
Abstract

Executive Summary
Though exit surveys are considered important tools for ascertaining quality and demand for healthcare services, apprehension about the reliability of responses in such surveys are not misplaced. It has been argued that ‘courtesy bias’ may lead respondents to give approving responses, especially if interviewed in the premises of the institution. This study examines:
• how users' perceptions are shaped,
• if there is bias in these perceptions and
• how these perceptions can be used in improving efficiency of the institution as well as changing the healthcare policy and practices.
The study does not find evidence that reported satisfactions are biased positively in the exit survey, especially for subjective questions regarding behaviour of health personnel. The responses are certainly not biased for relatively objective questions about infrastructure condition, supplies and services of the institutions. The survey does provide useful information on the determinants of consumer satisfaction with explanatory variables like dimensions of respondents' characteristics, if respondents availed special benefits and cost incurred by them.
The study reveals that it is not individual factors but interactions of factors that shape responses. By and large satisfaction with behaviour of health professionals improves if the respondent has availed benefits of services provided. But this process is influenced by institutions as well as expenses incurred in availing these facilities. The interaction between household income and institution shapes the respondents' satisfaction towards infrastructure. Dissatisfaction to provided services reduces if respondents are availing benefits of medicine compared to those not availing this benefit. Nevertheless, dissatisfaction reduces sharply only if respondents are paying relatively less cost for the services.
Findings conclusively prove that perceptions on services provided are also shaped by, apart from other factors, perceptions about the behaviour of health personnel as well as infrastructure.
The emergence of private players as major healthcare providers has resulted in the exposure of the clients to better quality of services and improved experiences. One of the key strengths of private service providers is that they place customer satisfaction at the centre of their processes. Private sector companies recognize that satisfied clients sustain business, produce positive word-of-mouth, and become loyal to a particular brand—an approach that the public sector fails to recognize (Williams, Schutt-Ainé, & Cuca, 2000). As a result, there is an increasing pressure on the public health institutions to improve the quality of their services. An urgent need to reinvent the processes and reorient the approach to service delivery is felt among policy makers, government and clients. Recognizing this need, policy makers have emphasized the importance of client-centric governance in improving accountability and responsiveness in governance. A logical first step towards this end would be to collect baseline data on clients' experiences with the public health services and using them to improve the quality of services. Across the globe, client satisfaction exit interviews have emerged as a way of Quick Investigation of Quality (QIQ, 2001) of certain aspects of healthcare—an idea propagated by the MEASURE evaluation project of Global Health Bureau of the United States Agency for International Development (USAID).
Until recently, any effort to improve the quality of health services has taken a top-down approach. However, now, the subjective side of quality has also been recognized as important, and clients' opinions and levels of satisfaction are used to assess the quality of services. There are no institutionalized ways in which clients can express their opinions, report their negative experiences, and provide feedback to improve quality of services. Exit interviews provide a quick and easy way to collate data on client satisfaction. Also, as exit interviews are conducted as soon as the client has a lived experience with the service provider, the data can be expected to be fairly reliable. However, there are also criticisms against this method as a valid source of data, as many argue that respondents in many cases do not openly report about negative experiences when they are within the premises of the service provider institutions. The present article argues that exit interviews could be indicative of the specific aspects of service delivery that need reforms and also help in getting the nuts and bolts of health institutions right. A study was conducted by Samarthan, Centre of Development Support (2011) which included institutional audits of the Sub-Health Centres (SHCs), Primary Health Centres (PHCs) and Community Health Centres (CMCs) in 12 districts of Madhya Pradesh. Structured questionnaires were used based on the IPHS 1
Indian Public Health Standards
Madhya Pradesh: A Brief Profile
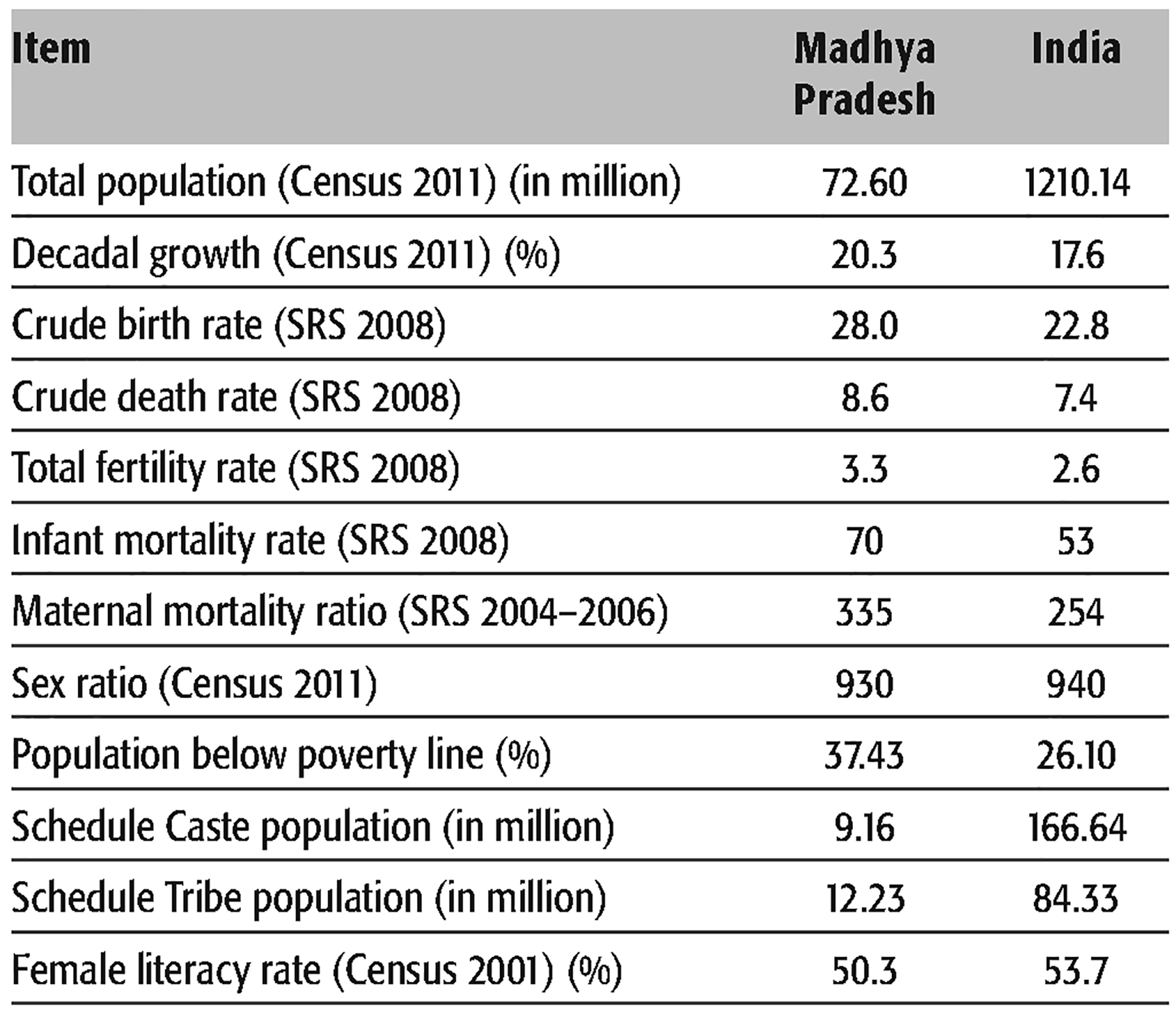
The state of Madhya Pradesh has an area of 308,245 sq. km, a population of 72.6 million, and a population density of 236 per sq. km. There are 48 districts, 313 blocks and 55,393 villages. 2
The comparative figures of major health and demographic indicators are given in Tables 1 and 2.Number of Respondents Having a Bank Account
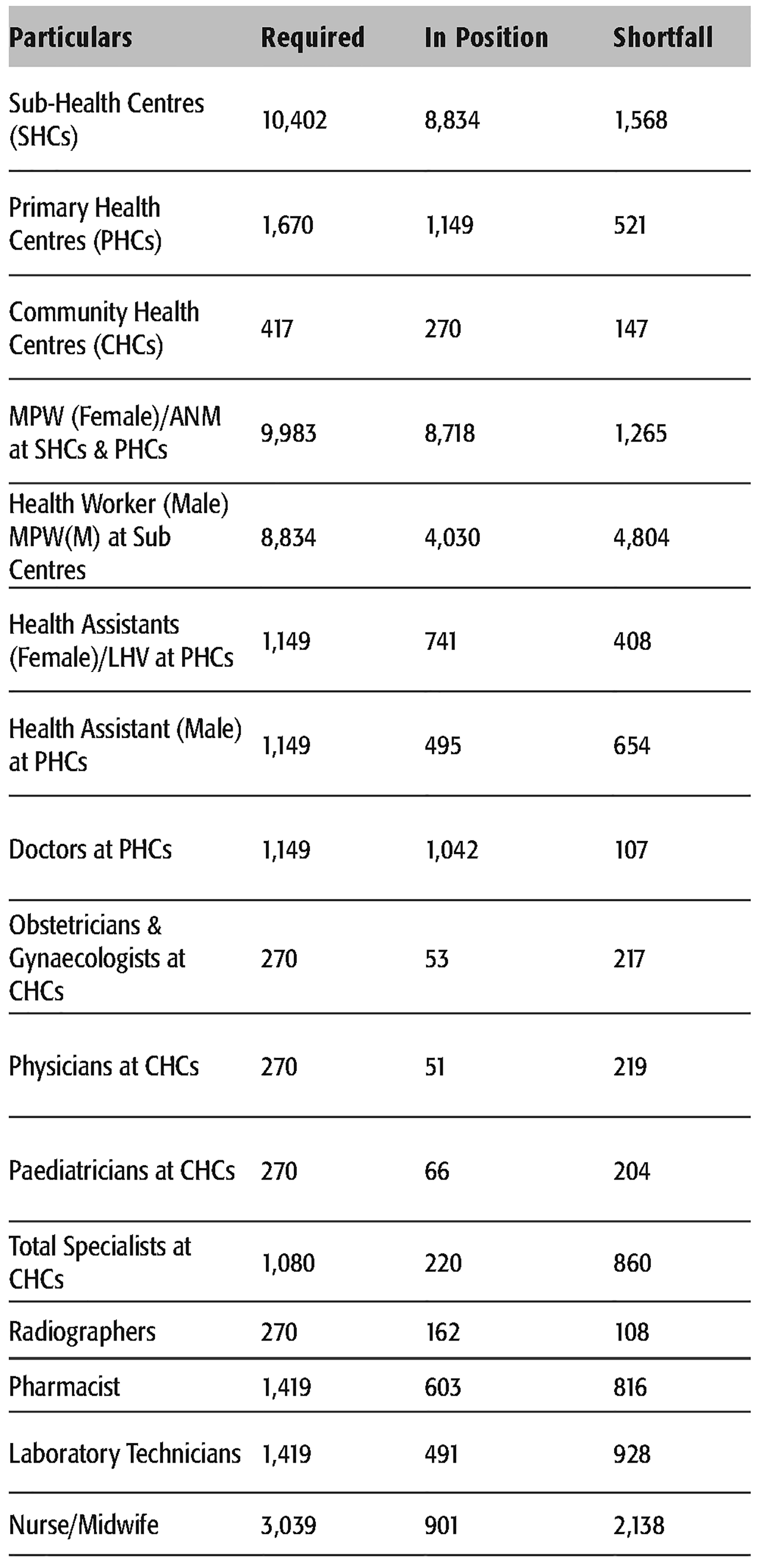
Health Infrastructure of Madhya Pradesh
Understanding Client Satisfaction in Public Health Services
Indicators of Quality of Health Services
Inter-linkages between clients' satisfaction, quality of services, access to services and sustainability of public institutions play vital roles in ensuring effective governance in today's world. For instance, dissatisfied clients will opt out of the services, spread messages about their negative experiences discouraging others to access the services. This in turn will result in the breakdown of public institutions. Clients' satisfaction is therefore the key to their decisions to continue accessing public services and is essential to long-term sustainability. Dissatisfaction among clients could be either due to poor quality of services like cumbersome processes, untrained/unhelpful personnel or lack of facilities because of issues related to accessibility—distance between the clients' place of residence to the Public Health 3
Sample Registration System.
As a part of a large-scale effort to reinvent healthcare institutions, client satisfaction surveys are increasingly being promoted as a method of understanding quality of health services and the needs and expectations of clients from these institutions. Evidence from healthcare research across the globe reveal that research techniques such as client exit surveys provide a quick and inexpensive way of determining specific areas of health services where quality could be improved. Exit interviews have become a popular way of assessing client satisfaction in developing countries like Ethiopia (Fekadu, Andualem, & Yohannes, 2011; Tesfaye, 2005), Madagascar (Glick, 2007) and Bangladesh (Aldana, Piechulek, & Al-Sabir, 2001). The Department of Community Medicine, Midnapore Medical College, West Bengal conducts institutionalized exit interviews so as to understand clients' satisfaction levels as an indicator of their performance (Das et al., 2010). These exit interviews are useful for highlighting the inadequacies in the basic aspects of service delivery that affect the quality of clients' experiences. They also provide evidence of whether specific policies have their desired effects. They are found to be easier to administer, less expensive, and provide rapid feedback when compared with client report cards. While exit interviews are being widely used in healthcare research, one must also be aware of the possible issues related to the reliability of the data collected through exit interviews. One of the biggest criticisms of exit interviews is the problem of ‘courtesy biases’ (Glick, 2007). Courtesy bias results from the reluctance of the respondents to express negative opinions of service while they are within the premises of the service provider during the exit interviews. This could result in over-reporting of satisfaction levels.
As satisfaction and its measurement are important for health planning, Crow et al. (2002) reviewed 139 articles on determinants of satisfaction. Their review provided evidences on two groups of factors: first, those relating to the characteristics of respondents and second, those relating to healthcare delivery. No firm conclusions can be drawn on the relationship between levels of satisfaction and gender (Crow et al., 2002). It has been argued that satisfaction is high when favourable experiences match favourable expectations and low when negative occurrence reinforces negative expectations (Linder & Stewart, 1986; Swan et al., 1985). Studies also confirm a positive relationship between satisfaction and previously recorded levels of satisfaction (Gray, 1980; John, 1992). In fact, evidence indicates that levels of satisfaction get enhanced when the patients' wishes are met and dissatisfaction arises when they are not (Jackson, Chamberlain, & Kroenke, 2001; Weingarten et al., 1995). Doctors' communication skills and the extent to which the patients are open to reasoned arguments also help in shaping the levels of satisfaction (De La Cuesta, 1997). Fitzpatrick (1991) and Pickering (1993) have advocated the need to educate consumers about appropriate care and to manage their expectations about what can realistically be provided.
There is evidence that poorer physical health (Annandale & Hunt, 1998; Hsieh & Kayle, 1991; Rogut, Newman & Cleary, 1996) and low quality of life (Weingarten et al., 1995) are associated with lower levels of satisfaction. Nonetheless, it has also been found that older respondents are significantly more satisfied than others (Al-Bashir & Armstrong, 1991; Cleary et al., 1992). In general, the findings about relationship between socio-economic indicators—education, social class, occupation and income—have been inconclusive and at times inconsistent ( Bertakis, Roter, & Putnam, 1991; Cohen, 1996; Crow et al., 2002; Khayat & Salter, 1994). It has also been suggested that a personalized approach of physician is appreciated by healthcare seekers (Hjortdahl & Laerum, 1992; Holloway, Matson, & Zismer, 1989). Studies investigating levels of satisfaction with in-hospital care have identified quality of patient –practitioner relationship (Cleary et al., 1992; Howie et al., 1998) and discussions with the practitioner (Calnan et al., 1994; Coyle, Calnan, & Williams, 1992; Roghmann, Hengst, & Zastowny, 1979; Snell, 1996; Williams & Calnan, 1991) as most important factors governing client satisfaction. While in-hospital satisfaction has been reported to be lower in government hospitals compared to private hospitals (Fleming, 1981), nursing strain and exhaustion have been found to adversely affect patient satisfaction (Leiter, Harvey, & Frizzell, 1998). On the other hand, studies on out-patient care suggest that professional standards and interpersonal relationships are of prime importance to patients (Bishop et al., 1991; De La Cuesta, 1997; Fitzpatrick, 1991). Longer consultation and personalized approaches are also appreciated by out-patients (Hjortdahl & Laerum, 1992). It has been argued that affective behaviour like warmth and respect (Kenny, 1995), courtesy and apathy (Comstock et al., 1982) and sensitivity and understanding (Treadway, 1983) are associated with higher consumer satisfaction.
Monitoring users' satisfaction is important for maintaining service quality in treatment (Crow et al., 2002). Moreover, these findings can affect health outcomes (Bishop et al., 1991; Fitzpatrick, 1991) as unsatisfied and frustrated patients may not respond fully to therapeutic interventions (Strasen, 1988). With respect to information exchange, evidence shows that satisfaction is higher with feedback and discussions about treatment (Brody et al., 1989; Hall, Rote, & Katz, 1988; Jackson et al., 2001). Despite these assertions, several problems arise while measuring satisfaction (Williams, 1994), which weaken the policy implications of evidence-based advocacy, emanating from these findings. Specifically, individual's judgements reflect their own circumstances and background, and do not necessarily lend themselves to objective measurement. If expressed satisfaction results from users' knowledge and expectations, the comments on quality of services may remain uncharted in these responses. Therefore, it is desirable to separate subjectivity, emanating from expectations, from the objectivity of service delivery quality. Crow et al. (2002) suggest that further research is warranted with respect to methods adopted especially on timing of the survey, bias introduced by interviewers and how these exit interviews may be incorporated into healthcare decision-making.
This article analyses the findings from the exit interviews with an objective to understand (i) how the perceptions are shaped; (ii) could the quality of healthcare infrastructure and services be taken seriously for advocacy; and (iii) feedback from health administration on the findings. This exercise will reveal whether the client satisfaction exit interviews are indicative of the institutional and procedural aspects of the public health institutions. Thus, exit interviews could be used as a practical way of investigating clients' satisfaction with respect to accessibility and quality of services.
Data and Methods
Sampling Design
The present study was spread across the different geographical regions of the state. It covered 12 districts where Samarthan (2011) works intensively on governance issues related to NREGA, 4
National Rural Employment Guarantee Act.
National Rural Health Mission.
Right to Information.
Sample of Individual Respondents
Data and Analysis
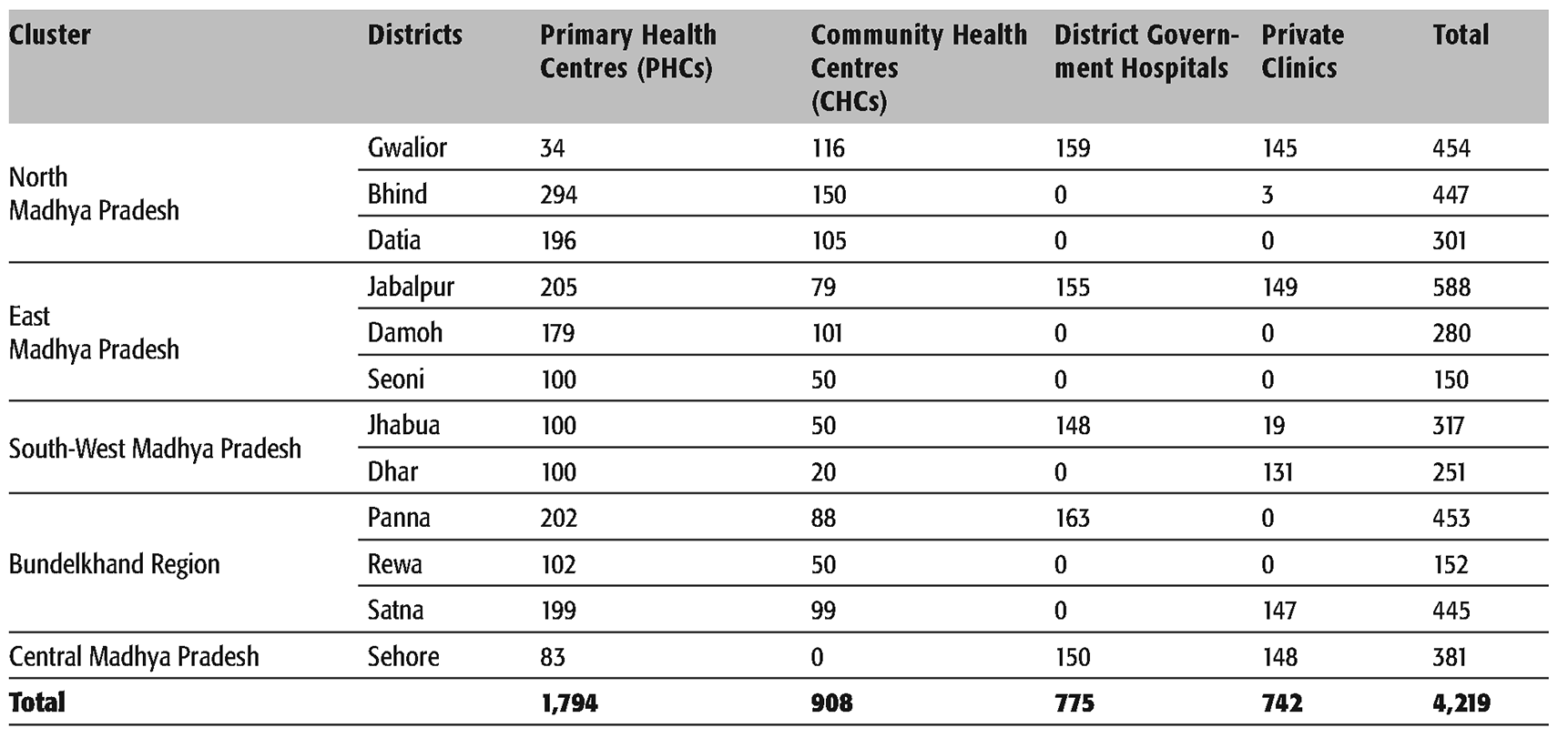
In each of the 12 districts, 1 CHC was selected randomly. In this CHC, 5 PHCs were randomly selected. A total of 4,219 individuals (3,308 out-patients and 911 in-patients) were interviewed from the PHC, CHC, district hospitals and private clinics to understand their perception and experiences of healthcare services. The data was collected between July 2010 and August 2010. Respondents attending an out-patient consultation were randomly selected on attendance and requested to complete the exit interview questionnaire. The research was conducted through a structured exit interview schedule which was used to collect data on the socio-economic background of the respondents, experiences of using the public health institutions, and the levels of satisfaction with respect to the quality of services. The key method used to analyse the data is quantitative. Tabular analysis is used to understand the degree of association between socio-economic characteristics of respondents and the level of satisfaction reported by respondents. This identified the main factors that were used in analysis of variance (ANOVA), which explained variations in satisfaction levels, as a cause-and-effect method. Although the present analysis has heavily relied on ANOVA, there are some sophisticated techniques—like Logit analysis—to explain the probability of being satisfied rather than not owing to changes in characteristics of respondents, and logistic regression—that can be applied. As the data on the level of satisfaction is ordinal, it was thought appropriate to use Analysis of Variance to identify factors that explain variations in patient satisfaction. Moreover, the latter techniques have stringent assumptions, making the results difficult to interpret, if assumptions are not met (Field, 2009). On the other hand, the assumptions of ANOVA are robust and variations from assumption, in practice, do not significantly affect the results (Field, 2009). Nonetheless, it is worth mentioning that though the variables, hypotheses and relationships tested in the article have already been studied before (see, for details, the literature review), the analysis has elements that lead to insights for policy formulation.
Exit Survey: Understanding Feedback from Clients
Percentage Level of Satisfaction of Patients

Two important and inter-related questions that we encounter in clients' feedback are: Are these opinions and reported experiences a valid conclusion on quality of services? This is an issue of methods used in generating the data and consistency in the patterns of the reporting. The second issue is: If these results are acceptable, how to use these variations as an advocacy tool? Before turning to the second issue, it may be worth reminding ourselves that as the OPD patient-exit survey was conducted outside the institutions, the likelihood of ‘courtesy bias'was relatively low. Moreover, if the proportion of highly satisfied or highly dissatisfied patients is less than 3 per cent and those who are not satisfied are about 42 to 57 per cent, the pattern of responses seems to be falling around averages rather than extreme. The findings thus reflect upon an expression of discontent that a public service provider may anyway face in the course of providing healthcare services. Therefore, by considering these responses as genuine expressions of satisfaction levels, the authors are not committing any bias. The analysis in the next section also confirms this conclusion.
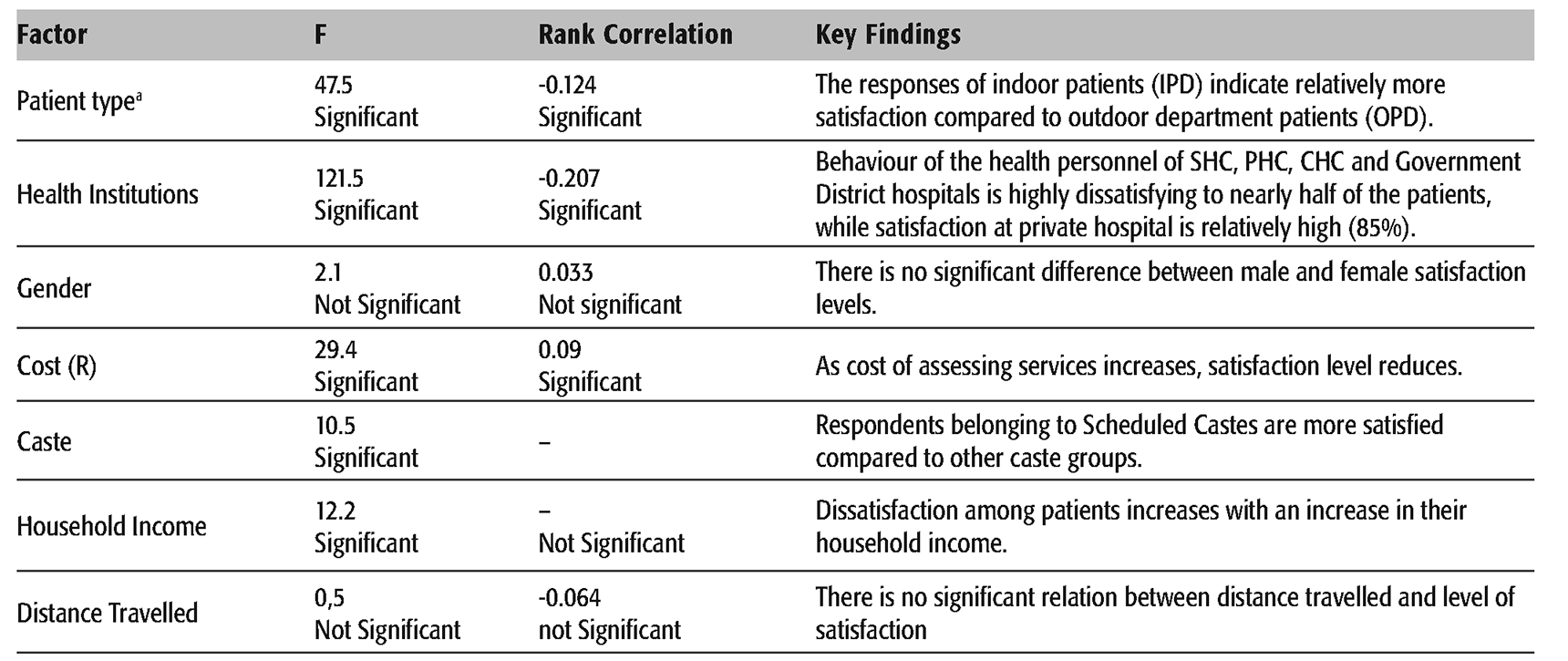
To begin with, we are raising an important question: Do the respondents differentiate in the healthcare services based upon their characteristics? Therefore, the factors that are significantly associated with the satisfaction levels are first identified and then an attempt is made to understand how these important (significant) factors taken together explain the variations in the levels of satisfaction. Tables 5 through 7 provide evidences (chi-square and rank correlation) for significant variation in the relationship between satisfaction level(s) and the factors: (i) behaviour of health professionals, (ii) infrastructure and (iii) services and the following key characteristics of the respondents namely: (i) patient type, (ii) health institutions accessed, (iii) gender, (iv) caste, (v) income of respondent, (vi) distance travelled to access health institutions and (vii) cost incurred in availing services.
Analysis Using Individual Factors
Satisfaction with Behaviour of Health Professionals
Satisfaction a on Behaviour of Health Professionals of the Institutions
a
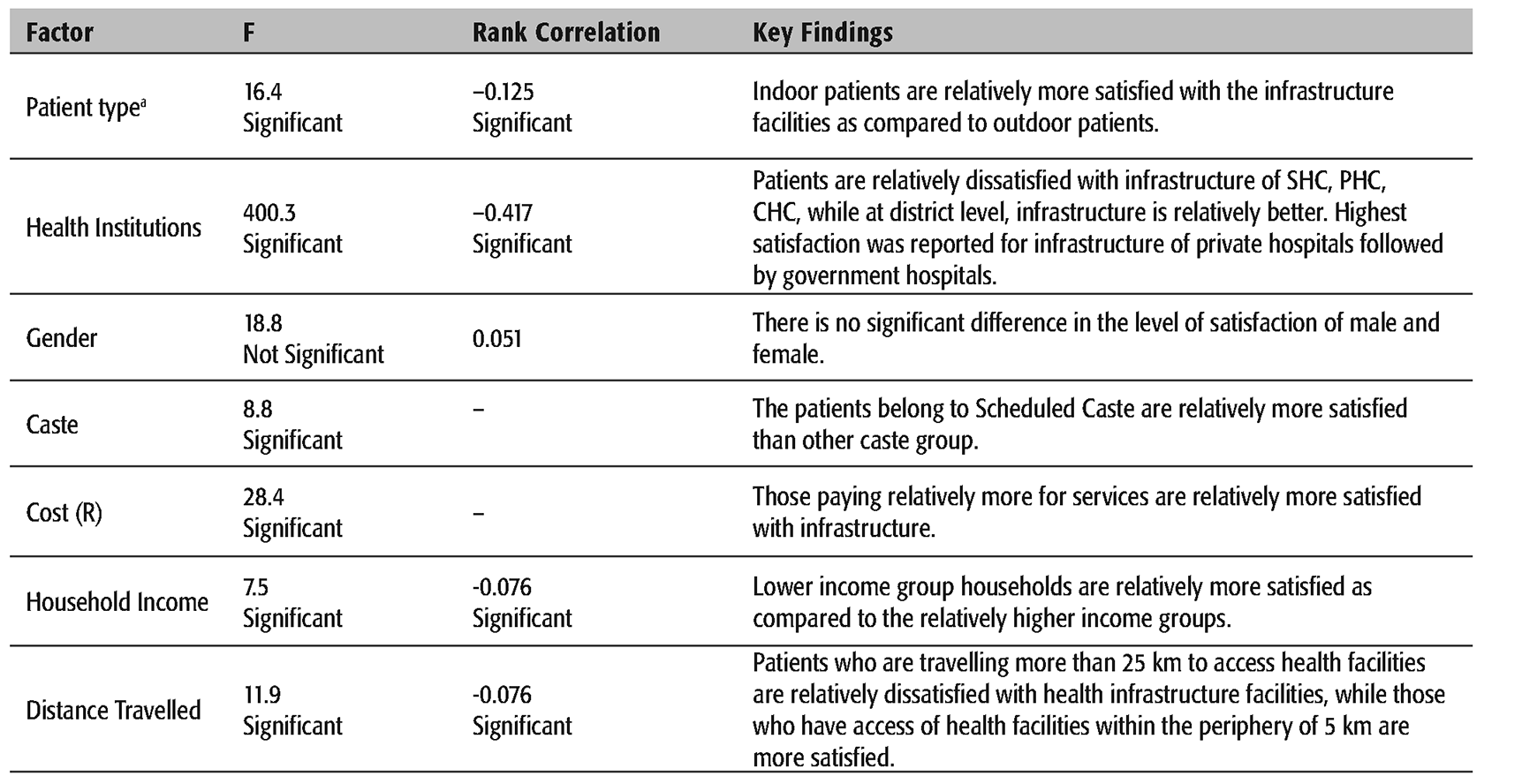
Satisfaction with Health Infrastructure
Satisfaction on Health Infrastructure Facilities of the Institutions
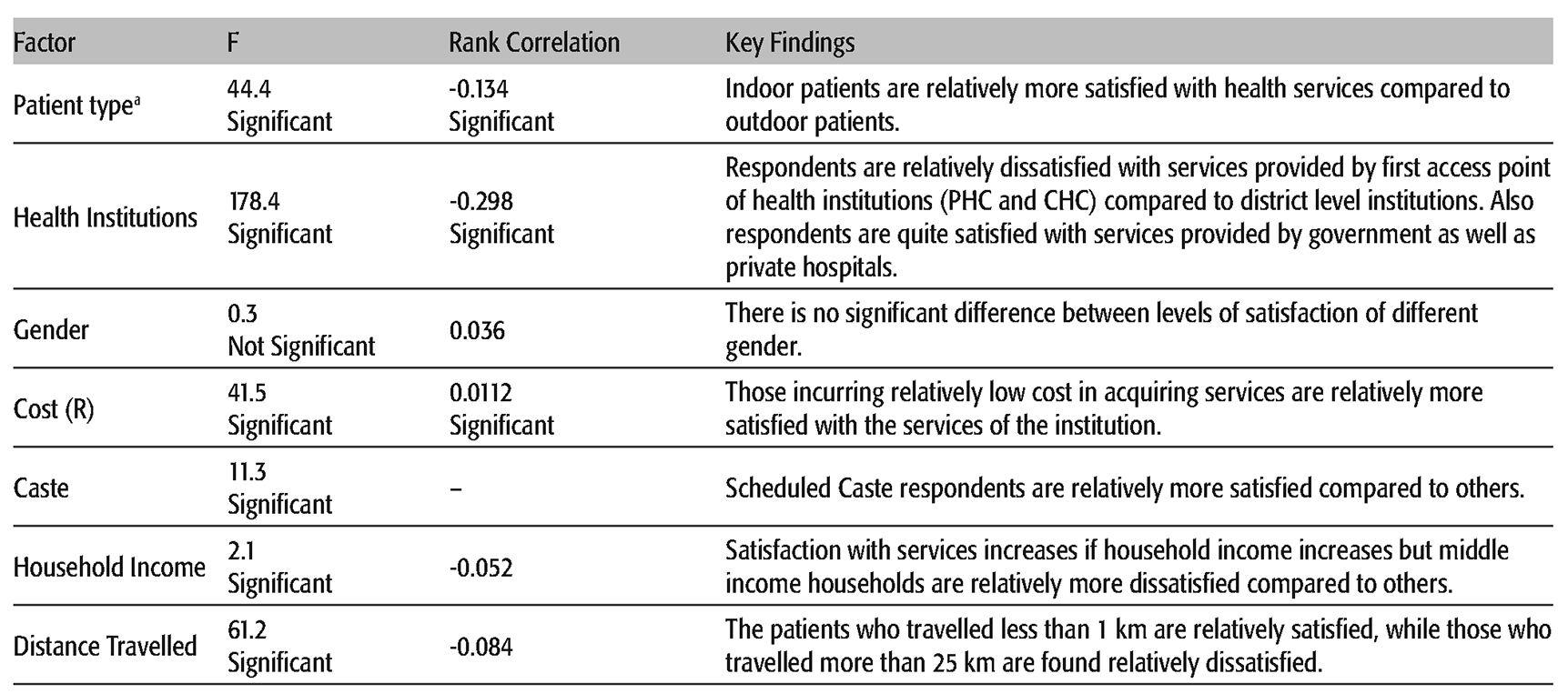
Satisfaction with Health Services
Table 7 provides evidence on association between patient satisfaction to health services of institution and their characteristic. Findings reveal that except for gender, other characteristics of respondents are significantly associated with the level of satisfaction services provided by health institutions: While the respondents are relatively dissatisfied with services provided by the first access point of health institutions, that is, PHC, SHC and CHC, they are comparatively more satisfied with the services provided by the government and private hospitals. The findings also reveal that respondents are satisfied with services provided by both government as well as private hospitals. Respondents also reported that in-patients services are more satisfactory than the services provided to out-patients. Scheduled Caste respondents are relatively less satisfied than other caste groups, while Scheduled Tribes are the least satisfied. Respondents in higher income category are relatively dissatisfied with the health services provided by institutions compared to the lower income respondents. Like behaviour of health professionals and quality of infrastructure of the health institutions, responses on satisfaction with services provided do not differ with gender or distance travelled.
Satisfaction with Healthcare Services of the Institutions
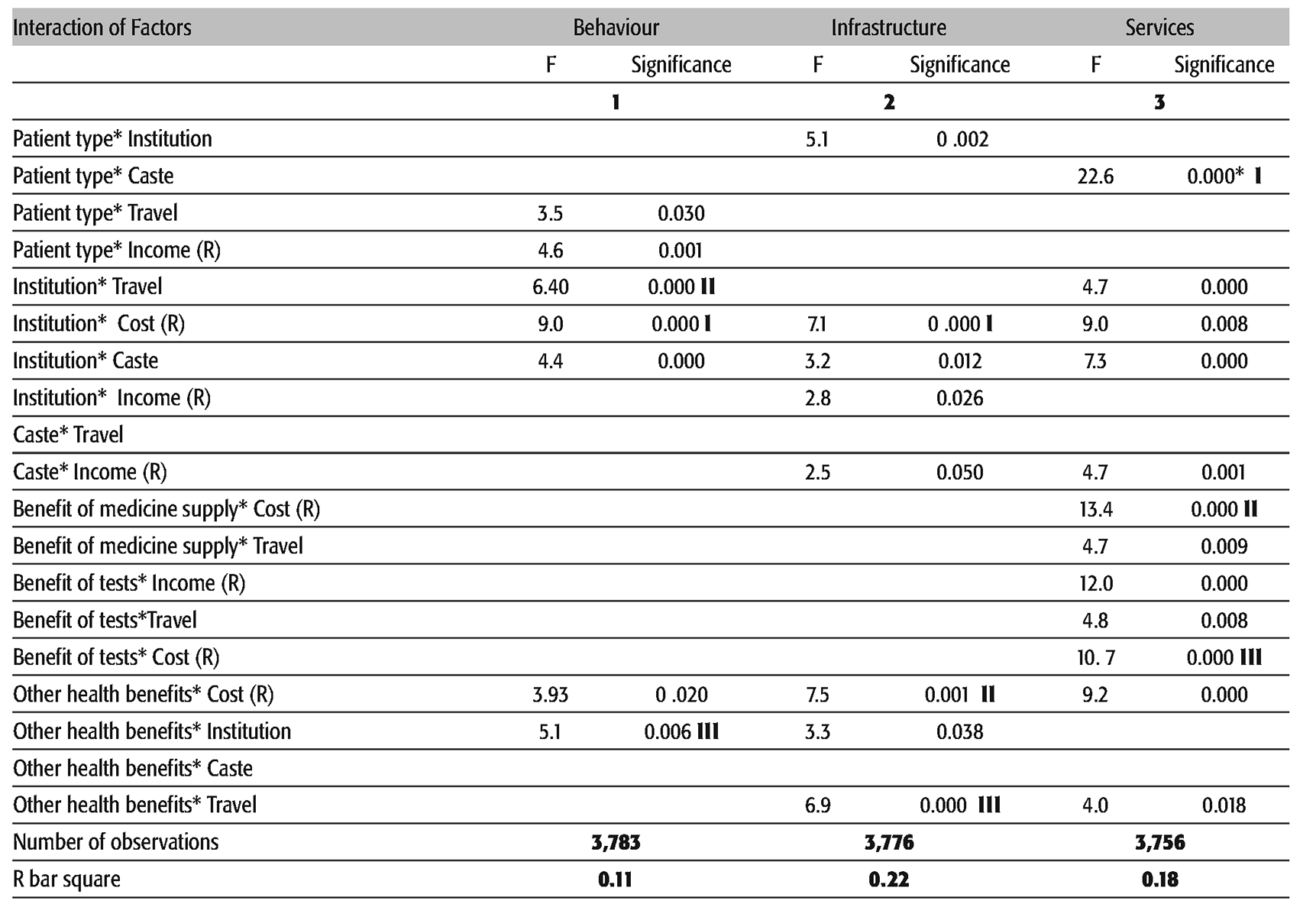
Explaining Levels of Satisfaction Using ANOVA
Results of ANOVA Explaining Variations in Level of Satisfaction
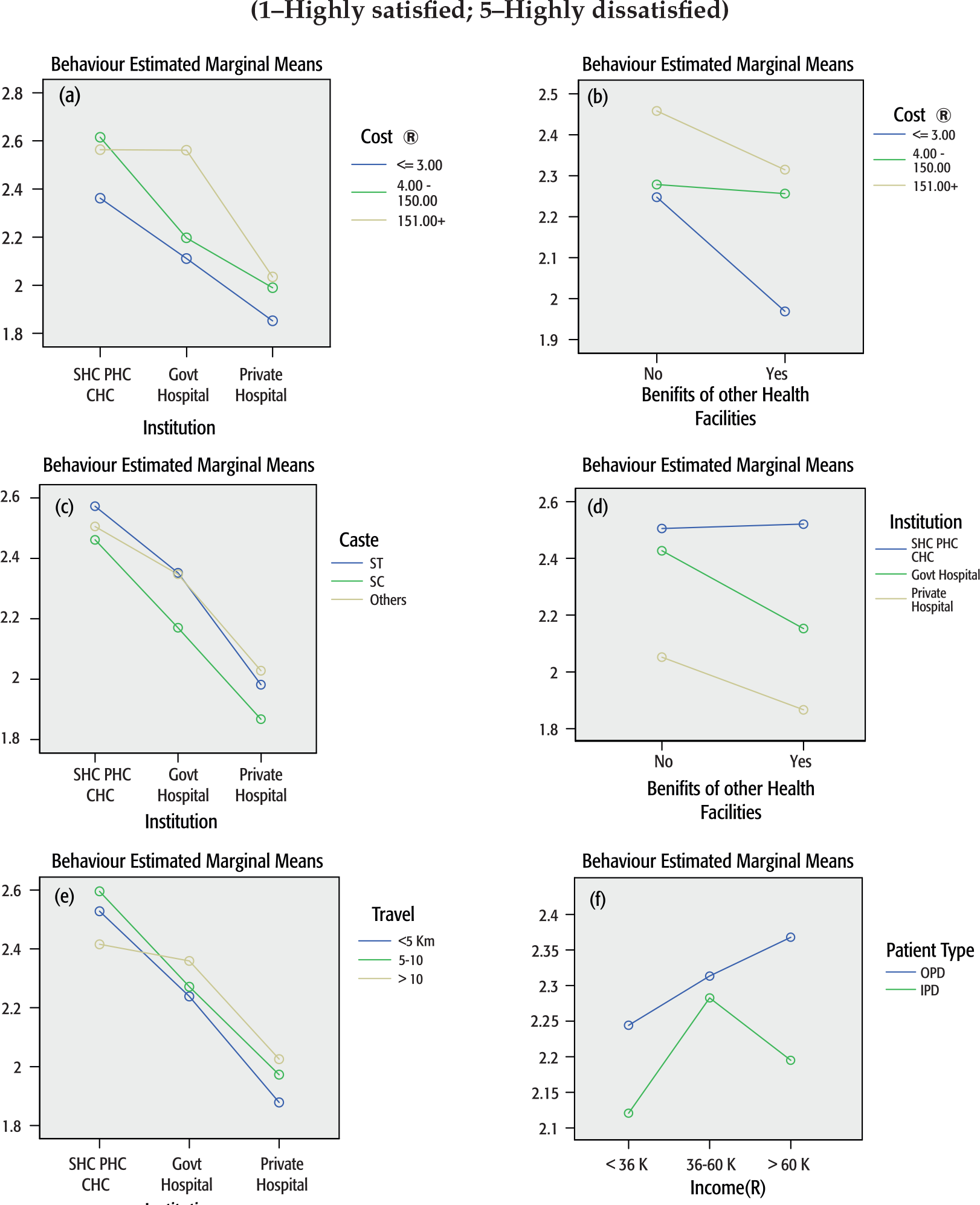
Satisfaction with Behaviour of Healthcare Professions
As only 11 per cent of the variations in satisfaction with behaviour of healthcare professionals are explained by the factors considered, it indicates that some important explanatory variables are missing from the model. Nonetheless, the findings clearly reveal that three most significant explanatory interactions are: (i) Institution and Cost; (ii) Institution and Caste; and (iii) Institution and Travel (Table 8, column 1).
What these interactions tell us is that though respondents' satisfaction levels on behaviour of the health professionals increases when one moves from SHC, PHC, CHCs to government hospitals to private hospitals, this pattern changes with cost, caste and travel (see Figure 1a through 1e, for details). For example, satisfaction with staff behaviour is affected by having incurred a high expenditure (on registration, tests, medicine, consultation and room charges) across the institutions; respondents who incur a high expense (i) do not significantly differentiate between behaviour of professionals of SHC, PHC, CHC and that of professionals of government hospitals (both are relatively dissatisfying), (ii) but do report that behaviour of health professionals of private hospitals is significantly more satisfying compared to government hospitals (Figure 1a). We find similar interaction effect of caste and travel with institutions (Figures 1c and 1e).
Source:
By and large the satisfaction with behaviour of healthcare professionals improves if the respondent has availed benefits of services provided. But this process is influenced by institutions (Figure 1d) as well as expenses incurred in availing these facilities (Figure 1b). For example, satisfaction with behaviour significantly improves when expenses are low but dissatisfaction prevails if respondent has incurred high expenses (Figure 1b). Similarly, satisfaction with behaviour of healthcare professionals significantly improves if the respondent has availed services in government or private hospitals but if the respondent has availed services in SHC, PHC or CHC, the dissatisfaction not only persists, but in fact slightly increases, if one avails benefits of services (Figure 1d). Interestingly, while the high income OPD patients are significantly more satisfied with the behaviour of health professionals, the high income IPD patients registered a decline in levels of satisfaction compared to middle income IPD patients (Figure 1f).
These findings also indicate low bias in the responses. If the satisfaction level had increased because of courtesy shown to the institutions, the interaction effect with institution, cost and travel would not have been significant.
Satisfaction with Infrastructure
Although all the interactions in the explanation in Table 8 (column 2) are highly significant, the three most important factors explaining the variations in the level of satisfaction with infrastructure of the institutions are interaction between (i) cost and institution; (ii) other health benefits and travel; and (iii) other health benefits and cost (see Figure 2a through 2e, for details). The first of the three interactions, cost and institution, reveals that though on the whole satisfaction level with the infrastructure of the institutions increases as one moves from SHC, PHC, CHC to government hospital to private hospital, the expenditure incurred on availing services does positively influence this behaviour, even in SHC, PHC and CHC (Figure 2a).
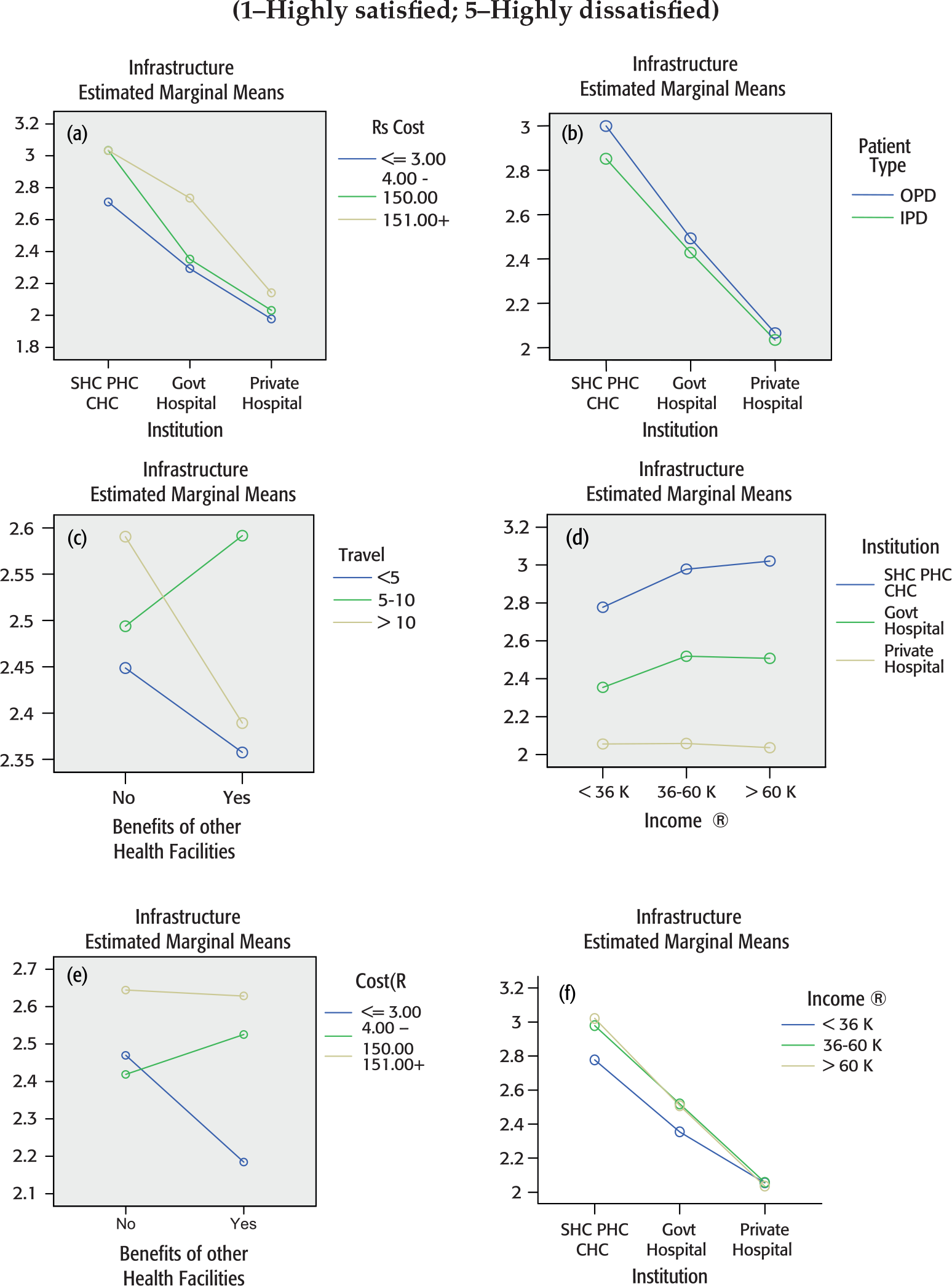
Source:
While the respondents incurring less expenses in availing services do demonstrate increasing satisfaction, those incurring high cost in availing benefits (i) do not significantly distinguish between services provided by SHCs, PHCs, CHCs and the government hospitals; and (ii) are highly satisfied with infrastructure of private hospitals. Similarly, while respondents incurring low expenses in availing services are significantly more satisfied compared to those who have not availed the benefits of health facilities, respondents incurring higher cost are, in fact, more dissatisfied with infrastructure compared to those who have not availed the benefit of services (Figure 2e). Figure 2d is revealing because the interaction between household income and institution shapes the respondents' satisfaction towards infrastructure. While at higher income levels, the satisfaction increases significantly when one move from SHPs, PHCs, CHCs to government hospital to private hospital, respondents from households with low income, though relatively dissatisfied, do not differentiate between private and government. We can interpret these results in another way: Satisfaction with infrastructure of private hospitals is very high irrespective of respondents' income. But dissatisfaction with infrastructure facilities of PHC–CHC and also government hospitals increases with income.
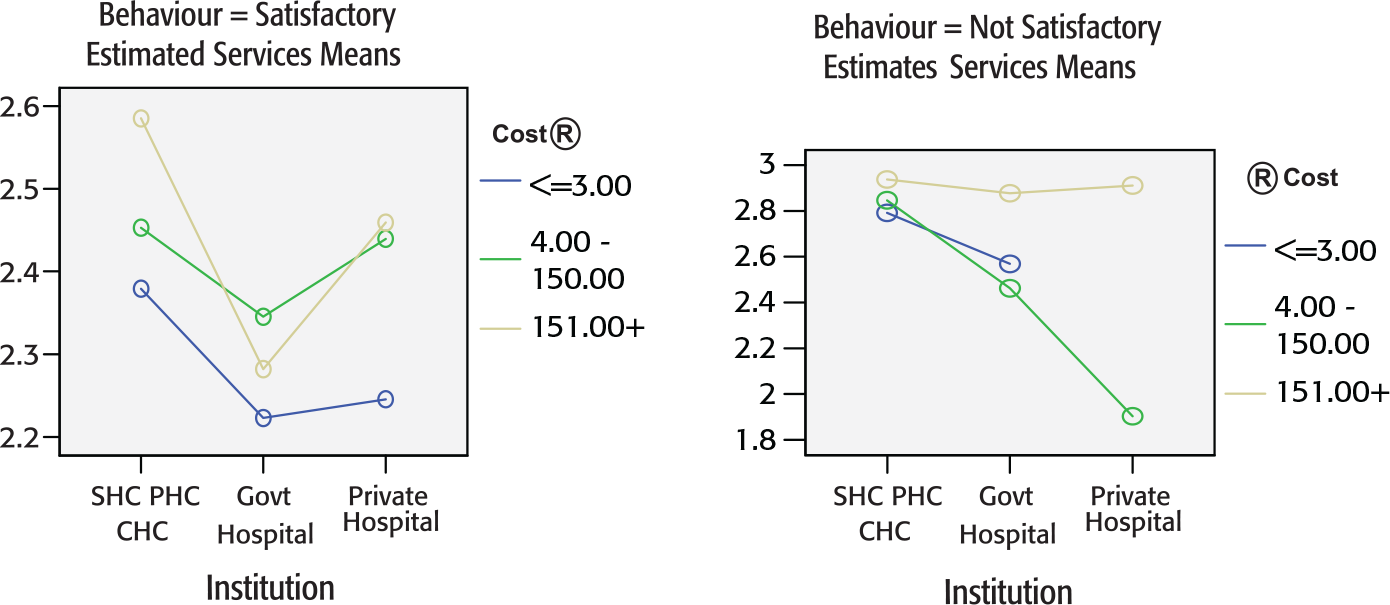
Satisfaction with Services Provided by Institutions
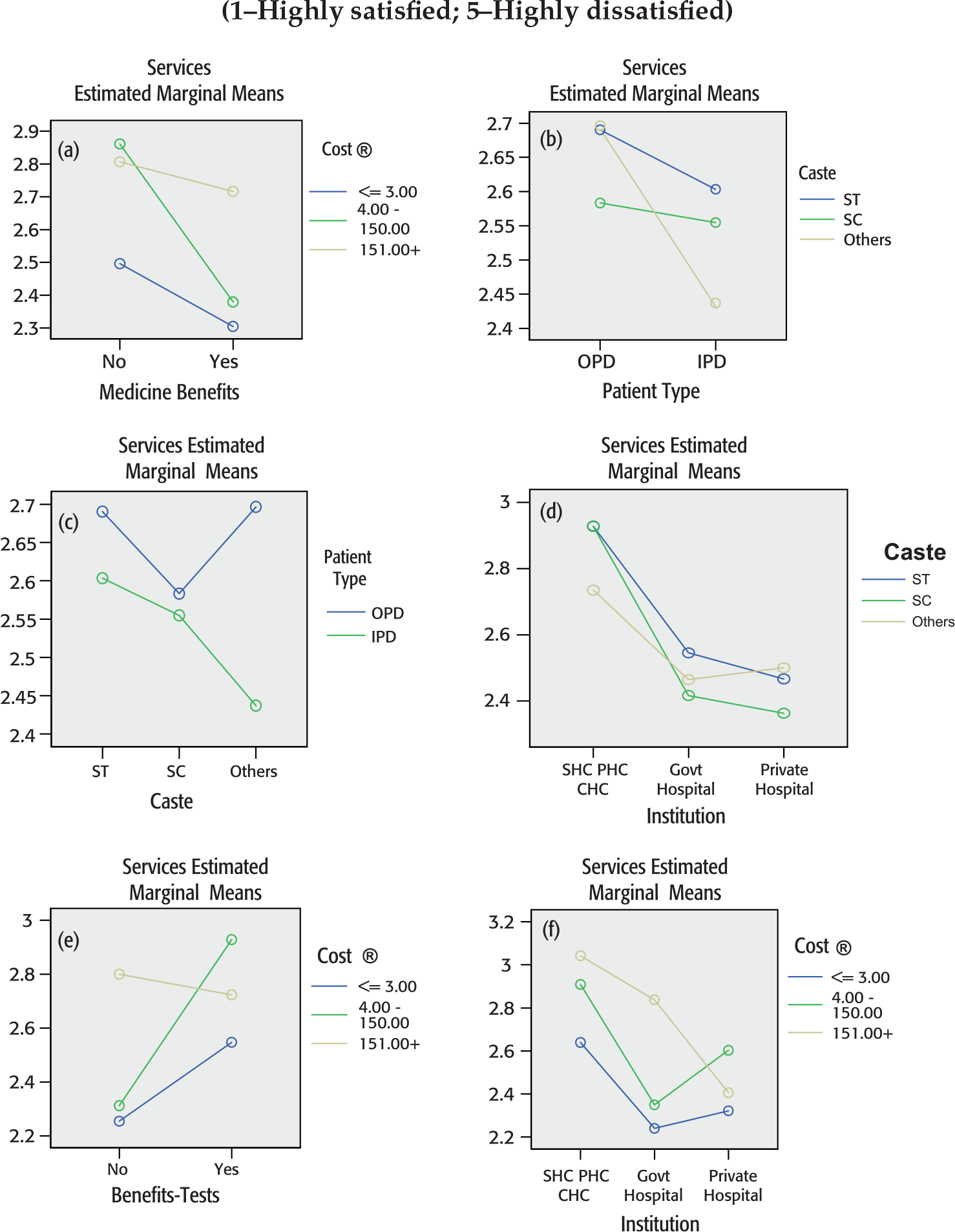
As the explanation suggests about 17 per cent variation in satisfaction with services provided, important explanatory variables must be missing from the explanation. Nevertheless, the size and interactions considered throws light on how the satisfaction levels are shaped. The three most significant interactions that explain satisfaction with services provided by institutions are (i) patient type and caste; (ii) availed benefits of medicine and cost incurred in availing services; and (iii) availed benefits of test and cost incurred in availing services (Table 8, column 3). It should be noted that services, for which satisfaction was recorded, included availability, quality and capability of doctor & ANM, ambulance, OPD timing, laboratory tests, free medicine and availability of medicines. Interpretation of the findings of Table 8 (column 3), apart from opening up the processes of forming their levels of satisfaction with services, also indicates that courtesy bias is not an important issue.
While indoor patients are in general relatively less dissatisfied with services of institutions, respondents belonging to Scheduled Tribe and Scheduled Caste categories are relatively more dissatisfied compared to others. On the other hand, with the outpatients, the dissatisfaction level is high for Scheduled Tribe and others caste respondents, while Scheduled Caste respondents are relatively less dissatisfied (Figure 3b).
Source:
Figure 3a depicts the process of shaping of satisfaction of respondents when they are availing benefits of medicine and incurring expenses for the services provided by the institutions. Dissatisfaction reduces if respondents are availing benefits of medicine compared to those not availing the benefits. Nevertheless, dissatisfaction reduces sharply only if respondents are paying relatively less for the services. If they are incurring high cost for services, they are still as dissatisfied as those not receiving benefits of medicine supply. This is a clear indication that courtesy bias is low.
The evidence showing low courtesy bias is also reflected in Figure 3e, which depicts how interaction between costs incurred in availing services and availing benefit of test is shaping the respondents' satisfaction levels with services of the institution. All respondents who have availed benefit of test are dissatisfied irrespective of expenses incurred. But if a respondent has incurred higher expenses in availing services, he is dissatisfied irrespective of whether he has availed benefits of test or not. But respondents incurring low expenses are relatively dissatisfied if they avail test rather than if they do not avail test. Had there been courtesy bias, respondents availing benefit of test would have recorded satisfaction.
Findings of the analysis by and large reveal satisfaction with the behaviour of health personnel but dissatisfaction with the services as well as infrastructure of healthcare institutions. It means that expectations of consumers are positively shaped if the health providers attend to the patient. This is understandable in the case of sub-district institutions where timings of doctors are highly irregular and the patient is satisfied if he is able to meet the doctor even after a few hours' wait. It is therefore important to understand how the perceptions are interrelated to each other. As an example, we analyse the effect of introducing satisfaction with (i) infrastructure and (ii) behaviour of health personnel in explaining the levels of satisfaction with services.
Role of Perceptions on Behaviour and Infrastructure in Shaping Perceptions on Services
Three-Way Interaction in Explaining Perception on Services
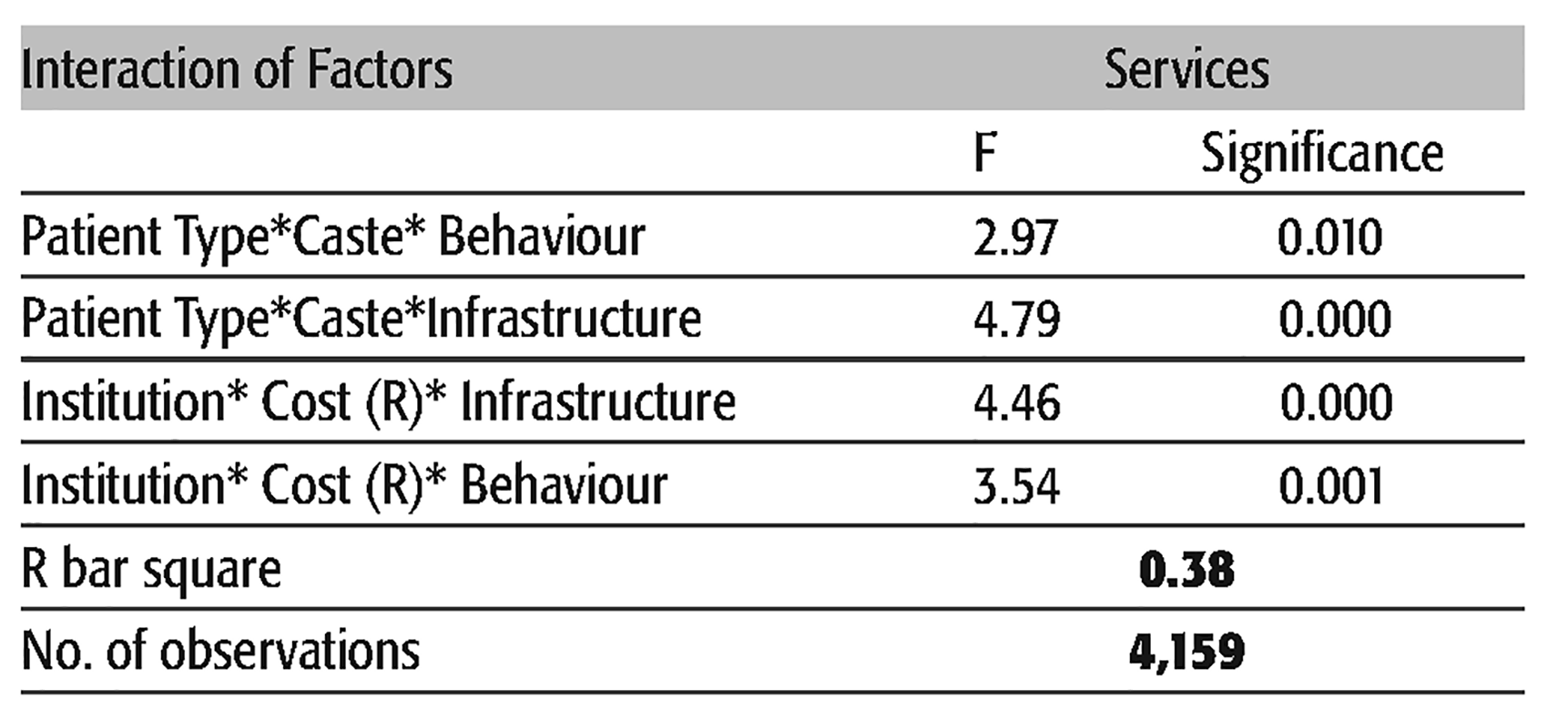
Inclusion of perceptions of consumer in the explanation improves the R bar square substantially to about 38 per cent. This means that a substantial part of variations in satisfaction with services are explained by interactions among (i) patient type and caste; and (ii) cost incurred in accessing services and institutions along and perception on (a) behaviour of health personnel, and (b) infrastructure. What these three-way interactions tell is that:
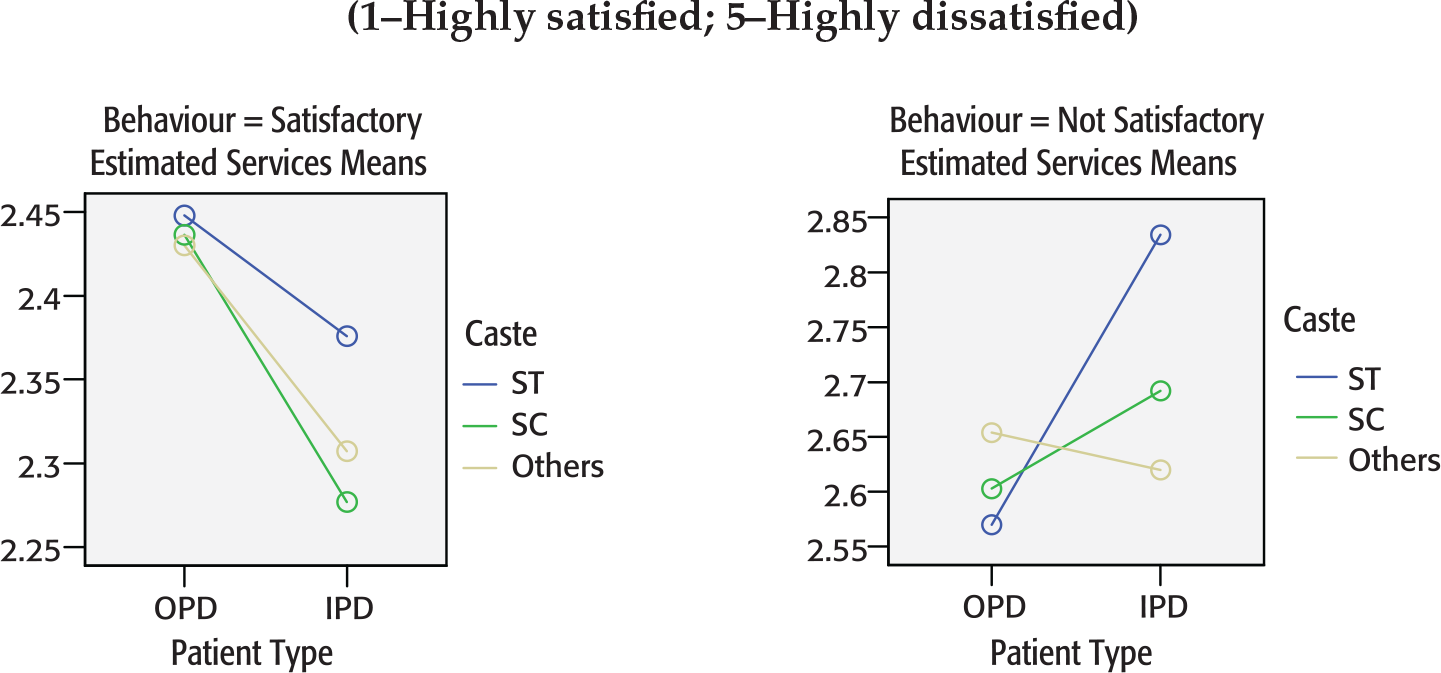
Irrespective of caste of consumer, if the behaviour of healthcare personnel is satisfactory, the consumer is highly satisfied if he is an in-patient rather than an out-patient. But if the consumer is not satisfied with the behaviour of health personnel, dissatisfaction towards services provided significantly increases for indoor patients compared to outdoor patients (Figure 4a).
Irrespective of the cost incurred in availing services from an institution, consumers' satisfaction on services received significantly improves in district hospitals compared to institutions at the sub-district level if they are satisfied with the behaviour of the personnel. But if a consumer is not satisfied with the behaviour of health personnel, his dissatisfaction increases if he has incurred high cost in accessing the services, irrespective of the type of institution he is in (sub-district, government hospitals or private hospitals).
Interaction among Patient Type, Cost and Behaviour
Interaction among Institution, Cost and Behaviour
These findings do indicate that perceptions on services provided are also shaped by, apart from other factors, perceptions about behaviour as well as infrastructure.
The Way Ahead
Summing Up
The analysis of the exit survey data from Madhya Pradesh suggests that client satisfaction responses in user exit surveys are not positively biased and are substantially critical. The criticality of responses is reflected significantly in the case of satisfaction on infrastructure and also on services provided by the healthcare institutions; evidences show that there is no positive bias for satisfaction on infrastructure as well as quality of services provided. However, the questions that seem to be answered with the least bias in the exit survey are those that are the least useful. If consumer perceptions in exit surveys closely reflect observable infrastructural facilities, questions on these perceptions would not add to what could be learned from direct observation using facility surveys.
What distinctively emerge from this exit survey are the subjective but positive perceptions on the behaviour of practitioners and the respondents' overall dissatisfaction with service quality. The perception is that public healthcare institutions at the sub-district level have poor infrastructure and poor service delivery and their health personnel display a dissatisfactory behaviour towards patients compared to the district level institutions, both public and private. This obviously calls for changing the functioning of SHC, PHC and CHCs both in terms of staff capabilities as well as service delivery. These aspects aside, the exit survey data are informative. Cost incurred to access services from the institution has a significant negative impact on the perceived value of the service. Another finding is that the characteristics of the patient seem to matter a great deal for reported satisfaction. They are able to differentiate satisfied from less satisfied healthcare consumers and shed light on the service quality that increase user satisfaction. It is highly disturbing that class, caste and income of the consumers should influence their perceptions about services of health institutions.
Importantly, ANOVA results conclusively show that responses are affected by interactions of factors rather than by individual factors. This analysis highlights three important interactions:
By and large the satisfaction with behaviour of health professionals improves if the respondents have availed benefits of services provided. But this process is influenced by institutions as well as expenses incurred in availing these facilities. For example, satisfaction with behaviour significantly improves when expenses are low but dissatisfaction prevails if the respondents have incurred high expenses. Similarly, satisfaction with behaviour of health professionals significantly improves if respondents have availed services in government or private hospitals but dissatisfaction persists, and in fact, slightly increases if the respondents have availed services in sub-district institutions (SHC, PHC or CHCs). The interaction between household income and institution shapes the respondents' satisfaction towards infrastructure. Satisfaction with infrastructure of private hospitals is very high irrespective of respondents' income. But dissatisfaction with infrastructure facilities of sub-district institutions (SHC, PHC, CHCs) and also government hospitals increases at relatively higher income. Dissatisfaction with the services reduces if the respondents have availed the benefits of medicine compared to those not availing the benefits. Nevertheless, dissatisfaction reduces sharply only if respondents are paying relatively less cost for the services. If they are incurring high cost for services, they are still as dissatisfied as those not receiving the benefits of medicine supply.
Three-way interactions also prove that perceptions on services provided are shaped by, apart from other factors, perceptions about behaviour as well as infrastructure.
Lastly, data in the exit surveys may also include (i) availability of essential drugs and their supply, (ii) quality of tests and the (iii) process of examining the patients. This is because the perceptions about services and behaviour of health personnel are also shaped by the following factors: Were the essential medicines made available on time? Who examined the patients? Was a physical examination done? Were the causes of ailment, general health and nutrition and instructions on medications discussed with patients? Did the diagnosis and healthcare lead to cure? These are objective assessments made by patients and may on the one hand become policy questions and may lead to objectivity in investigation, on the other.
Using the Findings of Client Exit Survey
The findings of this study may be used in two different ways. First, they could be used for joint action at the district and sub-district levels for identifying ways to strengthen the healthcare institutions. Second, they may be used as evidences for legal actions.
Accessibility of health services and its quality are key concerns in remote rural areas, especially for the poor and marginalized section of society. Owing to poor infrastructure, indifferent behaviour of health personnel, and poor quality of services in public institutions, even clients from poor income group are approaching the private institutions. Lack of medicine, erratic supply of electricity, non-availability of doctor, shortage of skilled health personnel, general apathy towards the poor, indifferent attitude of the health staff, poor maintenance of critical equipment are some of the factors that have deterred the patients, from all caste and income groups, from accessing the public health services both in urban and rural setting. The present standard of health services do not match the norms and hence when it comes to the question of quality service, people increasingly depend on the private healthcare providers.
As proponents of quantitative research, we are treating these responses not as given but shaped by the failure of the health institutions to service the needy. The findings of this research could be seen as the centre of deep subjectification at one level and voices of disapproval, on the other. The interaction of community with health institution, while seeking healthcare, takes shape not as a conflict between the providers and the sick; it stems from the question of governance. This interaction has less to do with the structure of the institution; it is more about the way in which the conduct of sick, as individuals, are predetermined. In doing so, institutions not only cover the legitimately constituted forms of subjection but also modes of actions—considered and calculated—which were intended to shape possible field of actions of the sick. In other words, to govern is to construct the possible field of actions of the sick. These disciplinary techniques, for controlling and internalizing the behaviour, also lead to self-discipline in the production of the individual as a subject (Gorden, 1980). This is not so much to exert power, but to ensure that the disciplinary mechanism is in place. Sovereignty and disciplinary mechanism are two absolutely integral constituents of the general mechanism of power (Gorden, 1980). Inevitably, this also represents asymmetrical power relations between healthcare providers and healthcare seekers.
Following Foucault (1980: 95–108), it can be argued that the privileged place to observe the power in action is the relations between the institution and the individuals (Balan, 2010)—How institutions exert their power on individuals and how the latter affirm their own identity and resistance to the effects of power because power is coextensive with resistance, producing positive effects. Consequently, despite strictly adhering to norms set by health institution in course of their interactions with institutions, the consumers also resist the way they are treated. Healthcare services become political for they represent the way we are governed. No matter how shabbily recorded, the findings of the client exit survey may be seen as consumers' protest to services provided by public health providers. These responses provide opportunity to understand the characteristics of liberalism and the mentality of administration that serve a society, existing external to the health institutions.
Client Exit Survey as a Tool of Advocacy
The following findings of institutional and exit survey were shared with the District Collector, Chief Health Officers and CEO, District Panchayat of all the 12 districts:
Consumers of sub-district health facilities are highly dissatisfied with infrastructure, behaviour of health personnel and services provided by the institutions. Infrastructure at PHCs is substantially below the standards prescribed by the health authorities, especially with respect to out-patients facilities, availability of health providers, availability of essential medicines, efficient and effective healthcare supply and electricity supply. There is discrimination in access to services on the basis of class and caste of patients.
These findings were also shared with media and Chairperson of District Planning Committees in these districts. Discussions on these findings were held with patients and health administration at the district and sub-district levels. Using participatory research appraisal method, a rapid study on Rogi Kalyan Samiti was conducted to understand the decision-making process relating to (i) public–private partnership at the institutional level and (ii) community participation in management health institutions. These findings were also shared with the District Collector and the Health administration of all the districts.
The Chief Medical Officers of Panna, Sehore, Jabalpur and Jhabua agreed that consumers have increasingly becoming dissatisfied with the services provided in government hospitals and prefer private healthcare services. But majorities of the people who access the government medical services come from poor and marginalized sections of the society who cannot afford the costly medical and health services of the private hospitals. There are, however, limitations that institutional health service providers face while discharging their duties. Shortage of skilled staffs and administrative engagements of the health service providers are two serious difficulties faced by the public health system. Health Officers also believe that as quality is a subjective issue—that varies across locations and is influenced by multiple factors like quality of human resource, remuneration, basic infrastructure, instruments, sanitation, water and electricity supply, supply of medicines and also affordability of the services by the consumers—it is difficult to assess comparative efficiency of health services in two different settings that is, rural and urban. It is also important to note that the government has put in place the parameters of standard health services of its institutions but in most of the cases the people from poor rural areas do not have any idea as to what these standards are and how significantly they are related to the quality of services being delivered to consumers. Therefore, the response of the people on any health survey administered, particularly in remote rural, semi-urban or backward areas, is to be first understood in terms of the prevalent standard of health services in the area, and the socio-economic and educational condition of the people being catered by these health institutions.
The health administrators of these districts, nevertheless, believe that such exit surveys can become a tool for judging the quality of healthcare services, provided objective questions like the time of opening of the healthcare centres, arrival time of healthcare providers, number of patients served by them, medicines provided to consumers and the extent of private practice by healthcare providers are part of the questionnaire. Equally important is monitoring of the effect of these findings on improvement in quality of services.
Using the Findings in Public Interest Litigation
Many of the findings from the study, especially related to services provided by the healthcare institutions—like availability, quality and capability of health provider, ambulance, OPD timing, laboratory tests, free medicine and availability of medicines—can be used as evidences on Public Interest Litigations. Independent of this Exit Survey, an activist and lawyer, Mr Sandesh Bansal, filed a Public Interest Litigation, in Jabalpur High Court in 2008 against the erratic electricity supply in public healthcare institution in Madhya Pradesh. Based on the judgement of this PIL, the Health Administrators in Madhya Pradesh ordered that in case of erratic power supply, all the public health institutions shall purchase and use diesel generator sets. Similar to the above PIL filed, data on quality of services provided by health institutions may be used in making a case against the poor health services. But the risk associated with subjectivity of such data cannot be over-emphasized.
Implications for Health MIS
Information from healthcare consumers about the causes of their dissatisfaction with public health providers can become an important tool for monitoring quality of services, provided the method of data collection addresses the issues of validity of responses. Such Exit Surveys can help in protecting interests of the consumers only if their feedback affects the decisions of the health administration (Crow et al., 2002). District health plan may include findings of exit survey conducted, on a regular basis, either by an independent agency or by the local health department. Results of these surveys may be used as performance indicators at the state or national level in identifying consumers' perceptions and concerns, areas of service failure, and scope for improvement.