
Abstract
The article is an investigative study drawn on the grounded theory approach, envisaging the relation between workplace bullying and employee behavioural outcomes among resident doctors in Indian healthcare organizations. Using an interpretative paradigm, the authors explored underlying psychological mechanisms among 48 participant doctors in light of India’s unique culture characterized by power distance and high collectivism. Findings suggest that the prevalence of bullying in Indian healthcare organizations impacts employee behavioural outcomes emerging as a major challenge in healthcare management. The authors further exhibit restricted or non-violation of resident doctors’ psychological contracts towards such diabolic acts at work due to the development of passive feelings in light of learned helplessness. The current study establishes that Indian resident doctors are less pretentious, and the protestations against supervisory mistreatment are subdued even before joining the medical profession. Indian kids being fostered with relationship-focused values, namely tolerance, patience and respect towards their elders/seniors from a very tender age develop feelings of passivity, which might result in limited or no violation of their psychological contract. Drawing on conservation of resources (COR) theory, forgiveness emerged as a coping mechanism in pernicious work culture, providing uniqueness to study. This qualitative research study promulgates the unique response mechanism of workplace bullying in the Indian context. The study results open new gateways to empirically analyse the relationship between bullying-response mechanisms in developing economies. Theoretical and managerial implications are discussed in the present research study.
Keywords
Workplace bullying and its adverse effects on the organization and its members have garnered a lot of academic interest in the past three decades (Tuckey & Neall, 2014). Workplace bullying is a salient occupational stressor characterized by negative interpersonal acts targeted toward employees at their workplace (e.g., unrealistic deadlines, excessive workload, spreading rumours or insulting remarks, etc.). While it has been widely studied in the developed economies, research on workplace bullying in India is still in its nascent stage (D’Cruz et al., 2016). Although prevalent in varied occupational settings, bullying in the healthcare sector is no exception (Di Martino, 2002). The Indian healthcare sector, being one of the largest in terms of both employment and growth (IBEF, 2021), witnessed numerous incidents of workplace bullying and harassment, especially among resident doctors. Looking at ‘India’s unique culture (Hofstede, 1980), “victims” response to workplace stressors is a promising avenue’ (Chun et al., 2006). This investigative study is an attempt to reconnoitre this austere occupational stressor among resident doctors in Indian healthcare organizations and explore its relation with employee behavioural outcomes.
In a dynamic healthcare setting, employee voluntary behaviours, that is, organizational citizenship behaviours (OCB; Organ, 1988) and constructive deviant behaviours (CDBs; Robbins & Galperin, 2010) play a pivotal role while ensuring the overall well-being of healthcare organizations. Although a considerable amount of literature exhibits a linear relationship between bullying and employee outcomes (Lanctôt & Guay, 2014), there is limited research highlighting underlying mechanisms in the said relation, that is, plausible mediators and moderators. Behind every behavioural outcome, certain psychological mechanisms are involved (Rigotti, 2009). Thus, this study tries to envisage the underlying psychological mechanisms in the relation between workplace bullying and employee behavioural outcome in the Indian healthcare sector. The authors adopted the grounded theory approach (Charmaz Z., 1995; Strauss & Corbin, 1994, 1997) to examine real bullying experiences of Indian healthcare employees and their interpretation in light of India’s unique culture chiefly characterized by power distance and high collectivism (Hofstede & Hofstede, 2005).
Literature Review
Workplace bullying, a form of interpersonal transgression, hinders normal work routine (Zapf et al., 1996) while having detrimental effects on employees, organization and society (Einarsen et al., 2011; Malik & Farooqi, 2011; Tuckey & Neall, 2014). It involves ‘the act of harassing, offending, and socially excluding someone at the workplace (Einarsen et al., 2011) while affecting the victim’s work tasks and behaviours’ (Devonish, 2013; Nielsen & Einarsen, 2012; Salin, 2014). Workplace bullying has two chief characteristics: persistency and power disparity (Einarsen et al., 2003). These negative acts can be work-related, person-related or physically intimidating (Einarsen et al., 2009).
Bullying at work is a universal phenomenon, and the likelihood of encountering workplace bullying among medical care employees is about three times compared to any other occupational setting (Brophy et al., 2018). Healthcare employees with their commitment towards patients’ well-being are considered more vulnerable (Field, 2002) and thus, bullies are more ubiquitous in healthcare settings (Brophy et al., 2018; Piquero et al., 2013). Moreover, negative acts are recurrently targeted toward trainees or junior doctors (Brophy et al., 2018; Paice et al., 2004; Quine, 2002) as they are considered abecedarian by their supervisors and seniors (Fox & Stallworth, 2005).
Workplace bullying likely affects employees’ psychological contracts (PC) with their respective organizations (Salin & Notelaers, 2020). PC is an implicit contract wherein employees psychologically examine existential work circumstances and compare them to their expectations (Robinson & Rousseau, 1994). When employee’s expectations are not parallel to the real world, PC is said to be violated, resulting in anger and a feeling of betrayal (Morrison & Robinson, 1997). Extant literature suggests that psychological contract violation (PCV) is a mediator between workplace bullying and employee behavioural outcomes (Emre et al., 2011; Kakarika et al., 2017; Salin & Notelaers, 2020).
Looking at ‘India’s unique culture characterized by power distance and collectivism’ (Hofstede, 1980), resident doctors find it arduous to raise their voice against such deleterious acts or their bully at work (Einarsen & Skogstad, 1996), looking at subsequential ramifications it can have on their medical careers (Tepper et al., 2001). In such conditions, the victim tends to withhold actions or behaviours that benefit the organization and its adherents (Parzefall & Salin, 2010; Zellars et al., 2002). Based on social exchange theory (Blau, 1968), employees tend to reciprocate favourable/unfavourable behaviour they receive at work (Robinson, 2008).
In the healthcare sector, prosocial employee behaviours such as OCBs (Organ, 1988) and CDBs (Galperin, 2003) largely contribute to the well-being of both the organization and its members. OCBs have been defined extensively as a vital ‘S’ ‘US’ factor (Oades & Dulagil, 2017) that serves to facilitate organizational effectiveness and functioning (McNeely & Meglino, 1994). When employees find it onerous to even raise their voice against their bully or are unable to seek revenge or reciprocate similarly, they often engage themselves in behaviours that impede overall organizational well-being (Dollard et al., 1939; Zellars et al., 2002). Literature suggests that bullying at work largely impacts employee’s OCBs (Gupta & Bakhshi, 2018; Zellars et al., 2002).
Furthermore, in a dynamic healthcare setting, employees’ CDBs are sporadically vital for patient safety, dispensing quality services and preventing organizations from bearing financial liabilities (Robbins & Galperin, 2010). It is apparent from healthcare literature that aberration from the standards is sometimes indispensable for the effective functioning of a healthcare organization (Robbins & Galperin, 2010). This study manifests that to facilitate the well-being of healthcare organizations, CDBs can act as change agents while adapting new and innovative medical procedures (Erwin, 2009).
There are limited studies highlighting the importance of constructive deviance, particularly in the healthcare sector (Robbins & Galperin, 2010). As per authors’ knowledge, this qualitative study is one rare attempt to explore the relationship between workplace bullying and CDBs in the Indian healthcare sector and also attempts to highlight various underlying psychological mechanisms (Rigotti, 2009) in said relationship.
This study aims to ascertain the existence of workplace bullying among resident doctors in Indian healthcare organizations and assay its relationship with employee behavioural outcomes. This qualitative study is undertaken to identify possible mediators and moderators in the relationship between workplace bullying and employee outcomes. The authors aim to develop a conceptual framework linking various themes emerging from the instant study.
Research Methodology
Research Design
To explore the relationship between workplace bullying and employee behavioural outcomes in the Indian healthcare sector, the current study adopted the grounded theory approach (Charmaz, 1995; Strauss & Corbin, 1997). Contrary to quantitative research, instant study envisioned capturing the lived experiences of the respondents (Charmaz Z., 1995; Rennie, 2014; Strauss & Corbin, 1998) and registering ‘participants’ interpretations of experiences as per their personal philosophy (Birks & Mills, 2015). This method is found to be appropriate to investigate the ‘participants’ subjective experiences of bullying at work and derive meaning out of it by comparing one interview excerpt with another and relating them with an explanatory concept to develop a theory (Charmaz K., 2010; Glaser, 1992).
It is natural that how a human understands the dynamics of his world and interprets things around him is influenced mainly by his antiquity and milieu (Mills et al., 2014). To develop the indigenous knowledge, grounded theory research is a promising avenue to ascertain culture-specific aspects of a phenomenon from native’s point of view (Malinowski, 1922; Tsui et al., 2007). Workplace bullying is a culture-varying phenomenon (Power et al., 2013). Adopting the grounded theory approach seems apt to either discover a completely new phenomenon or to extend or revise prevailing phenomena in a novel cultural context, that is, India (Rai & Agarwal, 2017)
Sample Characteristics and Sampling Procedure
This qualitative study is limited to Indian healthcare organizations based in the Delhi area. Adopting a judgmental sampling technique, the authors shortlisted India’s top government healthcare organizations based on the National Institutional Ranking Framework (NIRF, 2019) in the medical category. As per grounded theory research, the sampling procedure is purely theoretical and involves researcher’s judgement in finding the correct sample so they can contribute well to emerging theory. Thus, only clinical departments were considered for the instant study. Furthermore, both academic junior resident doctors (JRs) and senior resident doctors (SRs), with more than six months of work experience (Exp. >6 months) at their current organization, were considered, as suggested by Einarsen et al. (2009). The concept of saturation (Glaser & Strauss, 1967) was employed to determine the instant study sample size.
Data Collection
In-depth conversational interviews were conducted with 48 resident doctors (Annexure 1) out of the 51 initially approached via judgemental sampling technique as theoretical saturation was reached and no new knowledge was further provided (Strauss & Corbin, 1998). Before commencing interviews, each participant was briefed about the study. The briefing was done to ensure participants have sufficient knowledge about the concept under study and thus facilitate data reliability and validity (Saunders et al., 2009). A convenient place and time were discussed with participants for conducting interviews. Each interview was conducted in English and lasted for 40–45 minutes. All ethical research protocols were followed, including taking due permission of participants to record their responses and their consent to participate in the instant study. Responses were later transcribed verbatim by listening and re-listening to the audios (recordings) by authors to learn implicit meanings (Charmaz Z., 1995).
Interview Guide
For conducting the qualitative pilot study, the authors prepared a semi-structured interview guide with questions relating to participants’ personal bullying experiences and of their colleagues, about their mental status of being a sufferer or a bystander of bullying at work, their behavioural outcomes and coping mechanisms in such working conditions and also about source(s) of bullying (Annexure 1). The interview guide was supported by a thorough review of available literature in pursuit of conducting germane interviews and also facilitating participants to give narratives of their experiences at the workplace.
Data Analysis
In grounded theory studies, the coding of collected data (Charmaz Z., 1995; Jørgensen, 2001) is followed by a process of categorization which finally results in the emergence of themes. The current study adopted a systematic coding procedure (Charmaz, 1995; Strauss & Corbin, 1997). This was followed by simultaneous data analysis undertaken by the authors manually and independently to ensure meaningful qualitative data. Codes were identified by thoroughly studying each transcript line-by-line to identify key phrases and better understand the underlying concepts (Strauss & Corbin, 1997). Line-by-line coding (Charmaz Z., 1995; Jørgensen, 2001) was done to ensure higher-order data categorization. Initial line-by-line coding was followed by focused coding (Charmaz, 1995). More data was analysed until no new data emerged, and those codes were identified that appear to repeat most frequently (Strauss & Corbin, 1998). The codes were labelled in vivo (Flick, 2006), and a comparative method was adopted wherein similar incidents and events were labelled and grouped to form categories (Strauss & Corbin, 1990). By doing so, the authors could facilitate the development of the concept understudy more accurately. Throughout, memo-writing was in progress to enable authors to specify conditions in which codes exist and relation among them, emerging ideas, new interpretations and questions (Charmaz Z., 1995; Jørgensen, 2001).
After identifying substantive categories, axial coding followed, wherein authors were involved in data reconstruction to identify relations between emergent categories (Strauss & Corbin, 1998). Developed relations and categories were repeatedly verified against texts and data using inductive and deductive approaches (Strauss & Corbin, 1990). The process of data coding and categorization was supported by extant literature on workplace bullying (Miles & Huberman, 1994). Some categories were in line with existing literature, such as the pervasiveness of workplace bullying (among healthcare employees) and bullying being a cultural phenomenon. Some categories, such as constructive effects of workplace bullying and forgiveness being a coping mechanism, emerged entirely from our data providing uniqueness to the instant study. Mainly four themes emerged, namely existence of workplace bullying, non-violation of the psychological contract, workplace bullying influences employee behavioural outcomes and forgiveness might act as a coping mechanism. Double quotes are used to present the findings of the current study (Charmaz Z., 1995). Re-readings of literature were simultaneously done to analyse emerging assumptions, relationships and processes (Charmaz Z., 1995; Strauss & Corbin, 1990).
Member Checking
For validation of research findings, member-checking (Lincoln & Guba, 1985) was used for the instant study. To enhance data analysis credibility (Goldblatt et al., 2011), data interpretations were presented to all participants for judging and assisting in establishing a link between emergent categories and themes (Goldblatt et al., 2011). Results aligned with ‘participants’ experiences of bullying and its relation to their behavioural outcomes and coping mechanisms. Through member-checking activity, none of the participants’ and authors’ interpretations was found to be conflicting (Varpio et al., 2016)
FINDINGS AND DISCUSSION
With this exploratory study, four main themes emerged after a systematic analysis (as explained above) of interview data. Interview excerpts are highlighted in double quotes to support the study findings. Furthermore, the anonymity of each participant was maintained as a pre-condition to participate in the study. Therefore, only their unique participant code (Annexure 1) is mentioned in the excerpts.
Theme 1: Existence of Workplace Bullying Among Indian Resident Doctors
In this exploratory study, the prevalence of workplace bullying is quite evident among Indian healthcare employees. During conversational interviews, all 48 participating resident doctors reported at least one bullying incident either faced by them or by their contemporaries at work persistently:
‘It’s a ritual, every other day I see (one of) my friend repenting getting admission in his department (Orthopaedics) as he routinely gets intimidated either by his supervisors or by patients … he is quite distraught about his future in this profession.’ (p. 6)
Bullying can be work-related, person-related or physical in nature (Einarsen et al., 2003). In the present study, at least 17 out of 48 respondents reported being a victim of person-related bullying once in their medical career. Whereas six respondents reported being bystanders of physical abuse on their contemporaries at work. Witnessing incidents of work-related bullying at almost regular intervals was found to be common among all the respondents. Excerpts of their varied types of bullying experiences are reproduced below:
‘I am an SC (Scheduled Caste) candidate, and I overheard some of my batchmates questioning my talent in getting admission here (in the medical school) and told me I am lucky that I belong to a special category … I was quite disheartened listening to this’. (p. 2)
‘I still remember one of our colleagues was slapped by a professor in front of other junior doctors, staff members, and patients … (he) use to verbally threaten to fail us in exam’. (p. 41)
Many participants blamed the Government for ‘India’s overburdened hospitals and inadequate medical facilities. A crisis exemplified by the fact that India would need around 2.07 million more doctors to achieve the suggested doctor-patient ratio of 1:1000’ (WHO, 2019). In comparison, the current ratio is 1:3629 (IBEF, 2021)
‘Healthcare organizations are not much at fault as they are only following government directions. In my opinion, Government is (at fault) … isn’t government aware of how much work we do and attend thousands of patients in a day without any break?‘(p. 35)
Moreover, resident doctors are in their training period and thus, constantly supervised by senior doctors and consultants. In India, where there is a culture of power distance and high collectivism (Hofstede, 1980), such doctors find it onerous to raise their voice against seniors/supervisors due to the exiguous power they hold (Einarsen et al., 2003) and to avoid setbacks in the career:
‘We are here to learn, and our superiors and senior doctors help us fine-tune our respective subjects and this is what I am here for … their pedagogy might be harsh; I just ‘can’t raise my voice against them and invite problems for myself protesting against them’. (p. 16)
It can be affirmed from the responses that bullying does exist in the Indian healthcare sector, especially among resident doctors, almost on a regular basis. Reasons vary from them being considered as vulnerable to cultural barriers.
Theme 2: Non-violation of Psychological Contract of Indian Resident Doctors
As per extant literature, violation of a PC results when an employee experiences frustration, fury and disappointment emanating from non-fulfilment of employee’s predicted organizational promises and obligations towards him/her (Morrison & Robinson, 1997). PCV has a domino effect on the depletion of ‘employees’ vital resources, that is, time, energy, respect and dignity. Findings of the current study establish that Indian resident doctors are less pretentious, and protestations against supervisory mistreatment are subdued even before joining the medical profession. Based on learned helplessness theory (Maier & Seligman, 1976), authors predict that bullying at work is considered to be uncontrollable and independent of response-outcome relation among Indian resident doctors:
‘I was aware that I get to work long hours, without food and sleep … despite of knowing all this, I entered into the medical profession. I ‘can’t change the system’. (p. 4) It’s always the case that the more powerful one suppresses the one with less power, but I am aware of what my chosen career is and what I am here for … I don’t think much. (p. 29)
Furthermore, Indian kids are fostered with relationship-focused values, namely tolerance, patience and respect towards their elders/seniors, from a very tender age (Triandis, 1994). Parents make their kids believe in the institution of treating their mentors as God who bestow them with knowledge and ask them to be tolerant towards their admonishment (Sinha, 1990; Sinha & Sinha, 1990) as it is believed to be worthy for their overall development:
‘All these years, I have been asked by my parents to just focus on my work and let go all negative things happening around me at professional or academic front. In India, gurus (teachers) are treated as idols, whatever they do, they only want good for us’. (p. 45)
Authors predict that Indian resident doctors, after repeatedly experiencing such malevolent acts at workplace, develop feelings of passivity which might subsequently result in limited or no violation of their psychological contract(s). This study provides a new tangent to look at bullying-outcome relationship in light of learned helplessness theory (Maier & Seligman, 1976) and novel Indian culture (Hofstede, 1980)
Theme 3: Impact of Bullying at Work on Employees’ Workplace Behavioural Outcomes
Through this qualitative pilot study, authors found bullying at work affects behavioural outcomes of Indian resident doctors:
Organizational Citizenship Behaviours
OCBs, also known as prosocial voluntary behaviours, are indispensable for the proper functioning of an organization (Organ, 1988). In the presence of precarious work situations such as bullying, victim withholds voluntary actions or behaviours that benefit the organization and its adherents (Zellars et al., 2002). In this study, the authors found resident doctors to be less allied to their current healthcare organization:
‘Seldom offer ideas or any suggestions for improvement of hospital functioning. I have never been asked and don’t even remember giving any. I just complete work at hand and call it off for the day’. (p. 25)
Authors further predict that incidents of workplace bullying might affect employees’ organizational defending capacities in terms of preserving the public image or exhibiting concern while others disparage it:
‘I hardly recommend this institute for medical studies due to ill-treatment I faced here of lately … long working hours and unreasonable work deadlines add to the trauma’. (p. 10)
Constructive Deviant Behaviour
Medical practitioners, engaged in CDBs are believed to bring innovative procedures and a new era of medicine characterized by increased patient safety and quality of medical aid (Robbins & Galperin, 2010). While questioning an organization’s status quo to safeguard its well-being, both CDB and voice behaviour seem relatable but are disparate as the latter chiefly focuses on making only verbal constructive suggestions while the former essentially violates dysfunctional organizational norms (Galperin, 2003). Authors predict that challenging work conditions may oppress resident doctors to opt for more functional medical procedures, thus, imperilling organization’s well-being:
‘I lately solved a patient’s problem by breaking a mundane hospital procedure (but) faced with warning from my supervisor … (I) now spare myself of unnecessary questioning and criticisms’. (p. 23)
Through this study, authors further predict that bullying experiences at work might endanger smooth hospital functioning and patient safety by subduing such voluntary CDBs among resident doctors, who otherwise could bring a new era of medical procedures (Robbins & Galperin, 2010)
Theme 4: Existence of a Resilient Measure-forgiveness among Resident Doctors
There is an interesting finding of this exploratory study, wherein forgiveness emerged as a resilient/coping measure in case of bullying at work and was found to influence employee behavioural outcomes among Indian resident doctors. Drawing on the COR theory (Hobfoll, 1989), we predict that forgiveness might act as a moderator in the relationship between workplace bullying and organizational well-being. COR theory is based on the precept that individuals, in a challenging situation, tend to protect or conserve their current valued resources (time, energy, self-esteem) to attain professional development (Halbesleben et al., 2014):
‘Since we have to study, we don’t keep these (negative workplace acts) in our mind. It will distract and kill our remaining time which can be used in productive ways’. (p. 18) ‘I have wasted my youth, time and energy to be where I am today, if I keep it in my head and heart, I will never be able to be at peace and focus on more productive things’. (p. 32)
Primacy of resource loss, a basic tenet of COR theory, has a motivational element which predicts employees engaging in avoidance/let-go behaviour to evade further resource loss while maintaining their well-being (Halbesleben et al., 2014):
‘Yes, I have been mistreated, but I need not think much about it … unless someone makes it personal. It’s like a next day and I need to blow off the steam in order to treat my patients well’. (p. 3) ‘I actually forgave the offender but have to endure her every time we met … trying to focus on more meaningful things else I will burn in agony … (I) forgive but couldn’t forget’. (p. 5)
During interviews, some participants claimed to forgive their offenders upon comprehending that they have high pressure to perform in their chosen career. They were also of the opinion that bullying had constructive effects on their professional skills:
‘I now realised that whatever my seniors did with me had actually helped me improve my skills and also made me more confident … sometimes such behaviour works best for you to improve your art’. (p. 34)
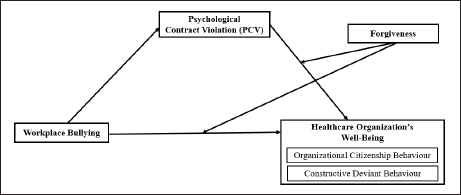
The findings and simultaneous review of the extant literature facilitate the authors in developing the conceptual framework (Figure 1).
Conclusion and Implications
Theoretical Implications
This study is an attempt to explore the relationship between workplace bullying and resident doctors’ behavioural outcomes crucial for the well-being and functioning of Indian healthcare organizations. With this study, the authors tried to envisage mechanisms of underlying moderators and mediators in said relationship. Firstly, this study affirms the prevalence of austere occupational stressors, that is, workplace bullying, among resident doctors in the Indian healthcare sector. Secondly, authors predict restricted or non-violation of resident doctors’ psychological contracts towards such diabolic acts at work due to development of passive feelings in light of learned helplessness theory (Maier & Seligman, 1976) thus, providing a new tangent to investigate bullying-outcome relation. Thirdly, the presence of bullying at work was found to impact resident doctors’ behavioural outcomes, that is, OCBs and CDBs, which are crucial for the well-being of healthcare organizations and patient care (Robbins & Galperin, 2010). Lastly, this study contributes to extant literature by finding a coping strategy among victims of workplace bullying, that is, forgiveness. Authors believe forgiveness can act as a moderator and facilitate the smooth functioning of Indian healthcare organizations.
Managerial Implications
Workplace bullying impacts employee behavioural outcomes, that is, prosocial voluntary behaviours believed to support the work environment where main tasks are being performed. Thus healthcare organizations must employ a zero-tolerance policy against workplace bullying (Meloni & Austin, 2011) and introduce awareness programmes like Stop it (Benmore et al., 2018) to improve working relationships. Furthermore, an independent body must be created in every Indian healthcare organization where bully-victims, can register their complaints without any obstruction. Additionally, HR professionals with experience in healthcare must be employed to timely resolve interpersonal conflicts (Srinivasan & Chandwani, 2014). With this study, the authors suggest that forgiveness might act as a resilient measure. In a dynamic work environment, such as healthcare organizations, where offences are inevitable, social motivation training may improve interpersonal relationships (Struthers et al., 2005). All these measures, if implemented effectively, can help in building bully-free workplace settings (Woodrow & Guest, 2014) in Indian healthcare organizations benefitting Indian medical practitioners and the public at large.
LIMITATIONS AND FUTURE RESEARCH DIRECTIONS
Although this study undertakes the interpretative approach in explaining the underlying relation between bullying at work and employee behavioural outcomes, it has some limitations. Firstly, this study has a gender-blind perspective on employee behavioural outcomes when confronting bullying at work. Future studies can consider gender perspective in the bullying-outcome relationship since reactions and interpretations towards workplace bullying might vary among men and women (Escartín et al., 2011). Although authors ensured respondents of concealing their identities throughout the study, they cannot rule out the possibility of social desirability bias on the part of the participants (Podsakoff et al., 2003). Future researchers can opt for longitudinal analysis to avoid such biases. For greater generalisability of study results, a similar study must be replicated in varied cultural contexts and geographical areas other than Delhi to investigate whether like results are obtained among resident doctors.
Sample Matrix.
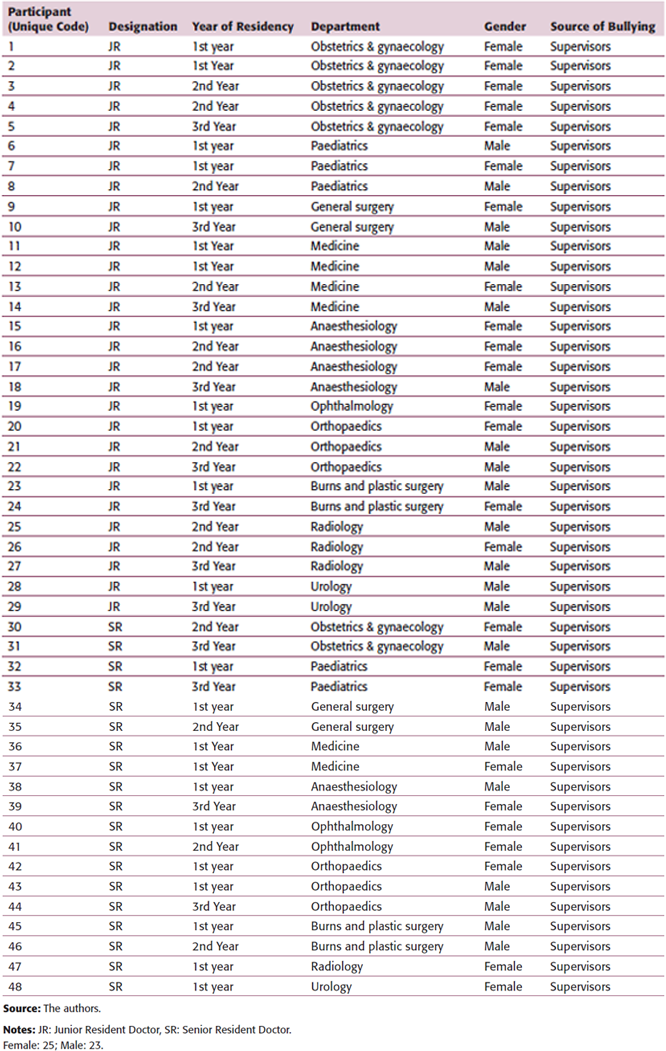
Female: 25; Male: 23.
Footnotes
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship and/or publication of this article.
e-mail: