
Abstract
Executive Summary
Catastrophic health expenses result in impoverishment of a large number of people every year in India. This often forces the resource-poor households to forego treatment due to lack of affordability. Providing quality health care to all at an affordable cost is a policy commitment for India as it is a signatory of the Alma Ata Declaration. The Government of India is working towards providing universal health coverage through its National Health Policy. As part of universalization of health care, the government had launched a publicly financed health insurance scheme, Rashtriya Swasthya Bima Yojana (RSBY), to provide affordable and quality health services. The present study dealt with understanding the impact of the scheme for improving health care-seeking and reducing burden of health expenditure among resource-poor families through a matched controlled cross-sectional study. The study tried to assess whether RSBY had improved care-seeking and reduced incidences of catastrophic health expenditure (CHE) and health expenditure-induced poverty among the insured population and also tried to explore whether the benefits were equitable. It was conducted in purposively selected two blocks of Ranchi district in Jharkhand with 1,643 households below poverty line (BPL). Both enrolled and non-enrolled households were selected randomly for the study after matching with some key matching criteria. It was found that RSBY neither increased in-facility treatment (hospitalization) nor reduced the likelihood of CHE among the enrolled households. More importantly, it significantly increased the incidence of health expenditure-induced poverty among the households who were above the poverty line before incurring any health expenditure. From equity perspective, care-seeking was much lower among the economically weaker households compared to the better-off households. Similarly, incidences of CHE and health expenditure-induced poverty were also found to be higher among the weaker sections. The study shows that RSBY did not achieve its objective of improving care-seeking and providing financial security to the enrolled households, and more importantly to the economically weaker sections of the society. Other studies have also found that one of the factors for high out-of-pocket expenditure in health is a weak public health delivery system which forces people to seek care from private providers. Hence, it is important for the policymakers to critically evaluate whether such insurance models will actually ensure better financial security for the households from excessive health expenditure and whether strengthening the existing public health delivery system would be a better option.
Keywords
In this backdrop, the Indian government launched Rashtriya Swasthya Bima Yojana (RSBY), a publicly financed health insurance scheme in 2007 to provide financial security and improve access to hospitalization services to BPL families. The insurance covers up to five members in a household. It covers almost all hospitalization cases, day care services that do not require hospitalization, and provides maternity coverage up to a limit of ` 30,000 per annum. Key features of this scheme include covering pre-existing diseases, providing cashless benefit, portability of RSBY Smart Card, etc. However, RSBY does not cover out-patient services which is one of the major limitations of the scheme.
Some studies have shown that RSBY has done well in enrolling the intended families in the states such as Himachal Pradesh, Delhi, and Gujarat. Studies have also shown that awareness level of the community about RSBY has increased and now larger populations are availing the benefits of RSBY in these states (Dilip, 2012; Gupta, 2010; Krishnaswamy & Ruchismita, 2011). However, other studies found that its communication strategy, a key for success of the scheme, was ineffective (Das & Leino, 2011; Trivedi & Saxena, 2013). The enrolment in RSBY was far below expectation, largely due to poorly organized enrolment drives by the insurance companies and discrimination faced by the households during enrolment drives (Nandi et al., 2012; Qifei, 2012). Under RSBY, around 70 per cent of the empanelled hospitals were private. The services were found to be expensive when compared to public providers (Nandi et al., 2012; Selvaraj & Karan, 2009). Hospitalization rates were still very low in RSBY programme and regional disparities were also found in the hospitalization rates (Devadasan, 2011). Factors for low utilization of health care under RSBY were found to be refusal of providing treatment, continuous decrease in the premium paid, shortage of quality medical facilities in the catchment areas, delays in issuance of smart cards, and errors in information in the smart cards, etc. (Qifei, 2012).
RESEARCH GAP AND RESEARCH OBJECTIVE
These evidences provide an overview of the successes and areas of concern of the scheme. However, most of the studies used secondary data like National Sample Survey Office (NSSO) data which could not separate out or identify households that were covered under insurance and also the effect of insurance on improved care-seeking or reduced incidence of catastrophic health expenses (Devadasan, 2011; Selvaraj & Karan, 2012). Some studies used primary data, however, they only focused on specific aspects such as impact of Information, Education and Communication (IEC), reduction of OOP health expenditure on enrolment under RSBY or institutional capacity and their incentives under the scheme (Das & Leino, 2011; Devadasan, Seshadri, Trivedi, & Criel, 2013; Gupta, 2010; Rajasekhar et al., 2011; Trivedi & Saxena, 2013). Some other studies are descriptive in nature (Forgia & Nagpal, 2012; Qifei, 2012; Trivedi & Saxena, 2013). These studies did not capture the effect of the RSBY towards increasing care-seeking or reducing CHE or health expenditure-induced poverty. Hence, a cross-sectional-controlled study was designed to see whether RSBY could achieve its intended objectives of increasing the health-seeking behaviour and reducing the burden of CHE, both from equity and efficiency perspectives. This research also aimed to assess the demand side and other social determinants of care-seeking and CHE.
STUDY DESIGN AND SAMPLING
Population Characteristics of Bundu and Silli Blocks
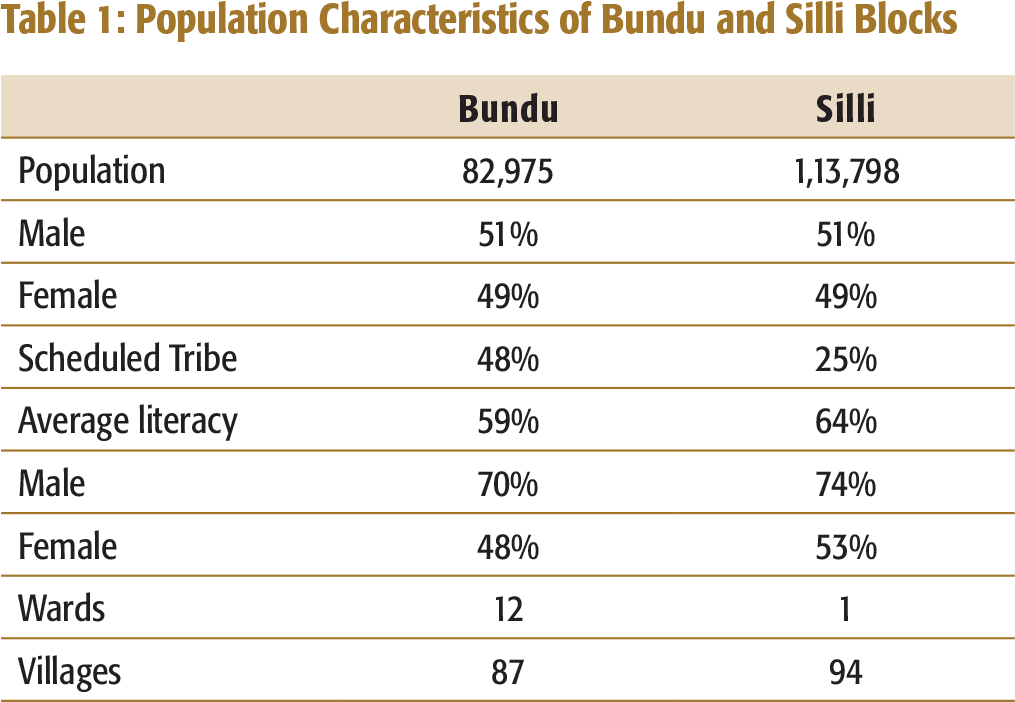
For representative sampling, villages and wards were randomly selected from the two blocks. In Bundu, 30 units (22 villages and 8 urban wards) and in Silli, 30 units (29 villages and 1 urban ward) were selected. In Bundu, units were divided into villages and wards based on rural–urban population ratio, using 2011 Census. However, in the case of Silli, there was only 1 ward, and it was selected along with 29 villages.
A qualification round was conducted by visiting all the BPL households in the selected villages. Information on BPL households with enrolment status and other related data were collected for matching and randomly selecting the households. Additional information such as cases of hospitalization, childbirths in the last one year, and records of out-patient services received in the last one month by any member of the household were also collected.
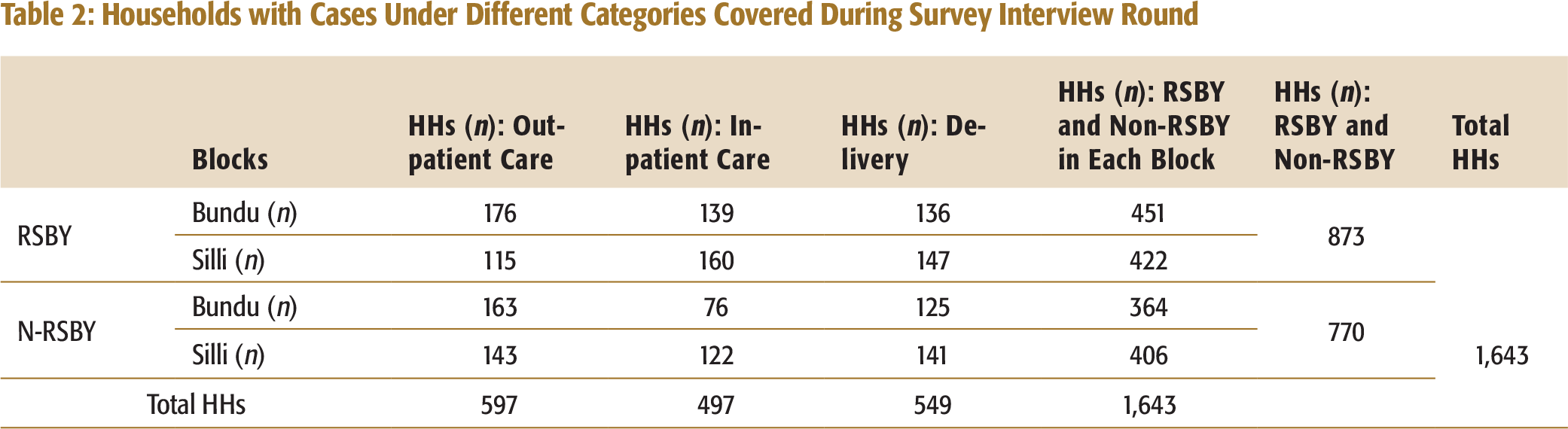
For the survey interview round, using prevalence of CHE among the poor and non-insured households of 35 per cent, and with an assumption of reduction of CHE by 10 per cent to 25 per cent in the insured households, a sample size of 425 households was estimated with 80 per cent power to detect the change in CHE between insured and non-insured households with 95 per cent confidence level and 10 per cent attrition in each arm for each block (Shekhar, 2011; Smith & Day, 1984). So, for both the blocks, total sample size of 1,650 households was estimated with 825 households in each arm. The assumption of reduction in CHE by 25 per cent was taken based on different studies conducted in different Asian countries (Shekhar, 2011; Wagstaff & Doorslaer, 2003).
Sample size was calculated using simple random sampling technique following the given formula (Binkin, Sullivan, Staehling, & Nieburg, 1992; Lemeshow & Stroh, 1988; Smith & Day, 1984; Sullivan, 1995):
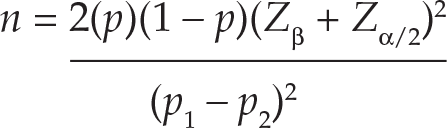
n = Sample size in each group (assumes equal-sized groups)
Zβ = Represents the desired power (typically 0.84 for 80% power).
Zα/2 = Represents the desired level of statistical significance (typically 1.96 for 95% confidence level).
p = Estimate of the expected current proportion of CHE, that is, 35 per cent.
p1 − p2: Effect size (the difference between the expected current proportion of CHE and expected reduced proportion due to RSBY intervention).
Households with Cases Under Different Categories Covered During Survey Interview Round
Interviewers for data collection were hired locally from the same blocks. They belonged to local ethnic communities and were proficient in speaking the local language/dialect. All the interviewers had prior experience of conducting surveys and data collection work on health issues. All of them were given a two-day in-house training as well as two days of practical sessions in the field on the questionnaire content, techniques to elicit more information, and strategies for obtaining complete and reliable data. A mechanism was developed for continuous review and feedback to them during the data collection work.
INCLUSION AND EXCLUSION CRITERIA FOR STUDY HOUSEHOLDS
For the qualification round, all families with BPL registrations from the selected blocks were included. For the survey interview round, all BPL families—where at least one member was hospitalized in the last 12 months or families with cases of childbirth in the last 12 months or families where any member was treated in out-patient care in the last 30 days—were included for sampling. The sampling included households where a member had expired within the reference period, but the family had incurred medical and non-medical expenditures. Those household members who stayed for less than six months in the house were excluded from the study, in accordance to NSSO health and morbidity survey. However, children born at any time during the reference period were included in accordance with the definition of morbidity and health survey 2014 of NSSO working under Ministry of Statistics and Programme Implementation (MoSPI), Government of India.
RESEARCH INSTRUMENT
Survey questionnaire was used to collect socio-economic and demographic information from the sampled RSBY and non-RSBY households during the survey interview round. Information on households’ health events, health behaviour, awareness about RSBY, their self-reported illness episodes, expenditures (both direct and indirect medical expenditures) incurred on treatment, health care providers visited, sources of finance for bearing treatment costs, claim received from RSBY, etc., were collected. Data on household’s consumption expenditure was collected using mixed recall period, that is, a 12-month recall period for six infrequently purchased non-food items, namely clothing and footwear, durable goods, education, medical expenses and any other non-food expenditure such as travel/entertainment, etc., and a 30-day recall period for frequent expenses including food.
DATA ANALYSES AND RESULTS
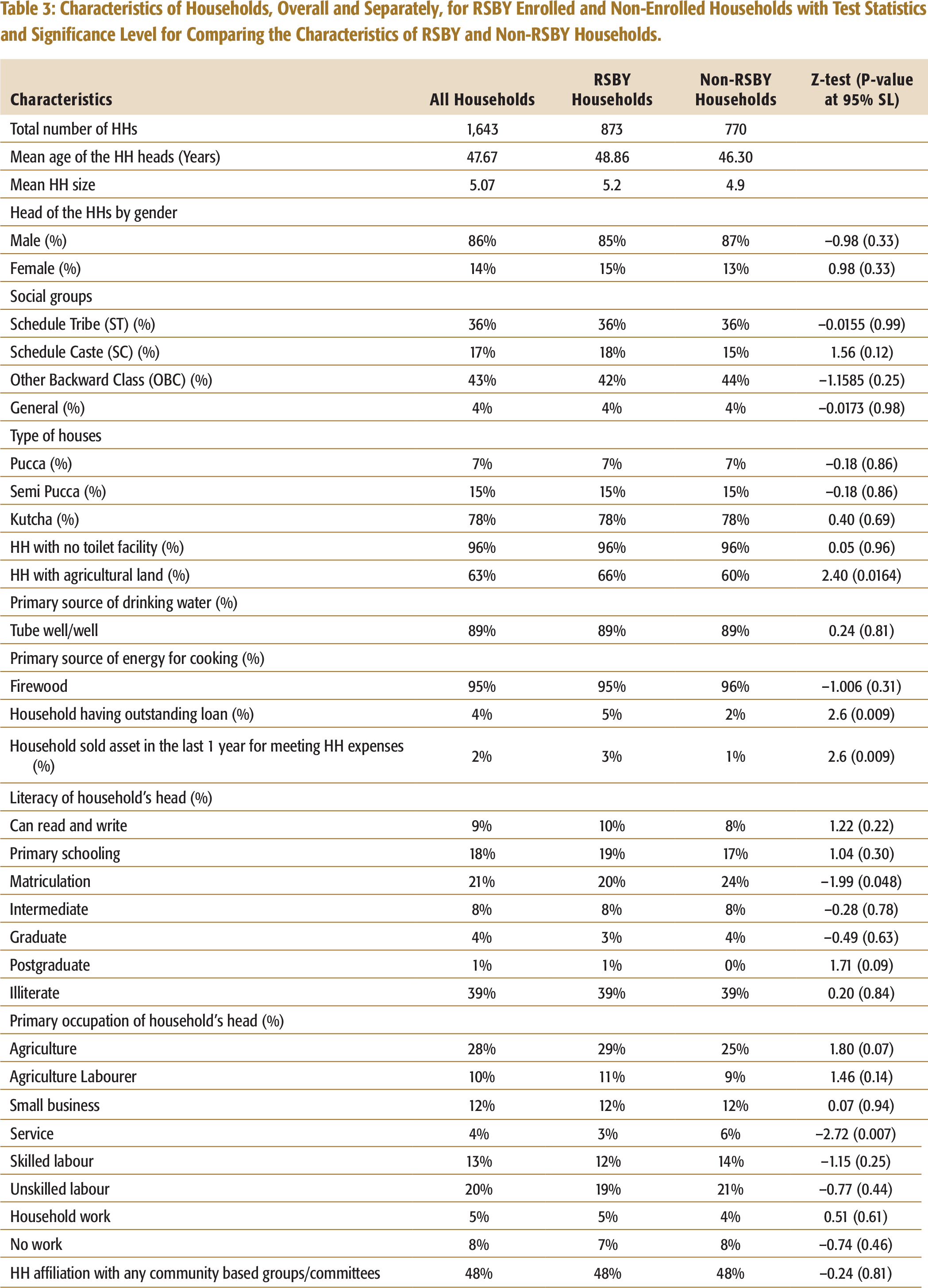
Characteristics of Households, Overall and Separately, for RSBY Enrolled and Non-Enrolled Households with Test Statistics and Significance Level for Comparing the Characteristics of RSBY and Non-RSBY Households.
INCLUSION AND EXCLUSION ERRORS IN RSBY
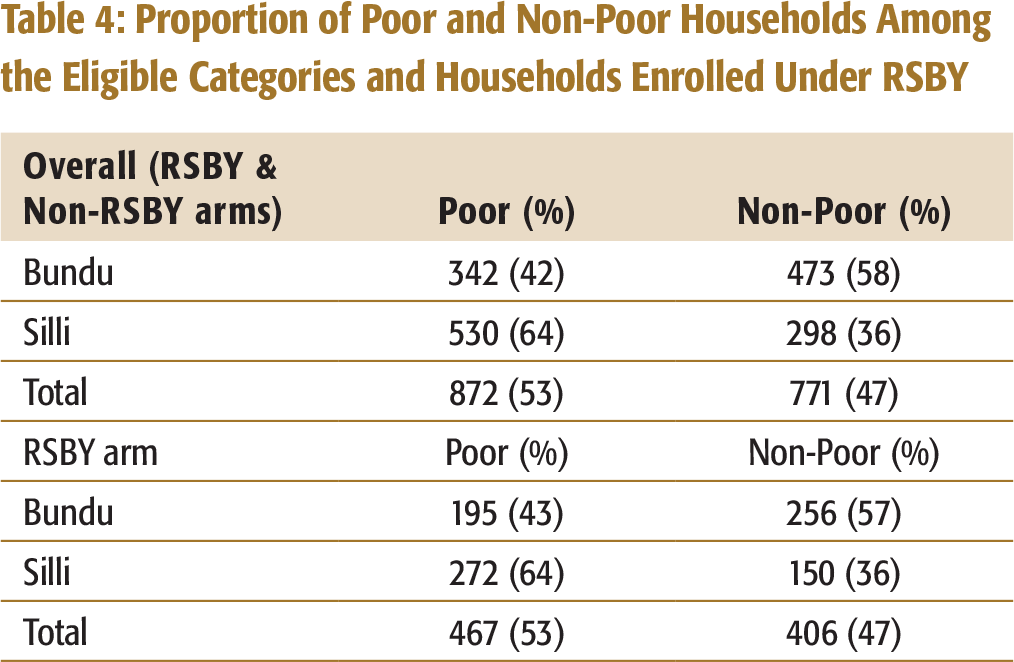
The success of any programme is primarily judged by its effective targeting. Targeting depends on eligibility, and for RSBY having a BPL number was the pre-condition. The household’s consumption data was used to calculate monthly per capita expenditure, and it was compared with the inflation adjusted thresholds of monthly per capita expenditure to assess whether the sampled BPL households were poor or non-poor (Ghosh, 2014; Planning Commission, 2013). In 2015, the inflation adjusted monthly per capita poverty line for rural area as approximately ₹ 1,200 and the corresponding figure for the urban area as approximately ₹ 1,700. The analysis showed that 47 per cent of the total households qualified as eligible even though they were non-poor, since they had a BPL card (refer to Table 4). Similarly, 47 per cent of the 873 RSBY enrolled households were non-poor. Similar discrepancies were found in other studies too (Dreze & Khera, 2010; Ghosh, 2011, 2014; Ram, Mohanty, & Ram, 2009).
Proportion of Poor and Non-Poor Households Among the Eligible Categories and Households Enrolled Under RSBY
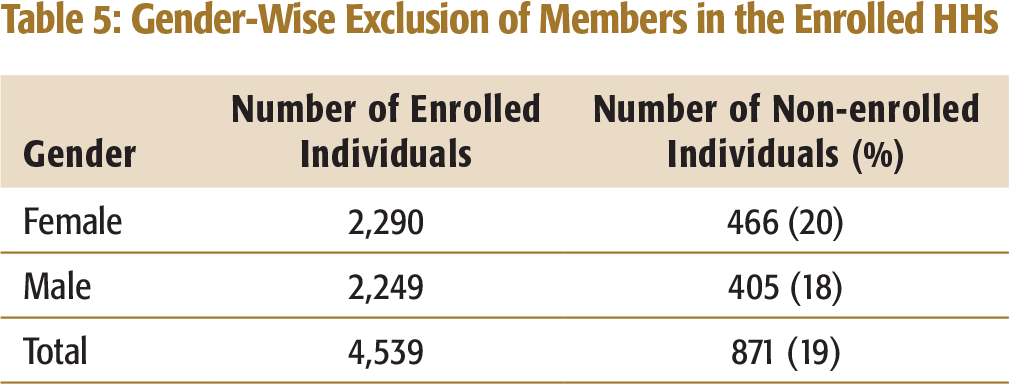
Gender-Wise Exclusion of Members in the Enrolled HHs
Age-Wise Exclusion of Members in the Enrolled HHS
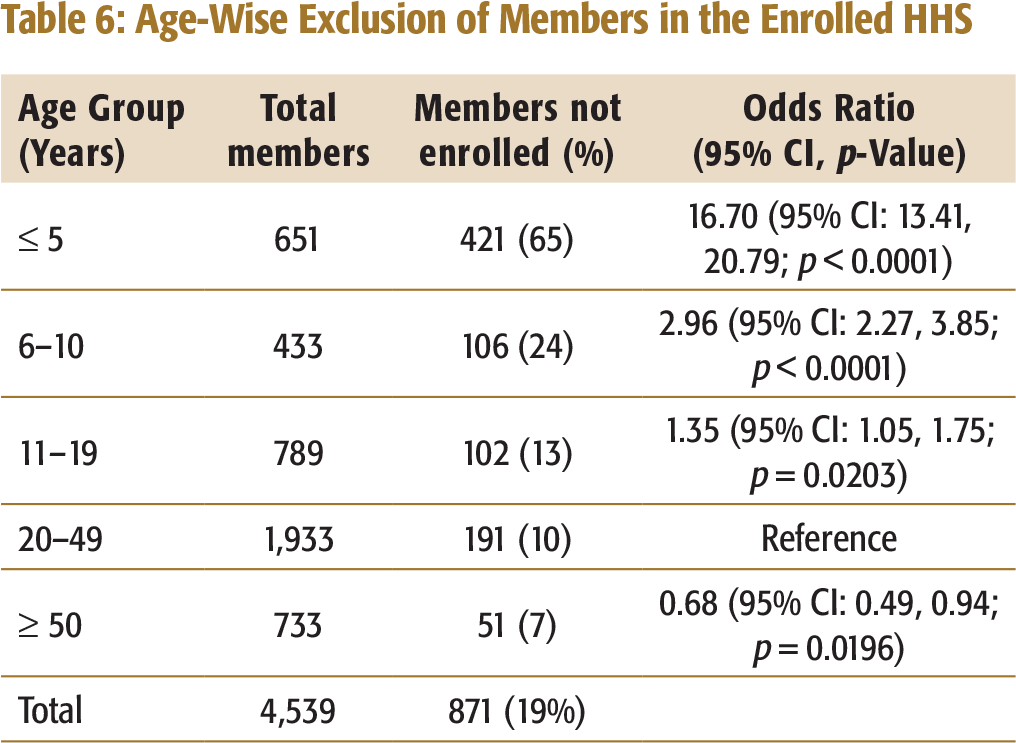
Exclusion error was also seen among high risk age group. Table 6 shows that out of the 871 excluded members from the enrolled households, about 65 per cent were below five years of age despite they are having higher risk of morbidity and mortality (Bassani et al., 2010).
The exclusion errors (Table 6) raise an important design and implementation issue. There is a need to revisit the maximum number of members in a family to be enrolled, as a lot of members are left out despite being eligible to get enrolled.
Multivariate Analysis to Understand Impacts of RSBY
Binary logistic regression analyses were performed in SPSS 20 software to identify significant determinants of hospitalization, incidences of CHE, and health expenditure-induced poverty, and to see the effect among the insured households on the aforementioned outcome indicators. Other independent variables taken were socio-economic and demographic status of households, households’ health events, health care service providers, and distance from the nearest service providers. The households were also categorized into quintiles using their consumption expenditure data. Quintile 1 was considered as poorest quintile and Quintile 5 as the least poor quintile. These were included in the analysis to see the outcome from the equity perspective.
Impact of RSBY on Hospitalization and Its Determinants
Hospitalization is known to be determined by many covariates. Hence, to see whether RSBY had improved uptake of hospitalization services among the enrolled households after controlling socio-economic and other factors, a binary logistic regression analysis was performed. Hospitalization status was taken as dependent variable. To assess whether RSBY had achieved its objectives of improving care-seeking (hospitalization) among socio-economically backward households, who were enrolled under RSBY, the analysis was done with the interaction of the RSBY dummy variable with dummy variables of income quintiles, social status, literacy of the household heads, their occupation, landholding of the households, and house structure. These indicators reflect the socio-economic status of the households. Other independent variables included in the regression model were household size, gender and age of the household heads, access to drinking water and toilet, distance from provider, and chronic illness of any family member. Alcoholism and smoking being high risk health behaviours were also taken as independent variables to see if they affected rate of hospitalization.
Determinants of Hospitalization Among the Studied Households
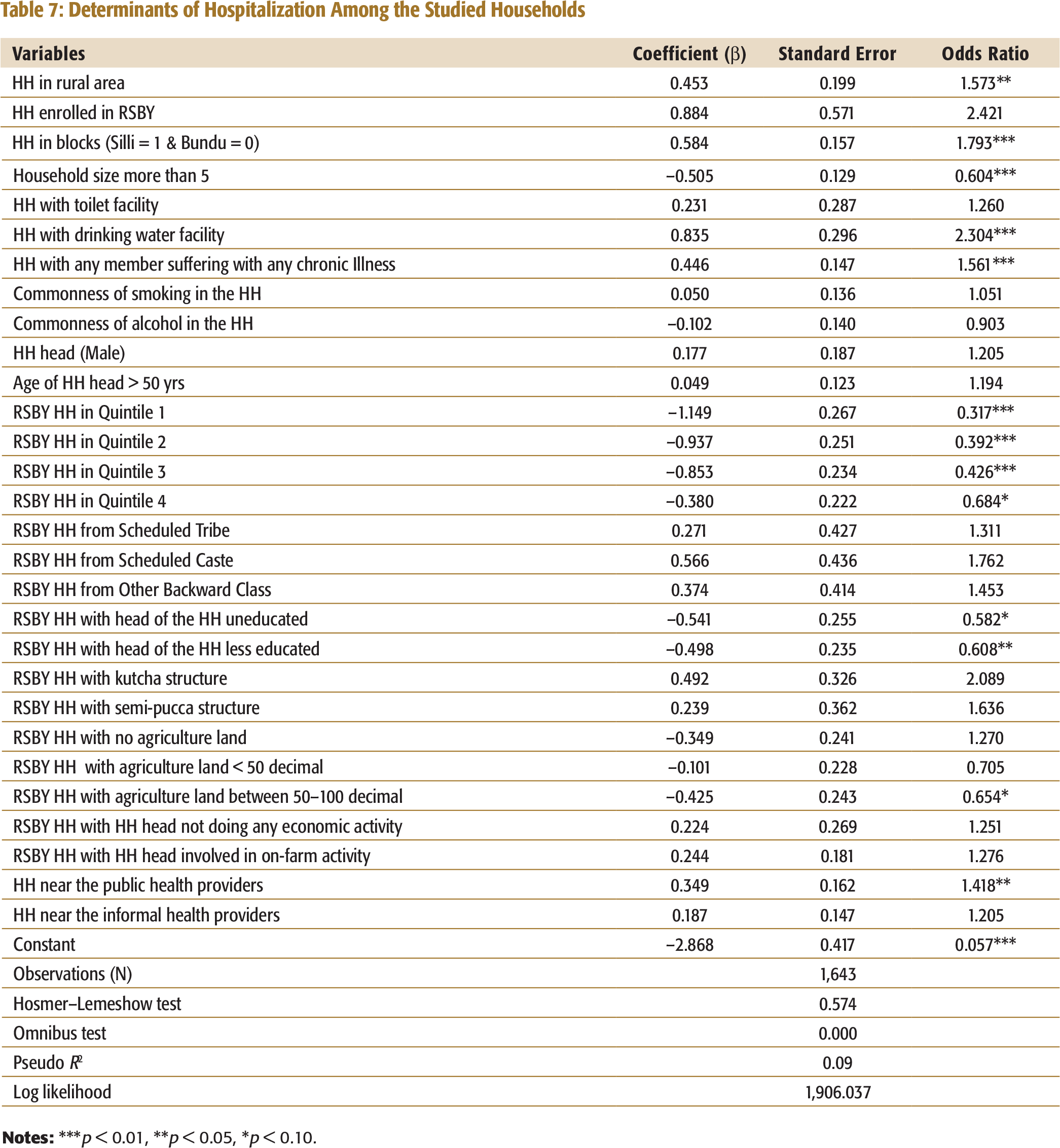
Households with any member suffering with chronic illness or those who lived near any public health provider sought more hospitalization services. Chances of hospitalization were higher among households in Silli block compared to Bundu block. Silli block had four hospitals which were empanelled to provide RSBY services, while in Bundu there was only one hospital. This may explain higher hospitalization rates. Higher proportion of tribal population in Bundu block and difficult terrain in some pockets with low public transport facilities may have been the factors for lower hospitalization rates in Bundu. Rural households sought more hospitalization services than those in urban areas. Households with large family size were less likely to seek hospital care.
In summary, the aforementioned analysis shows that hospitalization had not increased due to accessibility to government insurance scheme among the enrolled households. More importantly, care-seeking had been much lower among the enrolled households from economically and socially backward sections compared to the better off households, which is an area of concern. It is very important for such schemes to not only to perform better from the efficiency perspective by improving care-seeking among the enrolled households but also ensure that the benefit should also reach the economically and socially weaker sections of the society.
Impact of RSBY on Incidences of CHE and Its Determinants
When a household spends more than 40 per cent of its capacity to pay for health services, then the expenditure is called CHE (WHO, 2002; World Bank, 2004). Household capacity to pay refers to the non-subsistence expenditure, that is, the difference between the total household expenditure and their subsistence expenditure. Subsistence expenditure is defined as the mean food expenditure of households falling between the 45th and 55th percentiles of the total sample (Gnawali et al., 2009; Gotsadze, Zoidze, & Rukhadze, 2009; Wagstaff, 2008; Xu et al., 2003).
To see whether RSBY had reduced the incidence of CHE among the enrolled households—especially among those enrolled households who experienced hospitalization or had any childbirth in the last one year, after controlling for all socio-economic and other factors—a logistic regression analysis was performed. Incidence of CHE was taken as dependent variable and socio-economic status of household (gender, age, literacy, occupation status of head of the household, caste, household size, house structure, households with toilet and drinking water facility, agricultural land possession) as independent variables. Other independent variables included were distance from the nearest health provider, health events in the household in the previous year including cases of hospitalization or delivery, and who the service providers were in such cases, whether delivery was by caesarean section, and behavioural aspects of family members such as alcoholism or smoking. Enrolment status of households in RSBY and interaction of RSBY dummy variable with dummy variables of hospitalization and childbirth in the last one year were also taken as independent variables.
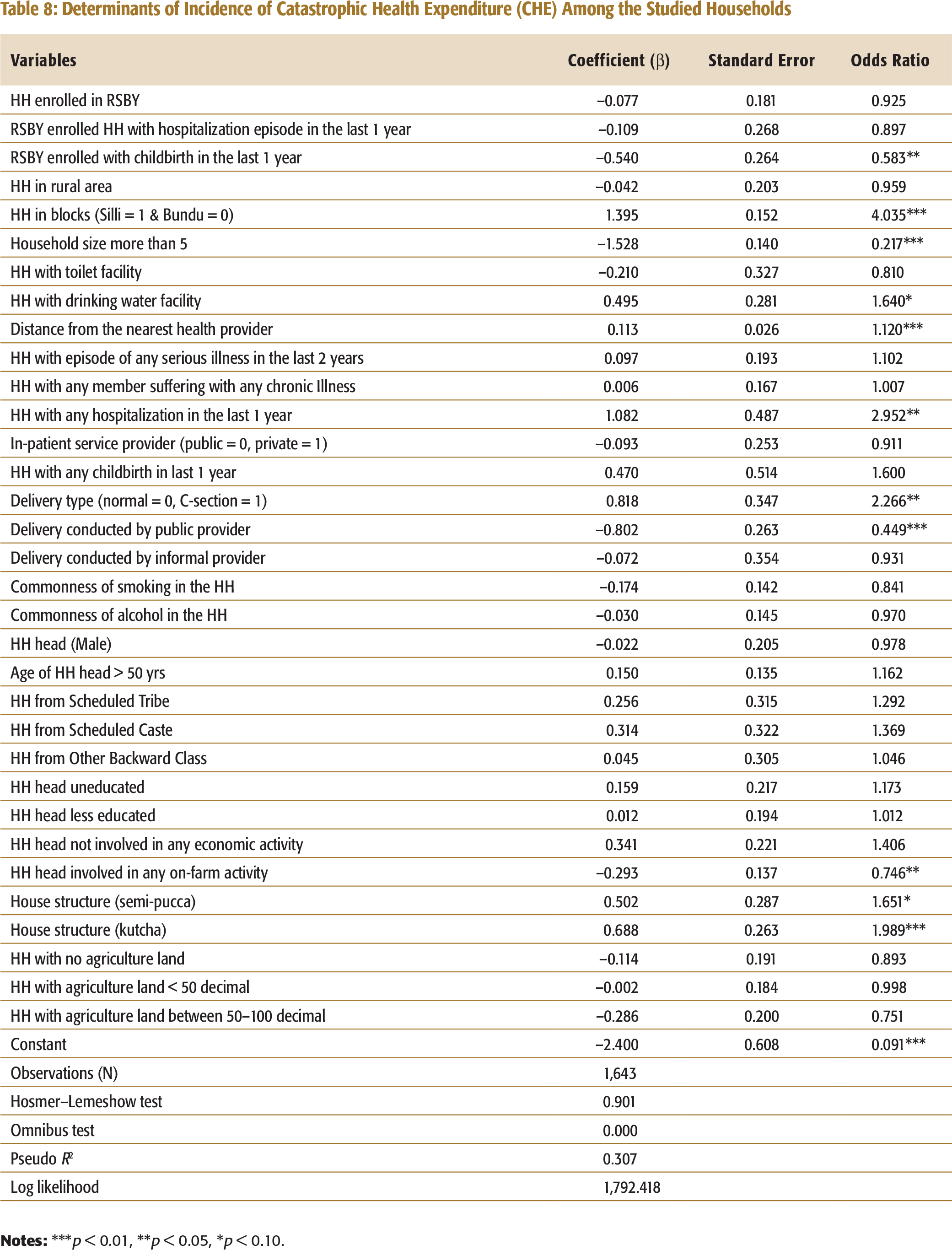
The analysis (Table 8) shows that RSBY had not impacted in reducing the incidence of CHE. Ideally, RSBY should, as that is one of the intended objectives of any publicly financed health insurance. The likelihood of CHE was very high among the households with any case of hospitalization in the previous year. We also examined whether incidence of CHE had reduced among those enrolled households which experienced hospitalization or had any childbirth in the last one year by interacting the RSBY dummy variable with dummy variables of hospitalization and childbirth. It was found that it did not reduce the burden of CHE among those enrolled households which had accessed in-
patient service in the last one year. As hospital expenditure is a direct cause of CHE and RSBY primarily covers hospital expenditure and promises to provide cashless service to the enrolled households at the empanelled hospitals, one would expect that the incidence of CHE should reduce at least among the enrolled households who received in-patient service from the empanelled hospitals. However, incidence of CHE had been
significantly reduced among the enrolled households with cases of any childbirth in the last one year. This is a positive outcome, as RSBY covers the cost of institutional delivery from the empanelled hospitals. Also, the likelihood of CHE was less when deliveries were handled by a public health provider or if it was a normal delivery compared to a caesarean section.
Determinants of Incidence of Catastrophic Health Expenditure (CHE) Among the Studied Households
Impact of RSBY on Incidence of Health Expenditure-Induced Poverty and Its Determinants
One of the success indicators of a health finance programme is its impact on reducing the incidence of health expenditure-induced poverty. Poverty headcount analysis was done by looking at the households’ monthly per capita medical expenditure as part of households’ monthly per capita consumption expenditure to assess the proportion of households pushed below the latest official poverty line due to medical expenditures (Planning Commission, 2013). It is measured by comparing the poverty headcount before and after OOP health payments. The ‘pre-OOP poverty headcount’ was calculated by comparing households’ consumption expenditure, gross of payments for health care with the official poverty line. Similarly, the ‘post-OOP poverty headcount’ was computed by netting out the OOP health care payments from the households’ consumption expenditure and comparing with the same official poverty line. The number of individuals slipping BPL because of OOP expenditures was assessed by calculating the headcount difference between post-OOP and pre-OOP payments (Bassani et al., 2010; Garg & Karan, 2008).
With the hypothesis that RSBY would effectively reduce incidence of poverty among the enrolled households after controlling for all socio-economic and other factors, a logistic regression analysis was performed with the households which were above the poverty line (APL) prior to incurring any health expenditure and at risk of falling to BPL due to it. Incidence of poverty due to health expenditure was taken as dependent variable; the independent variables being socio-economic status of household (gender, age, literacy, and occupational status of head of household, caste, household size, house structure, access to drinking water and toilet, agricultural land possession). Other independent variables included in the regression model were enrolment under RSBY, health events such as cases of hospitalization or delivery of any family member in last one year, chronic illness of any family member, and provider type for health events.
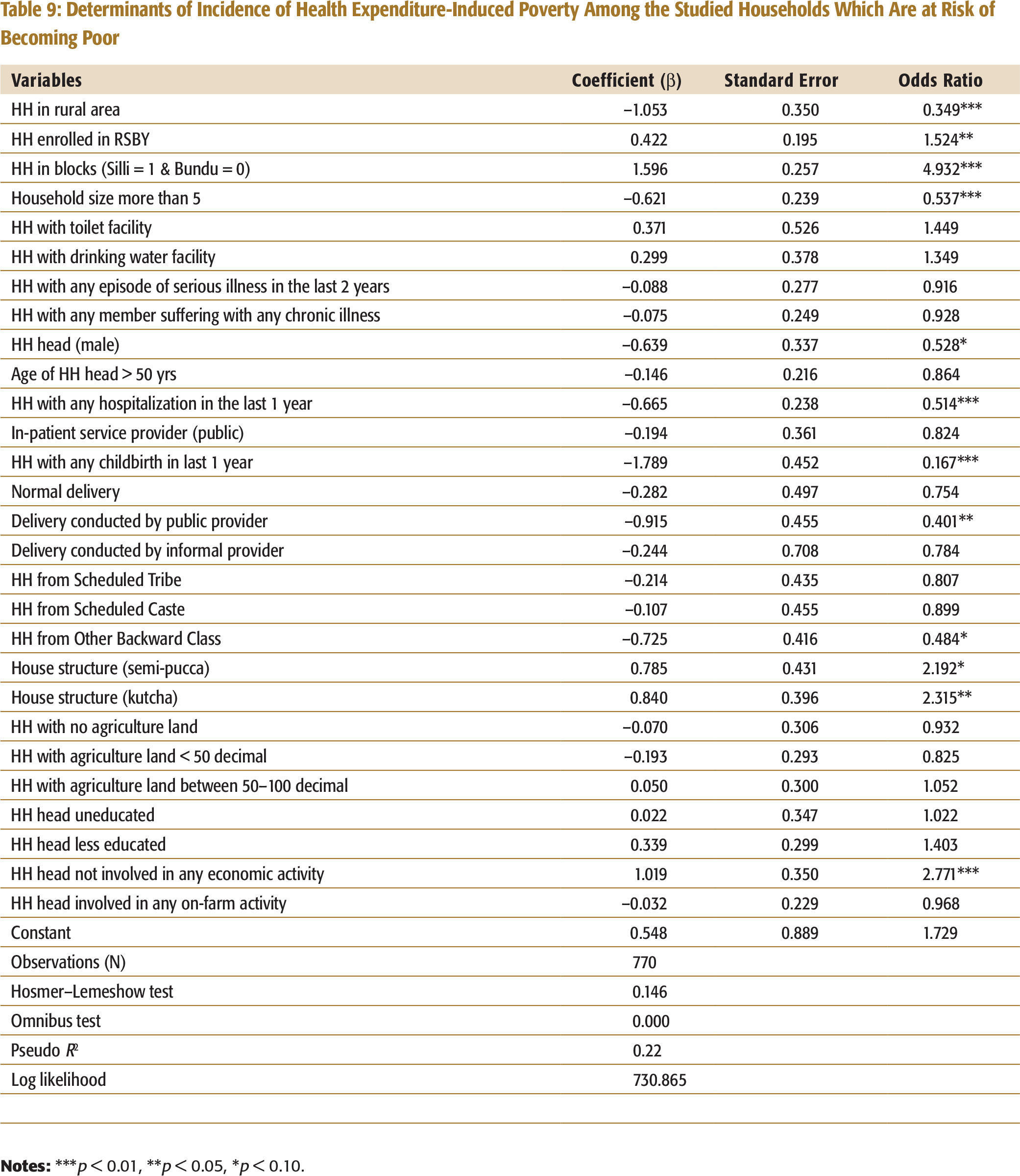
It was found that among the RSBY enrolled households, who were APL before incurring health expenditure, incidence of health expenditure-induced poverty had been significantly increased (Table 9). This shows that health expenditure had actually pushed the enrolled households BPL.
Incidences of health expenditure-induced poverty were lower among the rural households when compared to urban households. This was because the monthly per capita consumption expenditure in the rural areas was higher than its poverty line threshold in most of the cases (51% of the households) unlike in the case of urban areas, where such cases were low (36% of the households). Also, in rural areas, health expenditure was less than urban areas. These reasons can possibly explain the higher rates of health expenditure-induced poverty in the households in Silli block when compared to that of Bundu block. Incidence of health expenditure-induced poverty was very high in the male-headed households because they incurred more health expenditure. It was
Determinants of Incidence of Health Expenditure-Induced Poverty Among the Studied Households Which Are at Risk of Becoming Poor
CONCLUSION AND DISCUSSION
RSBY is a government-sponsored health insurance programme, for the resource-poor households, which primarily aims at providing financial security from secondary health care expenditure. It aims to cover around 35 per cent–40 percent families that are officially BPL. This study has tried to analyse the performance of RSBY from the perspectives of equity and efficiency, looking at the demand-side issues. The study shows that RSBY had not been able to successfully increase care-seeking among the enrolled households. It has also failed in reducing the burden of CHE among the enrolled households as well as enrolled households who experienced hospitalization. From the equity lens, hospitalization, even among enrolled households from economically poorer sections, was significantly low. In contrast, incidence of CHE was very high among them. Further, the scheme significantly increased the incidence of health expenditure-induced poverty among the enrolled households who were APL, prior to incurring health expenditure. This shows that RSBY had not performed efficiently in improving overall care-seeking, reducing the burden of CHE, or reducing the health expenditure-induced poverty.
Households from the poorest quintiles have higher health risk exposure, and yet lowest access; therefore, it is important to frame policies that enable access to free or affordable health care. Theory of insurance envisages that once barrier of affordability is reduced through financial protection from expenditure, the utilization of health care services increases among the economically poor. However, the study found that the care-seeking, even among the enrolled economically poorer households, was significantly lesser than the better-off households thus belying the stated objective of equitable access.
An important concern that the study highlights is targeting. The study found that around 47 per cent of households that got enrolled in the scheme were non-poor. However, some of the eligible socio-economically poor households may have been excluded because RSBY uses the old BPL list. This is a significant design problem. The government needs to address how to define poverty such that the most vulnerable resource-poor households should be part of the scheme. Though government is trying to enlarge the beneficiaries’ base by bringing in more parameters of vulnerability for inclusion (even without a BPL card), it is still a major challenge for the government to appropriately target eligible and underserved families.
While there is a ceiling on the maximum number of members per household who could be enrolled, there is no mechanism to check if all eligible members from households had been enrolled. The study found that about 19 per cent family members had remained excluded even after the household (under the ceiling limit) had been enrolled under the scheme. The excluded members generally were children (65%) who may have higher need for hospitalization as children less than 5 years are at a higher risk of morbidity and mortality compared to other age groups. The government needs to relook the strategy for effectively creating awareness among the eligible communities to ensure enrolments and benefits from the scheme. It also needs to iron out some of the programme implementation issues so that intra-household members should not be left out from the scheme once the households have been identified as most vulnerable.
There is a need for strong regulatory mechanism with adequate resources for effective monitoring the scheme at the ground level. State Nodal Agencies that have been assigned the role of monitoring need to ensure that effective communication be made with beneficiaries to bridge the knowledge gap and ensure that the most vulnerable and marginalized populations get enrolled. There is a need to oversee claim settlement ratio against the hospitalization rate to ensure that the benefits reach the intended beneficiaries.
Finally, out-patient care is not covered under RSBY. However, the finding from the study show that expenditure towards out-patient care was a major contributor for increasing the health expenditure-induced poverty among the households which were APL before incurring health expenditure. Other studies had also shown that out-patient care could be catastrophic in nature in the context of India (Devadasan, 2011; Selvaraj & Karan, 2012). Hence, it is important for the policymakers to take cognizance of the calamitous nature of out-patient health expenditure on extremely poor families and cover such expenditures under the scheme. This is especially true for making drugs and medicines affordable and accessible, which constitute nearly 62 per cent of out-patient cost, 44 per cent of in-patient cost, and 39 per cent of delivery costs. Government should promote generic medicines and drugs making them easily available so that medicines become affordable to BPL households.
India currently spends close to 5 per cent of GDP towards health of which only 1.4 per cent is contributed by the government (Wagstaff, 2008). Remaining 3.6 per cent of total health expenditure is privately borne with a majority share being borne by the households. The public health delivery system is currently underfunded, understaffed and lacks adequate infrastructure, and has failed to provide appropriate and adequate health care services to the people at an affordable price. Though the study found that those who sought care from the public health providers had lower chance of CHE and health expenditure-induced poverty. It also found that 77 per cent of the in-patient care and 59 per cent of the out-patient care were sought from private providers who were comparatively very expensive. Besides 27 per cent of out-patient care was sought from informal providers.
Overall, RSBY appears to be an unviable policy for providing financial security to the enrolled households and increasing care-seeking. The policy perhaps would not help in achieving the goal of universal health coverage. Hence, it is important for the government to strongly consider strengthening public health delivery systems, which provide equitable health care services- preventive, promotion, and curative to all at a lesser cost with better health outcomes. The study findings also show that care-seeking at the government facilities was less expensive when compared to private facilities.
LIMITATIONS
As the survey was retrospective in nature, some cases of hospitalization and childbirth within the reference period of one year may have been missed (Ghosh, 2011). Another methodological limitation is that the study was a controlled-cross-sectional study which did not capture the whole range of high and low expenditures throughout the year. Ideally, the study should have been a longitudinal study to capture whole range of health and other expenditure throughout the year. We tried to cover all BPL households during the qualification round, but there could be cases where some BPL households were left out. In some cases, it was found that families had migrated. Response bias is possible particularly in the cases of collecting treatment costs as we took responses from the family members only, and could not check with the hospital records. Only when a family had received benefit from RSBY, the benefit amounts could be cross-checked with the discharge slip.
Another limitation of the study is that since it was done at household level, it only captured the variables and information from the demand side, that is, taking the household’s perspective. Supply-side variables, issues, and problems could not be captured because the study did not collect information from the government, insurance companies, health care providers/hospitals, or other stakeholders who are playing key roles in its implementation.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received financial support for the research from Welcome Trust, UK through University College London (UCL), UK and Ekjut, India.