
Abstract
The hidden curriculum profoundly shapes professional identity formation in postgraduate psychiatry training through implicit norms, institutional culture, and role modeling. Beyond formal curricula, it influences ethics, communication, well-being, and professionalism. Recognizing and positively shaping hidden curriculum can enhance trainee development, institutional culture, and humane, patient-centered psychiatric practice.
The concept of the hidden curriculum was first introduced by Philip Jackson in 1968 in the context of school education, referring to the implicit lessons, values, and norms transmitted outside the formal curriculum. 1 This idea was later applied to medical education in a seminal article by Hafferty in 1998, who argued that, beyond formal curricular reform, the organizational culture, policies, evaluation systems, and everyday practices of medical institutions powerfully shape professional identity formation in trainees. 2 Subsequent researchers expanded this understanding by demonstrating how the hidden curriculum influences professionalism, ethical conduct, communication styles, attitudes toward patients, and trainee well-being across undergraduate and postgraduate medical training.
During the postgraduate trainee program, a doctor usually develops skills in specialized medical procedures, patient care, and laboratory work as applicable. A postgraduate training program is usually considered more intensive and difficult than undergraduate medical courses. During the postgraduate training program, trainees need to work long hours as they put their academic, research, and clinical work into practice while providing patient care.3–5 In a less resource-intensive health sector such as India, postgraduate residents play a crucial role in the medical field and are frequently expected to instruct undergraduate or junior students. This dual role of postgraduate residents as both learners and teachers in the Indian context creates a unique hidden curriculum. Residents, while still in the process of professional and emotional development, may replicate instructional styles they have themselves been exposed to, such as fear-based learning, public reprimanding, or hierarchical communication, often without deliberate intent. This transmission occurs informally through observation and practice, reinforcing a cycle in which such behaviors become normalized within clinical training environments. It’s critical to strike a balance between their instruction, academic activities, learning, and health care delivery.6,7 As per competency-based curriculum guidelines, it formally expects residents to acquire teaching skills and actively participate in training undergraduate students, thereby positioning them simultaneously as learners and educators. Also, the strong emphasis on documentation, logbooks, and continuous formative assessment may implicitly prioritize measurable outputs and procedural compliance within training. Furthermore, the expectation of functioning within multidisciplinary teams while maintaining professionalism and accountability may shape implicit norms around hierarchy, communication, and role expectations in clinical settings. 8 The residency program’s teaching and learning process is highly dynamic. It entails intricate interactions among several variables, including clinical workload, faculty supervision and role modeling, institutional culture, peer interactions, administrative respon-sibilities, and individual trainee characteristics. 9 As mentioned above, teaching faculty and postgraduate trainees often focus on the implicit curriculum because it is much better defined and is objective.
Despite its pervasive influence, the hidden curriculum in postgraduate psychiatry training remains under-recognized and insufficiently examined in structured discussions. Acknowledging its presence is essential for fostering reflective practice, strengthening professionalism, and promoting supportive institutional cultures.
This article explores the dimensions, impact, and strategies to monitor and promote a positive hidden curriculum in postgraduate psychiatry training programs.
Discussion
The postgraduate psychiatry trainee comprises a physician’s formal training. Throughout the postgraduate training program, a postgraduate trainee develops the clinical abilities necessary for senior residency or independent private practice, as well as the ethical maturity necessary to function as a qualified psychiatrist. This process is known as professional identity formation. 10 The curriculum significantly influences trainees’ educational outcomes and experiences. 11 Curriculum in academic programs has been defined by various criteria. Broadly, it can be categorized into explicit and hidden curricula. Eisner highlighted the distinction between the hidden and explicit curriculum. 12 The explicit curriculum can be understood as “the planned and expected educational or training outcomes and experiences of learners, but there are inevitable factors that influence their experiences, attitudes, values, behaviors, and transfer of ideas.” 13 The term “hidden curriculum” refers to those experiences that are not specifically listed in the predetermined curriculum. 13 Hidden curriculum is considered to be more subtle, pervasive, and influential than the explicit curriculum in shaping a psychiatry postgraduate training attitude and behavior. 14
Teaching faculty who train postgraduate medical personnel should consider how to develop and strengthen values, attitudes, ethical standards, social skills, and other traits that influence a clinician’s human behavior, in addition to knowledge and skills. The role of psychotherapy training, which is relatively unique to psychiatry residency, also provides an important avenue to reinforce Attitude, Ethics, and Communication (AETCOM) competencies. Through supervised psychotherapeutic work, trainees develop skills in empathy, reflective listening, and patient-centered communication, thereby aligning formal curricular objectives with the hidden curriculum. 15 Also, through unit and divisional routines, traditions, rituals, and daily interactions in clinical practice and learning on their respective units, postgraduate trainees acquire implicit messages about what is essential to their education and careers. Teachers and trainees should be aware that there is always some kind of hidden curriculum (a curriculum that can be acknowledged but not explicitly codified) present, whether in the classroom, the administrative office, or the clinic area. Because trainees learn more from imitated actions throughout their postgraduate training than from formal education, it is imperative to recognize the existence of a hidden curriculum. 16 Paying explicit attention to hidden curriculum can help faculty reflect upon what all, apart from the codified curriculum, is of value and necessity for the residents in the formative years of their careers. This may also enable them to make ancillary efforts to develop residents’ skills.
Components of Hidden Curriculum
Hafferty has outlined four areas in which institutions might identify the effects of the hidden curriculum: Policy development, evaluation, resource allocation, and institutional slang. 1
Policy Development
It alludes to the unspoken “rules of the road.” For example, some medical institutions have an unspoken moral and ethical rule that forbids postgraduate students from meeting with pharmaceutical firms’ medical representatives or accepting any kind of payment or non-payment.
Evaluation
In a few medical institutions, trainees are evaluated and emphasized on certain aspects, such as their behavior, the way they deal with patients, empathy and sympathy toward patients, dedication to their patients, and participation in activities beyond academic work, which can affect trainees at different stages of their careers.
Resource Allocation
Depending on what the organization values and wants to foster and encourage, resources are allocated and dispersed to those organizations. For example, postgraduate trainees face many demands, ranging from clinical responsibilities, research activities, attendance at scientific meetings, continuing medical education programs, and administrative activities, to maintaining competence in clinical practice, which requires dedicated time and funds. Each medical institute assigns varying degrees of importance and significance to the above-mentioned factors. However, instead of supporting what the trainees value, these institutions use or focus their resources solely on what the institute values most, such as funding high-tech diagnostic tools over patient counseling spaces. 17
Institutional Slang
It describes the words or phrases used within an organization that subtly convey its ideals. For example, in psychiatry training, the use of terms such as “difficult” or “non-compliant” and labeling patients based on diagnoses may contradict AETCOM 15 principles of empathy, respect, and patient-centered care, thereby reinforcing stigma and shaping the hidden curriculum through everyday communication practices.
In addition to Hafferty’s foundational framework, later researchers have expanded the understanding of hidden curriculum to include peer culture, emotional socialization, communication norms, and the impact of implicit bias, each contributing to the development of professionalism and well-being in trainees.18,19
To explore, identify, and map the key ideas about hidden curriculum and its dimensions, domains, effects, and variables in medical residency courses, a scoping study was conducted using the primary sources and supporting data. According to the electronic databases, the content analysis revealed seven themes: Communicational factors, educational issues, organizational issues, socio-cultural issues, professional issues, resident educational characteristics, and resident personal characteristics. 9 The most crucial of these appears to be role modeling.
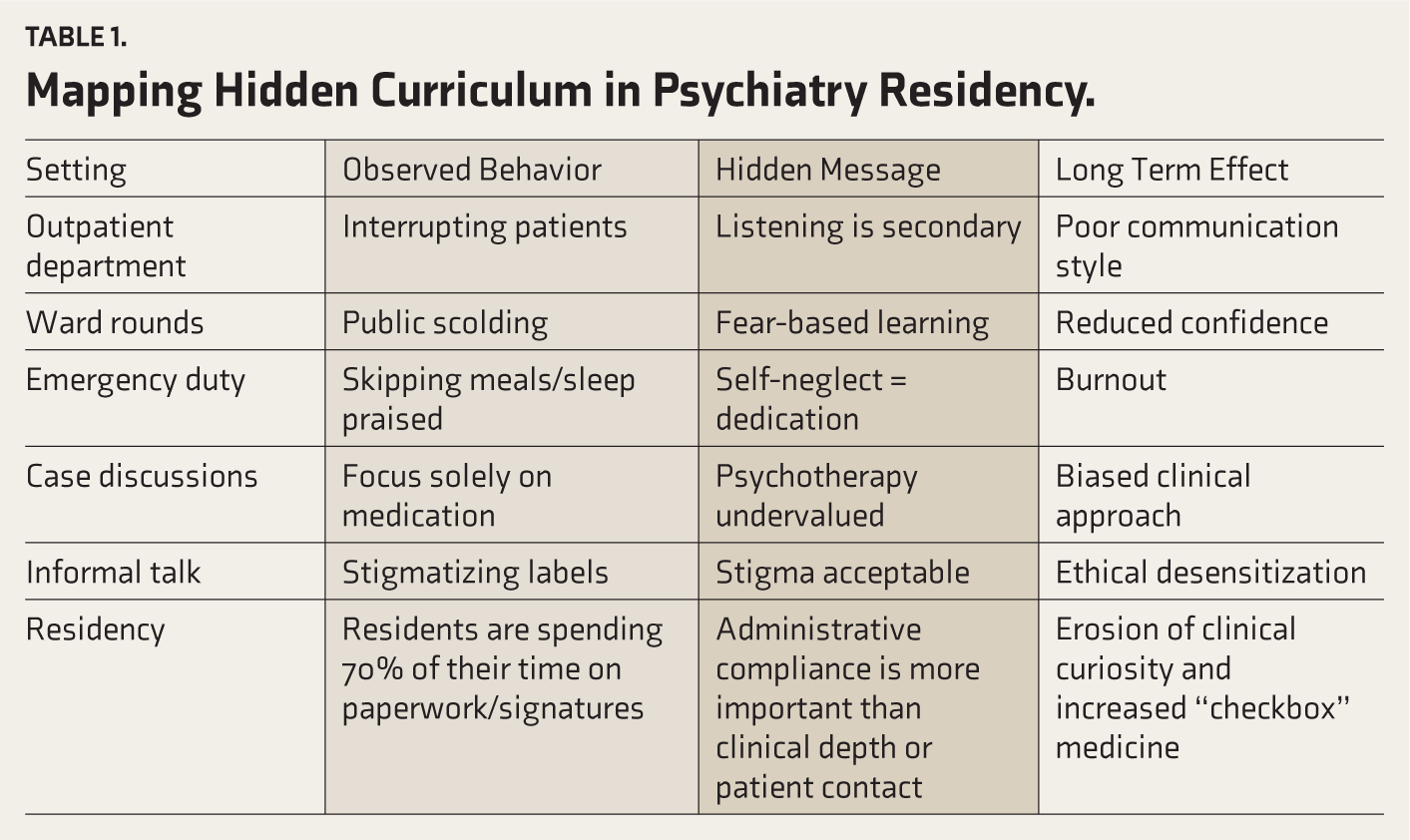
Table 1 shows how the hidden curriculum affects the long term.
Mapping Hidden Curriculum in Psychiatry Residency.
Anticipated Benefits of Acknowledging and Addressing the Hidden Curriculum
The hidden curriculum has the ability to significantly impact trainees’ and teaching faculty members’ present and future clinical and professional performance in the clinical setting since it communicates the crucial ethical culture, norms, and guidelines on acceptable emotions and behavior. 9
When acknowledged and positively shaped, the hidden curriculum can: Promote compassionate professionalism and ethical reasoning, enhance reflective practice and self-awareness, build supportive peer networks and reduce burnout, improve clinical communication and patient-centered care, strengthen teamwork, and respect across disciplines, foster leadership and health advocacy skills, and align learners with humane institutional values.20–22 Due to these potential benefits, we ought to recognize the hidden curriculum in psychiatric residency training and understand how it shapes future specialists in psychiatry.
Monitoring and Promoting a Positive Hidden Curriculum in Postgraduate Training Programs
It is recommended that all postgraduate training programs have a formal obligation to pay attention to and monitor the hidden curriculum as a marker of quality.
The following is the procedure to take care of a positive hidden curriculum:
Develop a reporting system for trainees: Creating a system that allows students to report behaviors that hinder their ability to meet formal learning objectives. Create safe forums for dialogue: Establishing safe spaces that respect the privacy of teachers and students to talk about and remedy hidden curricular impacts. Include hidden curriculum indicators in program evaluation: Integrate structured questions assessing professionalism, communication climate, teamwork culture, and observed role modeling into routine course and faculty evaluations.
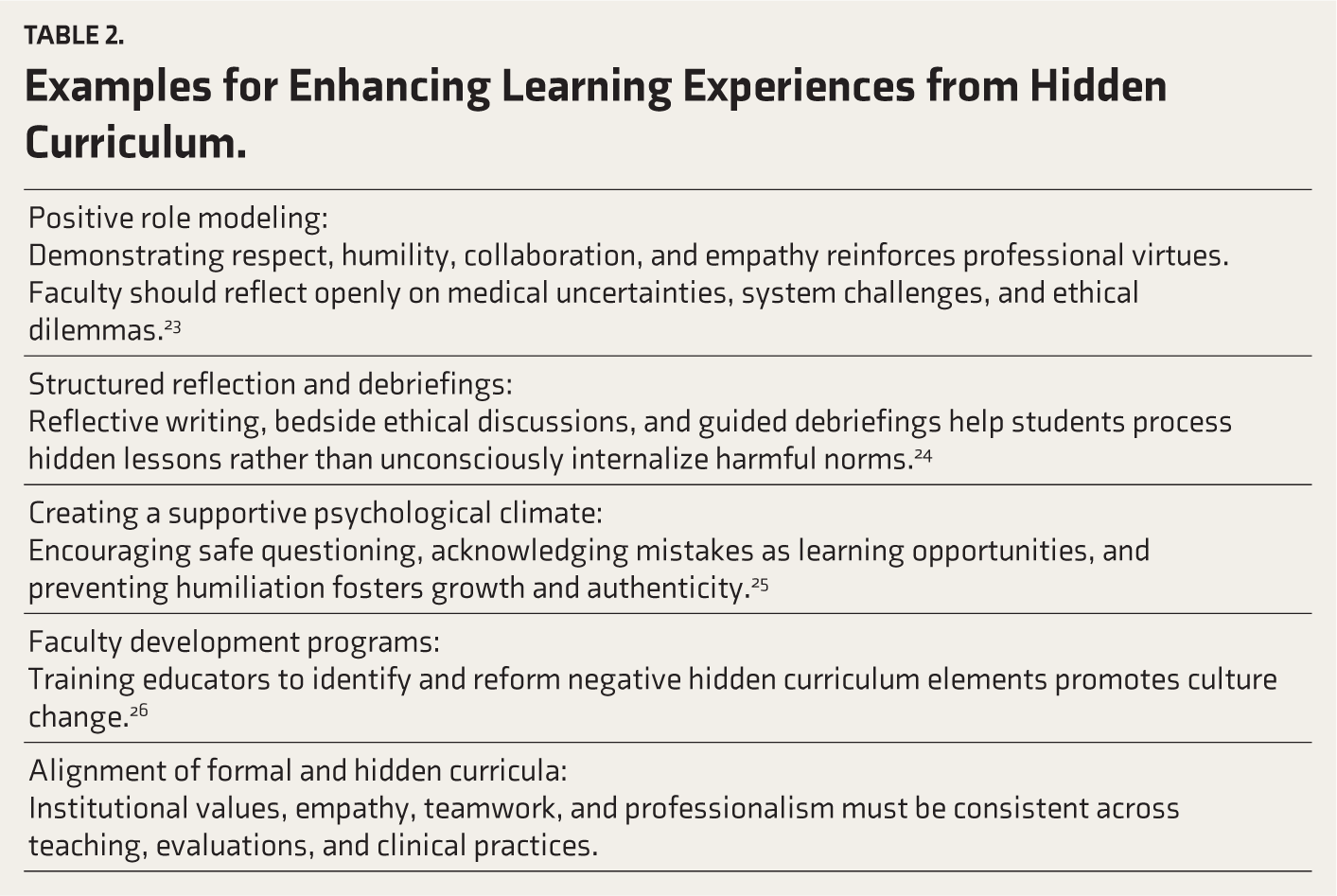
Examples of practices that enhance the hidden curriculum are presented in Table 2.
Examples for Enhancing Learning Experiences from Hidden Curriculum.
The American College of Physicians recommends group reflective practice to improve trainee well-being and better connect the explicit and hidden curricula. 26 A few Indian institutions have instituted group reflective practices for their trainees, such as senior residents taking classes on psychopathology, role modeling for interviews, or eliciting psychopathology, supervising the junior resident while taking consultation liaison rounds, from issues related to being on call with senior colleagues to dealing with emotionally challenging patient or patients with acute crisis such as suicidal attempt and acute florid psychosis encounters. As per existing literature, this practice of group reflection shows that the organization values its trainees and can improve professionalism, compassion, and patient care. 27
Conclusion
The hidden curriculum exists across institutions and knowingly or unknowingly shapes the professional development and career trajectories of psychiatry trainee residents. Despite being an implicit endorsement of an institution’s beliefs, it may have a significant impact on postgraduate students’ learning endeavors and career opportunities. It also develops time management skills, interpersonal communication skills, problem-solving capabilities, and the resilience demanded of medical professionals. The initial step in recognizing the hidden curriculum may be group reflection or mentor-supervised training, which might eventually lead to the creation of plans to support trainees’ welfare across institutions. By strengthening role modeling, enhancing reflective opportunities, and promoting supportive institutional cultures, faculty can transform hidden curriculum into a positive driver of medical professionalism and humane patient care.
Footnotes
Acknowledgements
None.
Appropriate Permissions from the Concerned Authorities
Has been taken.
Data Sharing Statements
NA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the views or policies of the journal, its editors, or the sponsoring society.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.
Positionality Disclosure
The authors are affiliated with three different teaching institutions, each characterized by distinct work environments.
Prior Presentations
NA.
PROSPERO/CTRI Details
NA.
Simultaneous Submission to Another Journal or Resource
The authors confirm that this submission is original and not under consideration elsewhere.
Citation Diversity Statement
We have included diverse perspectives in our references by citing work from authors across different genders, geographic regions (including the Global South), and career stages. We have also aimed to represent a range of disciplinary viewpoints relevant to the topic.