 2017). While the joint effects of public and private health expenditure on health outcomes has been researched, focus on measuring the interrelationship between these two and modelling their effects on health outcomes in the presence of other related variables such as health infrastructure and population demographics has been rarely explored.
Given the background, there is a need for a study that investigates the relationship between multiple health influencing variables and its outcome on multiple health indicators. The present study has three research objectives. First, to investigate the effect of healthcare spending on multiple health outcomes in SAARC nations after controlling for country-specific health infrastructures and economic conditions. Second, to undertake a differential analysis of the effect of public and private healthcare spending (both aggregate and OOP) on specific health outcomes. Third, to explore the presence (if any) of the differential effect of health expenditure and health infrastructure variables on specific health outcome variables, including mortality and morbidity indicators. Based on the research objectives, the following hypotheses (null) were tested in the present study:
There are no significant differences in the effects of public versus private expenditure on health (including the effect of OOP health expenditures) on health outcomes in SAARC countries;
There are no significant effects of health infrastructure variables on health outcomes in SAARC countries;
There are no significant differences on the effect of health expenditure variables across specific health outcomes.
The first hypothesis builds on findings from Novignon et al. (2012) and extends their argument with the addition of OOP expenditures. The second and third objectives are based on the suggestions of Akinkugbe and Mohanoe (2009) and Volpe et al. (2009).
Based on a 20-year (1993–2012) panel data from seven SAARC countries, health expenditure was found to influence improved health outcomes in SAARC nations. In addition, the differential effect of public, private and OOP health expenditure was observed on different health outcomes. To be precise, OOP expenditures was found to be the major influencer of life expectancy, death rate and instances of tuberculosis (TB), while public expenditure was found to be influential for improving infant mortality rate (IMR). The present study supports the notion that disaggregated effects of health expenditure (by including the effect of public, private and OOP expenditures) are needed to get a complete understanding of the health expenditure–health outcome linkage. In addition, the findings emphasize on the role of proximal predictors of health outcomes (alongside expenditure variables in the same model) as important inclusion in the health expenditure-health outcome investigation.
STUDY VARIABLES
Four health status indicators were used in the present study as dependent variables (DVs). These are IMR, crude death rate (CDR), life expectancy at birth (LEB) and incidence of TB.
Researchers have suggested the inclusion of multiple health indicators to increase the robustness of the results (Novignon et al., 2012; Rad et al., 2013). Cutler et al. (2006) opine that the relation between social status and health is complex and may not be amenable to a single explanation using one or two outcome variables. For example, health outcome indicators such as mortality rates and life expectancy may reflect the health status of a population only in part. Thereby, it may not allow the identification of feedback mechanisms and causal linkages between health expenditures and health outcomes (Kindig, 1997). Likewise, in developing nations, a rise in income and health expenditure may lead to a longer life span but may also induce habits such as smoking (since disposable income is high), leading to higher instances of TB (Pampel, 2007).
In addition, Larson and Mercer (2004) note that health indicators in developing nations suffer from limitations related to reporting and data collection. Thus, an aggregate of health indicators is more likely to provide the right picture of a nation’s health status. For example, infant mortality and life expectancy provide information on mortality and longevity but are not sufficient to provide information about disease instance, fertility and morbidity (Larson & Mercer, 2004; Rad et al., 2013). Thus, four health indicators were selected as DVs. The four indicators measured mortality and morbidity measures of a population independently. Researchers have frequently used IMR as a mortality indicator, and its relationship with health expenditure is well documented (Bradley et al., 2011; Goldman & Grossman, 1988). Similarly, LEB is considered an inclusive measure of health status as it may include the effects of mortality, morbidity and disability (World Health Organization [WHO], 2010,) and it is found to increase with an increase in public health expenditure (Kim & Lane, 2013). The CDR was included as a morbidity measure as researchers have suggested a negative impact of public health expenditure and infrastructure on death rates (Mays & Smith, 2011). The instance of TB was the fifth and final health outcome in the study as it is a serious health indicator that needs to be controlled (Lönnroth et al., 2010) and researchers found public expenditure to affect the increase/decrease of TB prevalence in a country (Tanimura et al., 2014).
The predictor variables included in the study are as follows: (a) income (measured as GDP per capita); (b) public expenditure on health as a percentage of GDP; (c) private expenditure on health as a percentage of GDP; (d) OOP private expenditure as a percentage of GDP; (e) number of hospital beds available per 1,000 individuals; (f) number of physicians per 1,000 individuals; (g) percentage of the population that has access to improved sanitation facilities; (h) percentage of the population that has access to clean water sources; (i) adult literacy rate, and (j) rate of participation of females in the labour force.
Measures for income and expenditure (both public and private) were added as they are expected to influence health outcomes (Novignon et al., 2012). Majority of studies have estimated public and private health expenditures as a share of GDP (such as Grigoli & Kapsoli, 2013; Kaushal et al., 2013; Novignon et al., 2012; Peters et al., 2003) and thus, the present study followed the same measures. The OOP expenditures were included in the model as they are critical determinants of healthcare status in developing countries that have improper health infrastructure (Shahrawat & Rao, 2011). We defined OOP health expenditure as ‘any direct outlay by households, including gratuities and in-kind payments, to health practitioners and suppliers of pharmaceuticals, therapeutic appliances, and other goods and services whose primary intent is to contribute to the restoration or enhancement of the health status of individuals or population groups’ based on the WHO definition. We also defined private health expenditures as those coming from ‘domestic private sources including funds from households, corporations and non-profit organizations’. Clean water sources and sanitation facilities are important health infrastructure factors that influence health status (Grigoli & Kapsoli, 2013), even though their effects on specific health outcomes did not receive much attention. Thereby, they were included. Lastly, the availability of hospital beds and physicians were included as measures of health infrastructure. While sanitation and water sources could be considered indirect (or distal) health infrastructure factors influencing health outcomes, hospital beds and availability of physicians could be considered direct (or proximal) factors (Bhandari & Dutta, 2007; Kindig, 1997).
Lastly, to add robustness to the model, two socio-economic predictors of health outcomes were included in the present study, namely, adult literacy and female labour force participation. Education is considered an influential social determinant of health outcomes (Kabir, 2008). Educated women may have higher productivity at home, resulting in better family health and higher rates of child survival. Educated women have a higher life expectancy and lower child mortality (Grabauskas & Kalediene, 2002; Kalediene & Petrauskiene, 2000). Educated people would be more aware of healthcare, and thus their instances of disease and morbidity may be lower (Cutler & Lleras-Muney, 2006). In addition, the participation of individuals (majorly women) in the labour force of the nation may have a direct influence on individual health status (Cai, 2010). On the contrary, bad working conditions, higher work pressure and job stress may lead to health deterioration (Cai, 2010). It is important to include the two variables with the other predictor variables to make the model more complete.
THE EMPIRICAL MODEL AND METHODS
The generic panel equation model specified for the present study is illustrated in Equations 1 and 2.

In Equation 1, y it represents the vector of the DVs in country i at time t. The constant is denoted by α and X represents the vector of the exogenous variables. The vector of the regression coefficients is denoted by β and ε it is the vector of random error. The time trend is represented by τ. The random effects term is given by u i (where u i and ε it are independent). The article follows a simple model of panel data estimation as suggested by Hsiao (2014) and Elhorst (2003).
In the present study, the specific form of the equation derived from the generic form (Equation 1) is given in Equation 2.
In Equation 2, HO represents the four health outcomes, namely, IMR, LEB, CDR and TB. GDPC represents the per-capita GDP at constant prices. HEXPB and HEXPT represent the share of public and private health expenditure as a percentage of GDP, respectively. OPHEXP represents OOP health expenditure (calculated as a percentage of total health expenditure). HOSBD and PHYS represent the number of hospital beds and physicians available per 1,000 people, respectively. SANI and WTRSC represent the percentage of the population with access to improved sanitation facilities and water sources, respectively. LIT represents the adult literacy rate, and LBP represents the female (ages 15–64) labour force participation.
The present study used pooled cross-section data and yearly time series data from 1993–2012 for the seven SAARC countries: Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan and Sri Lanka. Afghanistan was the only SAARC country excluded from the analysis because of a lack of continuous data. The empirical data was collected from the World Bank statistics on the World Development Indicators (WDI) (Simon et al., 2015). All variables were converted to natural log to avoid skewness within data (log-log model).
Elhorst (2003) suggest a random effects model in panel data to avoid the loss of degrees of freedom that may be incurred in a fixed effects model associated with a relatively large sample size. Thus, in the present study, a random effects model (country) was estimated using generalized least squares (GLS). However, the Hausman specification test was conducted first to ensure that the data was more appropriate for a random effects model (like the procedure of Novignon). The Hausman test results favoured the random effect models for the country; thus, the same is reported in the results.
RESULTS
Descriptive Statistics
Descriptive Statistics.
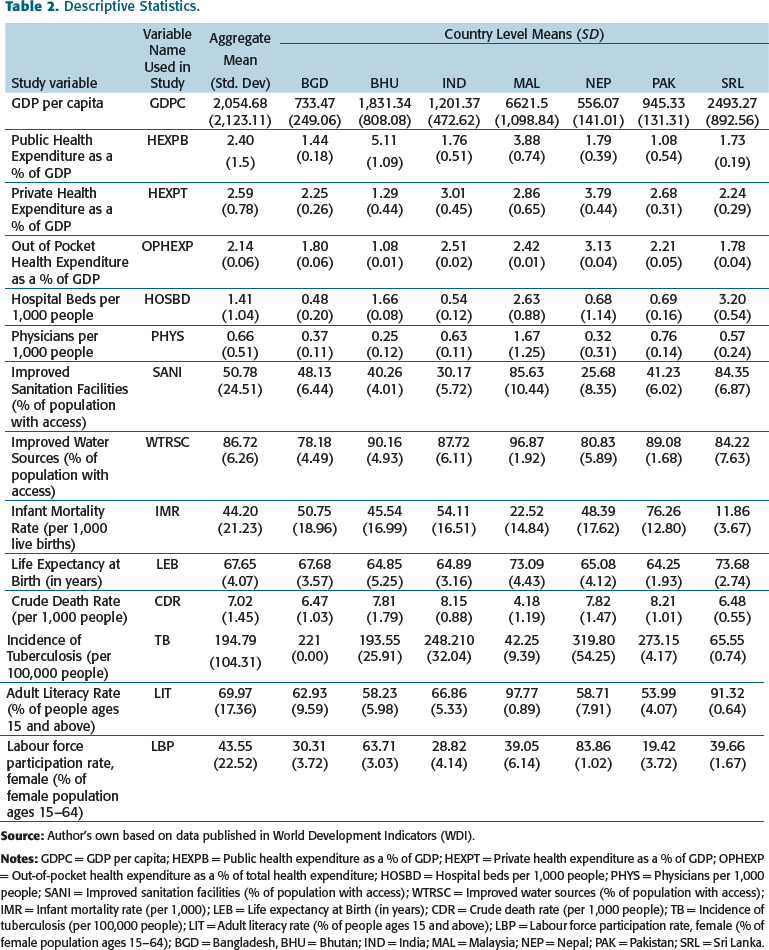
The mean hospital beds per 1,000 people and physicians per 1,000 people were found to be around 1.41% and 0.66%. The mean LEB in the SAARC region was about 67 years. Infant mortality (per 1,000 live births) was around 44, while the CDR (per 1,000 people) was 7. The mean incidence of tuberculosis was estimated at 195 per 100,000 people. Approximately 86% and 51% of the population had access to improved water sources and sanitation facilities, respectively. GDP per capita and instances of TB were found to vary across countries to a significant extent (Table 2).
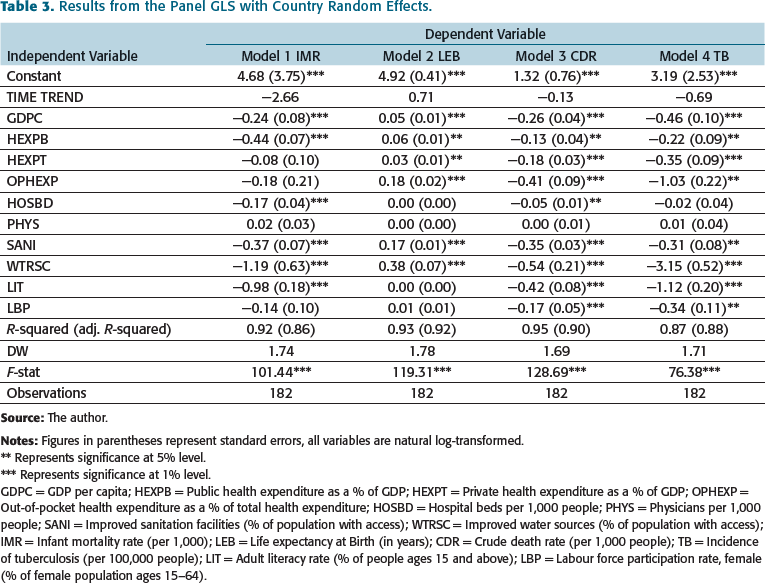
Results from the Panel GLS with Country Random Effects.
** Represents significance at 5% level.
*** Represents significance at 1% level.
GDPC = GDP per capita; HEXPB = Public health expenditure as a % of GDP; HEXPT = Private health expenditure as a % of GDP; OPHEXP = Out-of-pocket health expenditure as a % of total health expenditure; HOSBD = Hospital beds per 1,000 people; PHYS = Physicians per 1,000 people; SANI = Improved sanitation facilities (% of population with access); WTRSC = Improved water sources (% of population with access); IMR = Infant mortality rate (per 1,000); LEB = Life expectancy at Birth (in years); CDR = Crude death rate (per 1,000 people); TB = Incidence of tuberculosis (per 100,000 people); LIT = Adult literacy rate (% of people ages 15 and above); LBP = Labour force participation rate, female (% of female population ages 15–64).
Infant Mortality
The per capita income (GDPC), per capita public expenditure on health as a percentage of GDP (HEXPB), hospital beds per 1,000, access to sanitation facilities and improved water source, and literacy rate were all found to have a significant effect on the IMR (Table 3). A 1% increase in per capita GDP was estimated to bring down infant mortality by 0.26%. An increase in per capita public expenditure on health by 1% was estimated to decrease IMR by 0.41%. Similarly, one unit increase in hospital beds was found to reduce IMR by 0.16%. An increase in access to improved sanitation facilities (SANI) was observed to decrease IMR by 0.21%, and an increase in access to improved water source was observed to decrease IMR by 1.17%. An increase in adult literacy rate by 1% was observed to reduce IMR by 0.98%. None of the other variables had any significant effect on IMR.
Life Expectancy
Access to an improved water source (WTRSC, 1% increase) was found to have the most significant effect (increase LEB by 0.37%) on LEB followed by access to improved sanitation facilities (SANI, an increase LEB by 0.18%). A 1% increase in OOP health expenditure (OPHEXP) was found to increase LEB by 0.17%. Public and private health expenditures were found to have a positive and significant effect, respectively, on LEB (unlike the case of IMR). Per-capita GDP was found to have a positive and significant effect on LEB, though its effect size was small. Adult literacy rate and female labour participation was not found to have any significant effect on LEB.
Death Rate
Both public and private health expenditure were found to have a significant effect on reducing the death rate (CDR) (Table 3). However, the effect size was more for private expenditure (0.19) than public expenditure (0.17). OOP health expenditure (OPHEXP) was found to be more important in reducing CDR than public or private expenditure, as a 1% increase in the same was observed to reduce CDR by 0.42%. Similar to the results related to TFR, improved water source (WTRSC) had the largest impact on CDR as a 1% increase in access to improved water source decreased CDR by 0.53%. Access to improved sanitation facilities (SANI) was a significant influencer of CDR, as was income or (GDP per capita) (Table 3). Both literacy rate (LIT) and female labour participation (LBP) were observed to have a significant and negative influence on the death rate. The number of hospital beds per 1,000 had a significant negative effect on the death rate, though the effect size was small (0.04).
Health Expenditure and Instances of Tuberculosis
All variables except hospital beds and physicians were found to have a significant effect on the instances of TB. Access to improved sources of water and sanitation facilities were found to significantly affect TB. (For example, a 1% increase in access to improved water sources would decrease TB by 3.13% and a 1% increase in access to improved sanitation facilities would decrease the TB instances by 0.28%.) The OOP expenditure was found to have a significant effect on TB since a 1% increase in OOP expenditure reduced TB instances by 1.01%. Similar results were found for literacy rate (1.02% decrease). A 1% increase in public and private health expenditure was found to reduce instances of TB by 0.2% and 0.32%, respectively. Income was found to reduce the instances of TB (1% rise in GDPC would decrease TB instances by 0.47%). Lastly, female labour participation was found to decrease TB instances (1% rise in LBP would decrease TB instances by 0.33%).
DISCUSSION
The findings from the study indicate a significant role of health expenditure in the betterment of health outcomes in SAARC nations. It supports existing research (Bokhari et al., 2007; Bradley et al., 2011; Kim & Lane, 2013; Poullier et al., 2002). However, the most important contribution of the present study lies in the results that show differential effect public, private and OOP health expenditure on different health outcomes. While OOP expenditure was the biggest influencer of life expectancy, death rate and instances of TB, public expenditure was influential for IMR. In addition, the study also brings forth an empirical investigation into the correlation between private and public health expenditure that is not well explored in extant research.
The findings support the disaggregation of total healthcare expenditure into public and private components, as suggested by Novignon et al. (2012). The present study augments the argument by including OOP health expenditures that are considered critical determinants of multiple health outcomes in low-income nations (Balarajan et al., 2011; Shahrawat & Rao, 2011). However, this finding opens a new point for discussion. Researchers consider OOP health expenditures to be detrimental to economic growth and they may lead to instances of poverty in low-income nations (Balarajan et al., 2011). The finding of the significant and high effect of OOP expenses on reducing TB further supports this point. If the burden of more fatal diseases has to be borne by the individuals, it may subsequently lead to catastrophic effects on the disposable income (Brinda et al., 2014). While OOP expenditures may lead to improved health outcomes, its adverse effects may result in a lowering of disposable income and may subsequently lead to worsened health outcomes such as under-nutrition (Chandrasiri et al., 2012). This is a dilemma since public health facilities are either insufficient or inefficient (Farahani et al., 2010; Majumder, 2013; Munsur et al., 2009; Shakya, 2004, p. 73). It puts forth a policy issue for the government to ensure the delivery and availability of quality healthcare for all sections of the society.
The second contribution of the present investigation is the aggregation of health infrastructure variables in the same model (such as the number of hospital beds per 1,000 and access to sanitation facilities). Researchers such as Bokhari et al. (2007) have called for the inclusion of health infrastructure variables in addition to health expenditure measures to assess the impact on health outcomes in a comprehensive manner. The present study addresses the call. The results indicate a significant influence of access to improved sanitation facilities on all health outcomes in the research and access to a better water source on all study variables except infant mortality. The significant effect of sanitation and improved water source on health outcomes in the presence of expenditure components imply that they are important determinants of health outcomes and that should be considered alongside the components of expenditure. The effect size and the sign of the effect deserve special focus. Improved sanitation facilities reduced infant mortality and death rate as expected. Sanitation was also found to increase life expectancy. While TB is not waterborne, sanitation was found to reduce the instances of TB too. This implies that access to improved water sources could act as a proxy for various health outcomes. This is further supported by the findings as access to clean water was found to affect all dependent variables (such as increased life expectancy and reduced death rate). This finding supports the existing literature. This also brings a policy implication that the government should focus on the provisioning of clean water.
To summarize, the distal measures of health infrastructure were found to influence most of the health outcomes in a significant manner, with some unexpected aberrations. The findings underline the importance of choosing the right model structure that is tested empirically. The non-inclusion of health infrastructure variables may lead to partial or inconclusive results. There may be a possibility that this omission of important variables was behind the studies that did not find any significant effect of health expenditure on health outcomes (e.g., Glied & Lleras-Muney, 2003).
Among the proximal measures of health infrastructure, that us, number of hospital beds and physicians per 1,000, the results varied. Whereas the number of hospital beds (per 1,000) was found to affect IMR, TFR and CDR, the number of physicians per 1,000 people was not found to have any significant effect on any dependent variable. This partially contradicts the literature that suggests the opposite (Akinkugbe & Mohanoe, 2009). However, careful observations of the descriptive statistics related to the SAARC countries suggest low levels of both the variables across the countries along with small deviations (Table 2). Thus, the lack of provisions may be the reason behind the findings of the insignificant effects.
The inclusion of socio-economic variables in the study (literacy rate and female labour participation) makes the study more comprehensive. The literacy rate reduced IMR, TFR, CDR and instances of TB. This indicates that a population that is more educated would be aware of health-related information, which would reflect in their actions, leading to favourable health outcomes. Labour force participation was found to reduce death rates. This may be because of two reasons. First, employed women may be economically better off because of the higher disposable income. This would allow them to live a healthier life than unemployed people. Second, the level of stress and boredom may be less for employed women, leading to lesser family stress and thereby higher longevity. Labour force participation was found to reduce instances of TB. This may be because of the increased economic power that would enable people to live healthier lives and afford better healthcare. It may also be because of the increased level of information that employed women may derive from being in an environment where they can interact with their peers.
To summarize, the major contributions of the article could be outlined as an empirical explanation of the relationship between public and private health expenditures, elucidating the differential effects of different types of health expenditure on different health outcomes, incorporating the impact of health infrastructure in the same model alongside health expenditure and, finally, incorporating the effects of socio-demographic variables jointly with the variables, as mentioned earlier on the health outcomes. The inclusivity of the gamut of variables in this research adds to its robustness and generalizability.
POLICY IMPLICATIONS
At the aggregate level, the present study supports the importance of public health expenditure in improving health outcomes in the SAARC region. However, it also notes the significant role of private healthcare spending on major health outcomes. First, the ‘OOP influence’ indicates the possible inefficiencies in public healthcare and the lack of proper distribution of health services by the government to the general population ,which the private sector is filling in. Second, the significant effects of OOP health expenditure (especially for outcomes such as death rate) imply that people in the SAARC region rely on OOP health expenditures for health-related issues. Per capita income was found to significantly affect all outcome variables (with appropriate directionality). This points out that an increase in income would positively influence the health outcomes in the SAARC countries. Poverty is a serious issue in the SAARC region (Balarajan et al., 2011), and thus at a policy level, measures to reduce poverty would indirectly affect health outcomes through increased income.
The policy implications of the present study emphasize the role of the government in increasing both health expenditures and health infrastructure to create better health outcomes. The OOP expenditure affecting health outcome raise an alarm for the policymakers as poverty is a major problem in SAARC countries, and OOP may be a cause for poverty in lower-income groups. The government should investigate the causes behind such high OOP expenditures and should undertake appropriate measures to curb health expenditure-influenced poverty. Lastly, the findings related to the health infrastructure (i.e. number of physicians and number of hospital beds) suggest that the SAARC regions suffer from scarcity of both these elements. Thus, the government should aim to increase this ratio directly or with public–private partnerships. The research puts forward some incremental and novel contributions for the academics and implications for policymakers to ponder.
Footnotes
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship and/or publication of this article.