
Abstract

Inclusion Criteria
In addition to the eligibility criteria mentioned in the published article, studies that included participants with subclinical diagnostic thresholds were also eligible. This correction applies to the abstract, PRISMA flow chart, and method section.
Methods
In accordance with the commentator’s suggestions, 1 details on the “dppc2” method for estimating effect size and standard errors are being supplemented. As “dppc2” was computed with three imputed correlations (r = 0.25, 0.50, 0.75). We applied imputation to study-level correlations within this range, selecting the minimum correlation that yields variance intervals between 0.075 and 0.025. Furthermore, sensitivity analyses were conducted using different imputed correlation values, and subgroup analyses were conducted based on diagnostic threshold (clinical vs. subclinical), illness phase, and risk of bias.
Results
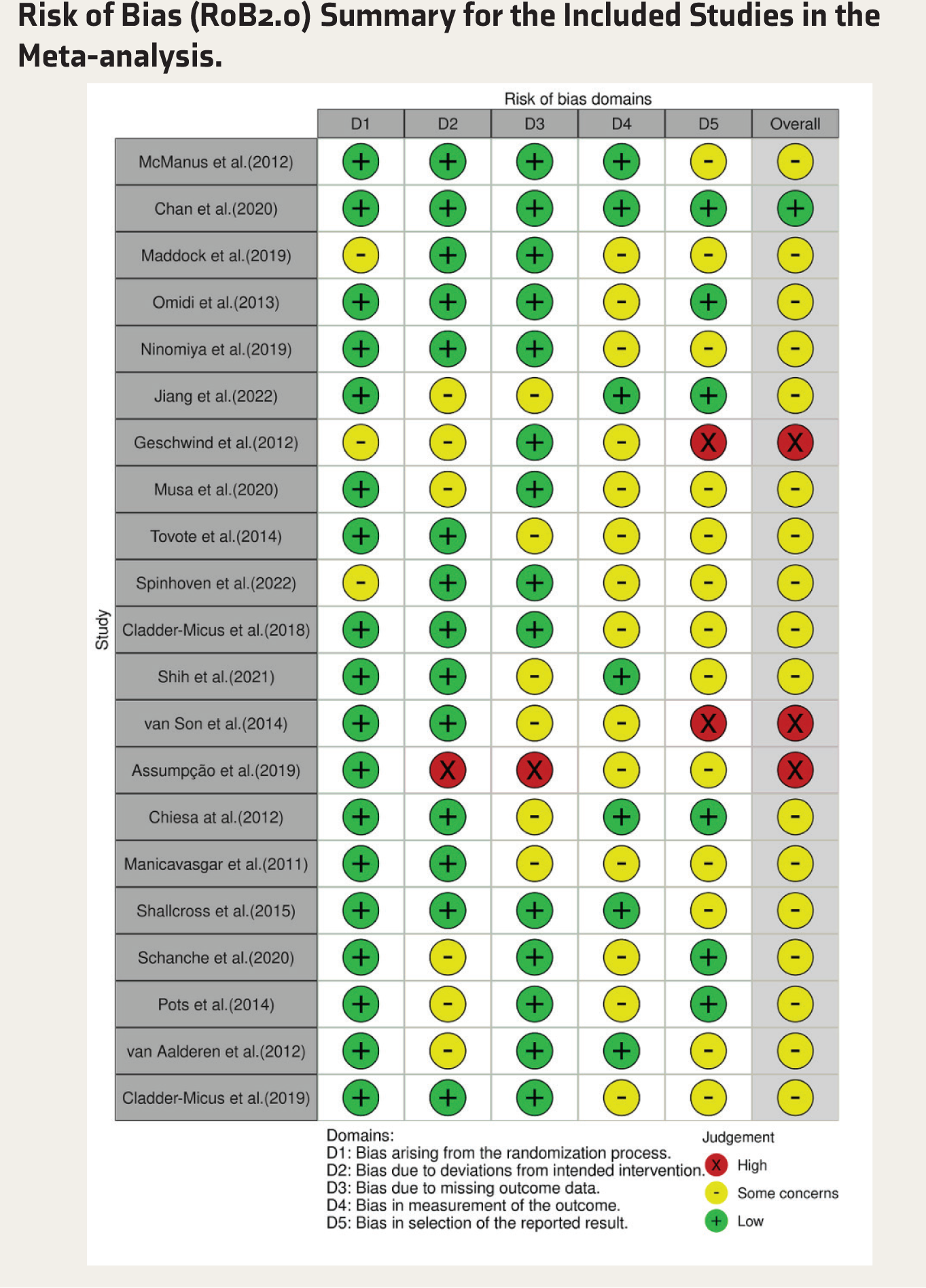
Following the commentator’s recommendations, Table 1 was revised, and a detailed account of the diagnostic threshold, current disease stage, and outcome assessment measures is provided for all included studies (see revised Table 1). The traffic light plot (Figure 2) is also corrected, as our previous RoB 2.0 evaluations were heavily influenced, as recommended by Munder and Barth for psychotherapy-based RCTs. After revision, now most studies are rated as having some concerns (see revised Figure 2).
Characteristics of Included Studies.
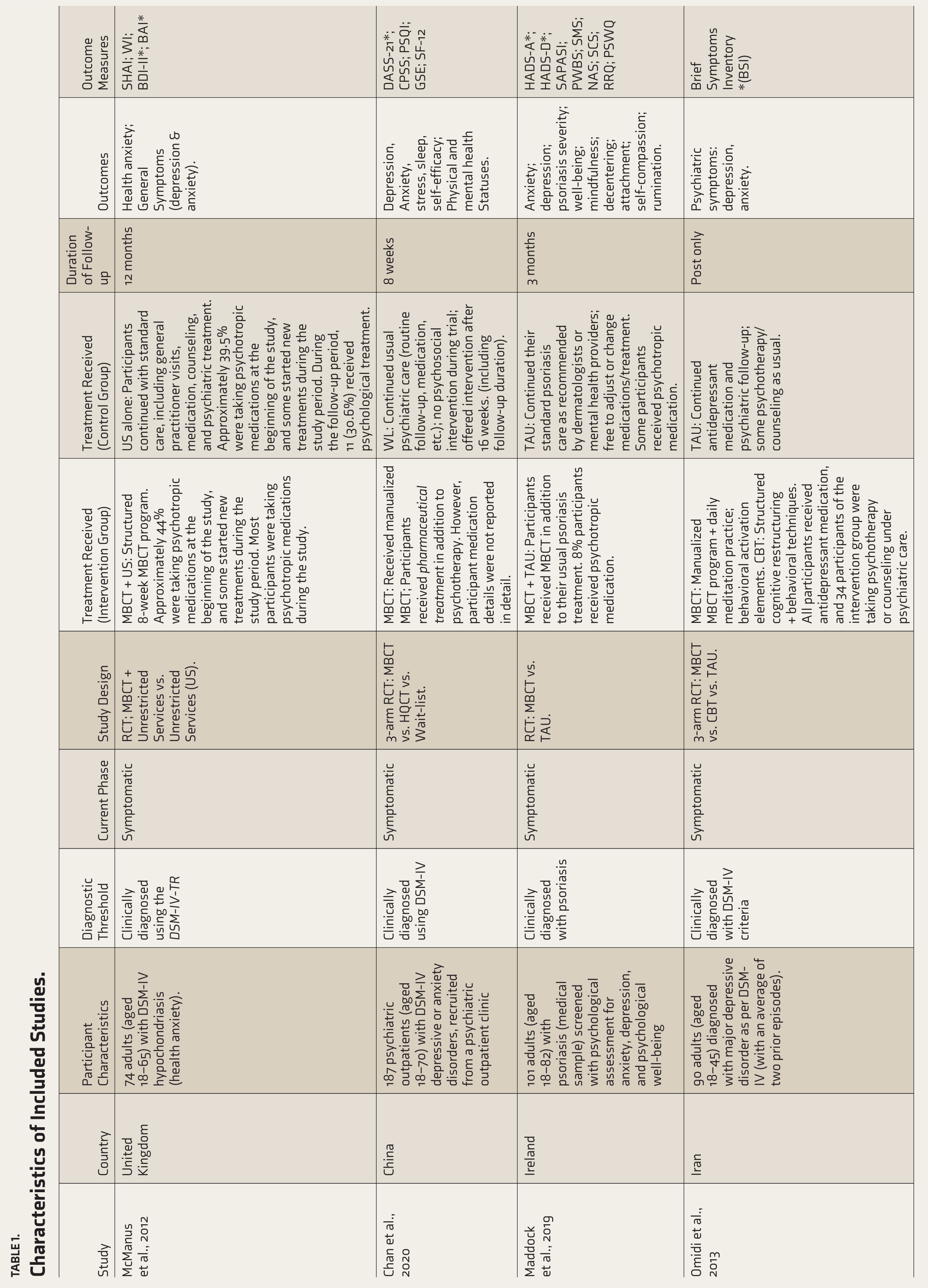
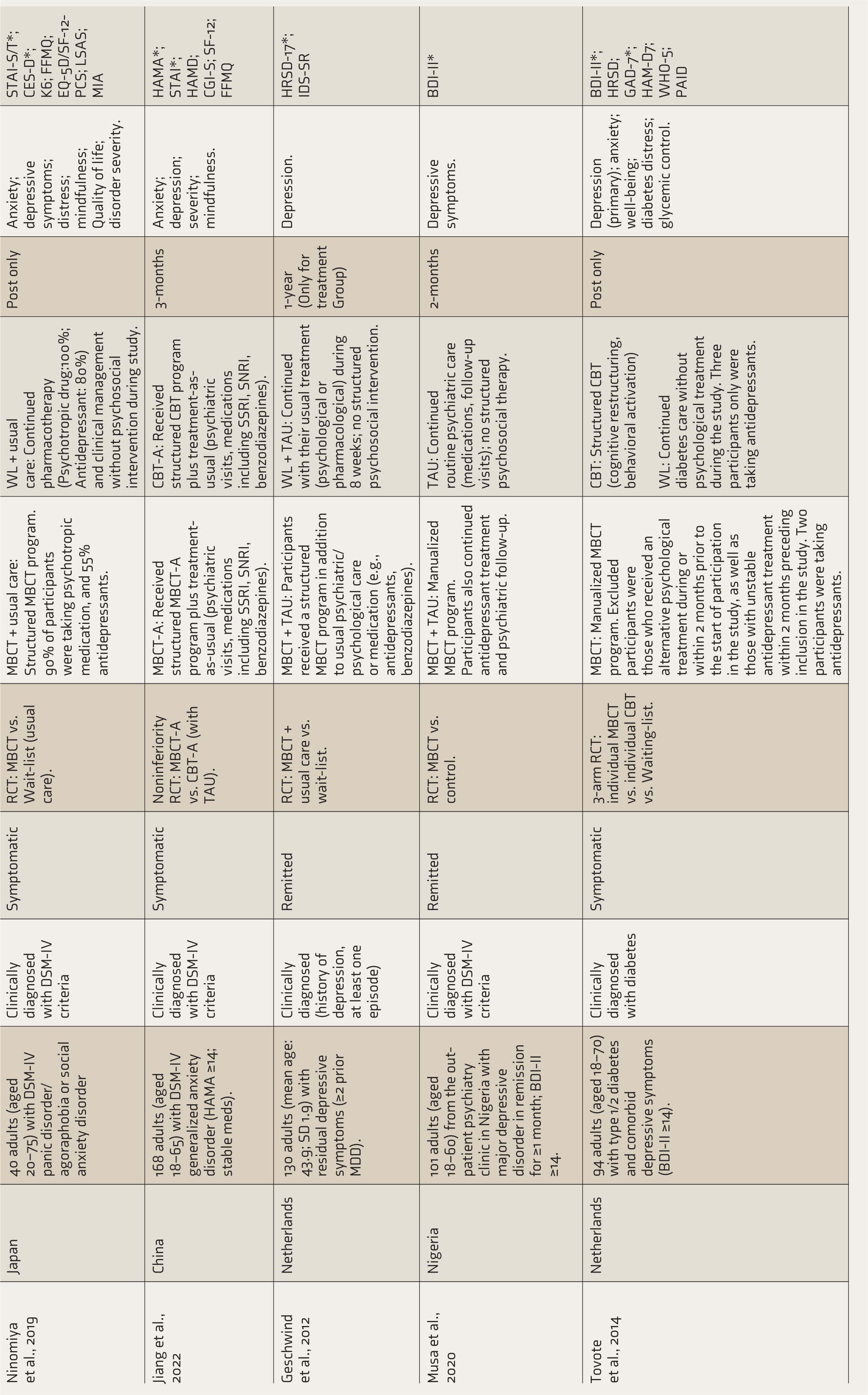
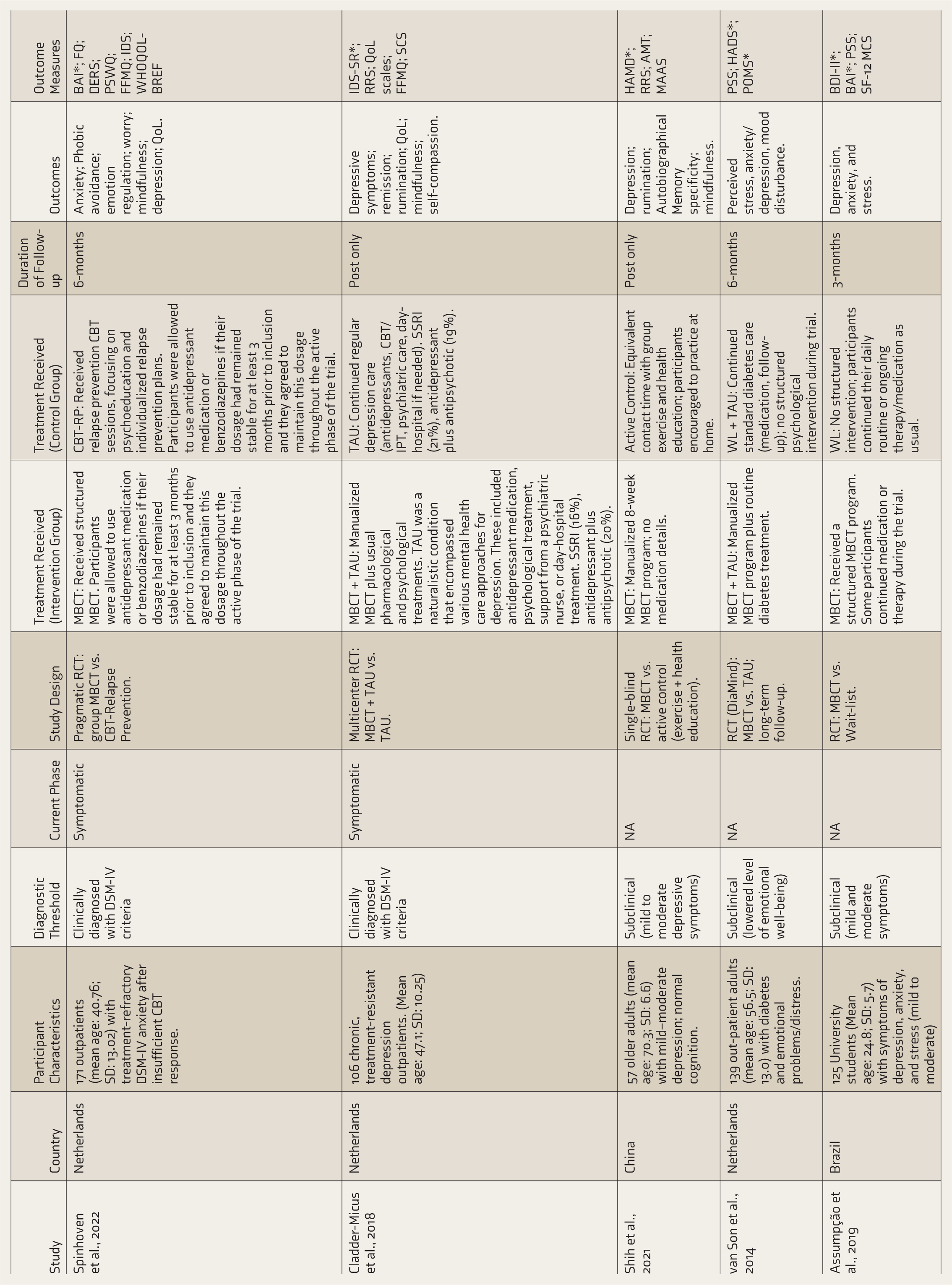
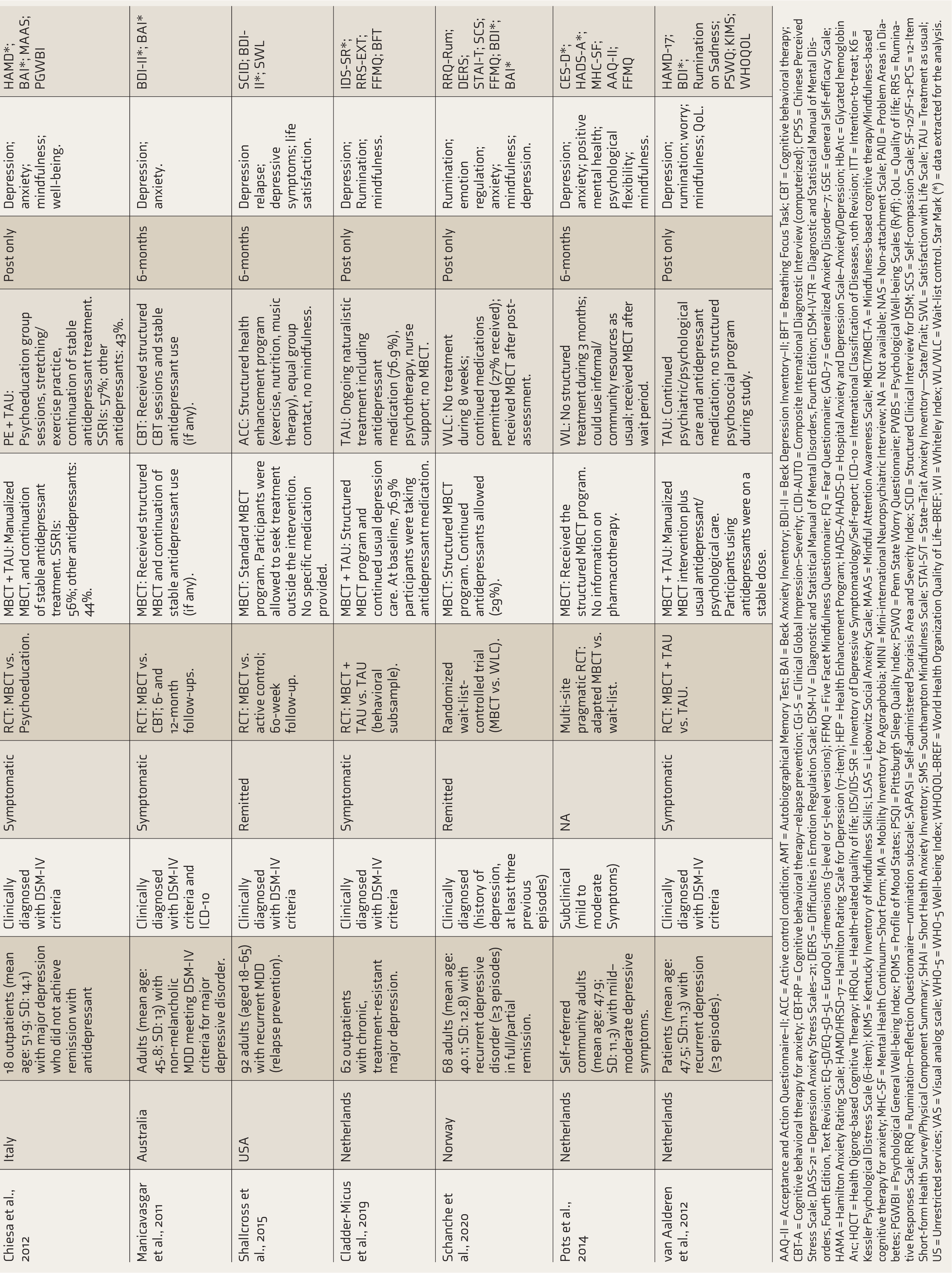
AAQ-II = Acceptance and Action Questionnaire–II; ACC = Active control condition; AMT = Autobiographical Memory Test; BAI = Beck Anxiety Inventory; BDI-II = Beck Depression Inventory–II; BFT = Breathing Focus Task; CBT = Cognitive behavioral therapy; CBT-A = Cognitive behavioral therapy for anxiety; CBT-RP = Cognitive behavioral therapy–relapse prevention; CGI-S = Clinical Global Impression–Severity; CIDI-AUTO = Composite International Diagnostic Interview (computerized); CPSS = Chinese Perceived Stress Scale; DASS-21 = Depression Anxiety Stress Scales–21; DERS = Difficulties in Emotion Regulation Scale; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; EQ-5D/EQ-5D-5L = EuroQol 5-dimensions (3-level or 5-level versions); FFMQ = Five Facet Mindfulness Questionnaire; FQ = Fear Questionnaire; GAD-7 = Generalized Anxiety Disorder–7; GSE = General Self-efficacy Scale; HAMA = Hamilton Anxiety Rating Scale; HAMD/HRSD-17 = Hamilton Rating Scale for Depression (17-item); HEP = Health Enhancement Program; HADS-A/HADS-D = Hospital Anxiety and Depression Scale–Anxiety/Depression; HbA1c = Glycated hemoglobin A1c; HQCT = Health Qigong-based Cognitive Therapy; HRQoL = Health-related quality of life; IDS/IDS-SR = Inventory of Depressive Symptomatology/Self-report; ICD-10 = International Classification of Diseases, 10th Revision; ITT = Intention-to-treat; K6 = Kessler Psychological Distress Scale (6-item); KIMS = Kentucky Inventory of Mindfulness Skills; LSAS = Liebowitz Social Anxiety Scale; MAAS = Mindful Attention Awareness Scale; MBCT/MBCT-A = Mindfulness-based cognitive therapy/Mindfulness-based cognitive therapy for anxiety; MHC-SF = Mental Health Continuum–Short Form; MIA = Mobility Inventory for Agoraphobia; MINI = Mini-international Neuropsychiatric Interview; NA = Not available; NAS = Non-attachment Scale; PAID = Problem Areas in Diabetes; PGWBI = Psychological General Well-being Index; POMS = Profile of Mood States; PSQI = Pittsburgh Sleep Quality Index; PSWQ = Penn State Worry Questionnaire; PWBS = Psychological Well-being Scales (Ryff); QoL = Quality of life; RRS = Ruminative Responses Scale; RRQ = Rumination–Reflection Questionnaire—rumination subscale; SAPASI = Self-administered Psoriasis Area and Severity Index; SCID = Structured Clinical Interview for DSM; SCS = Self-compassion Scale; SF-12/SF-12-PCS = 12-Item Short-form Health Survey/Physical Component Summary; SHAI = Short Health Anxiety Inventory; SMS = Southampton Mindfulness Scale; STAI-S/T = State–Trait Anxiety Inventory—State/Trait; SWL = Satisfaction with Life Scale; TAU = Treatment as usual; US = Unrestricted services; VAS = Visual analog scale; WHO-5 = WHO-5 Well-being Index; WHOQOL-BREF = World Health Organization Quality of Life–BREF; WI = Whiteley Index; WL/WLC = Wait-list control. Star Mark (*) = data extracted for the analysis.
Risk of Bias (RoB2.0) Summary for the Included Studies in the Meta-analysis.
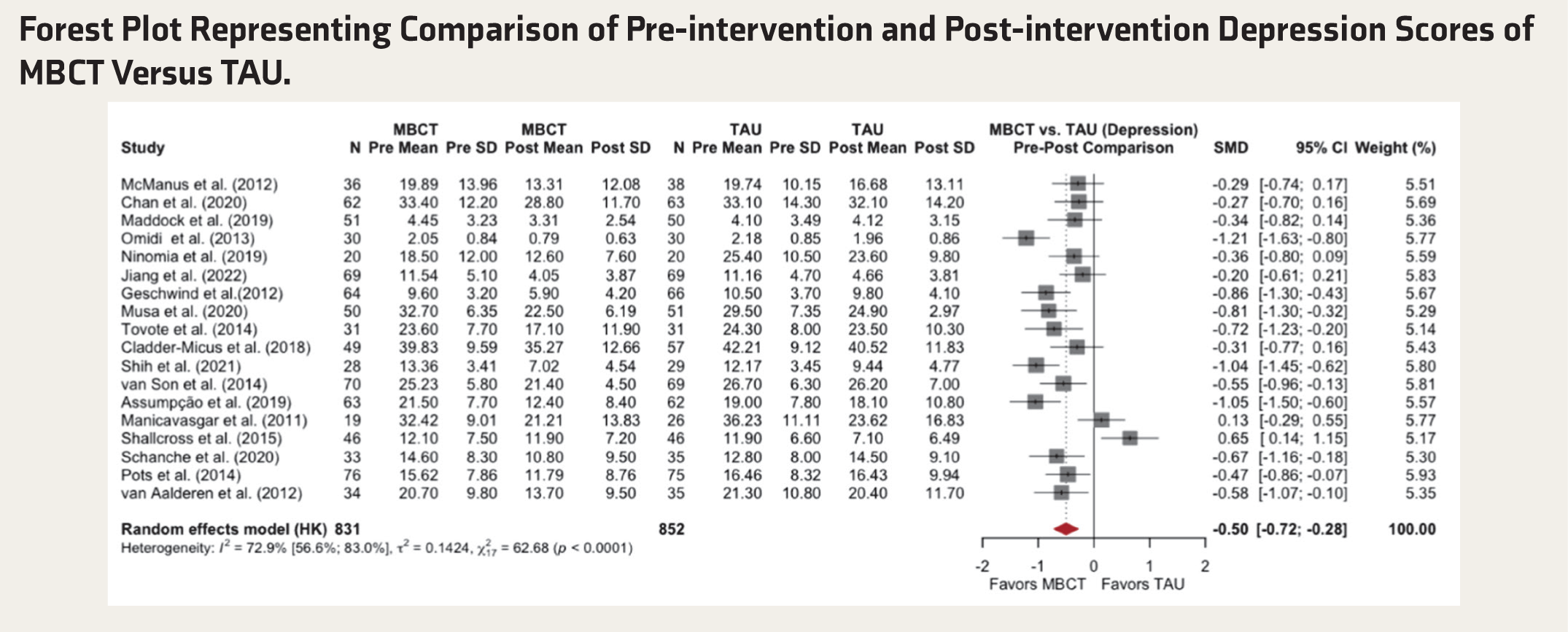
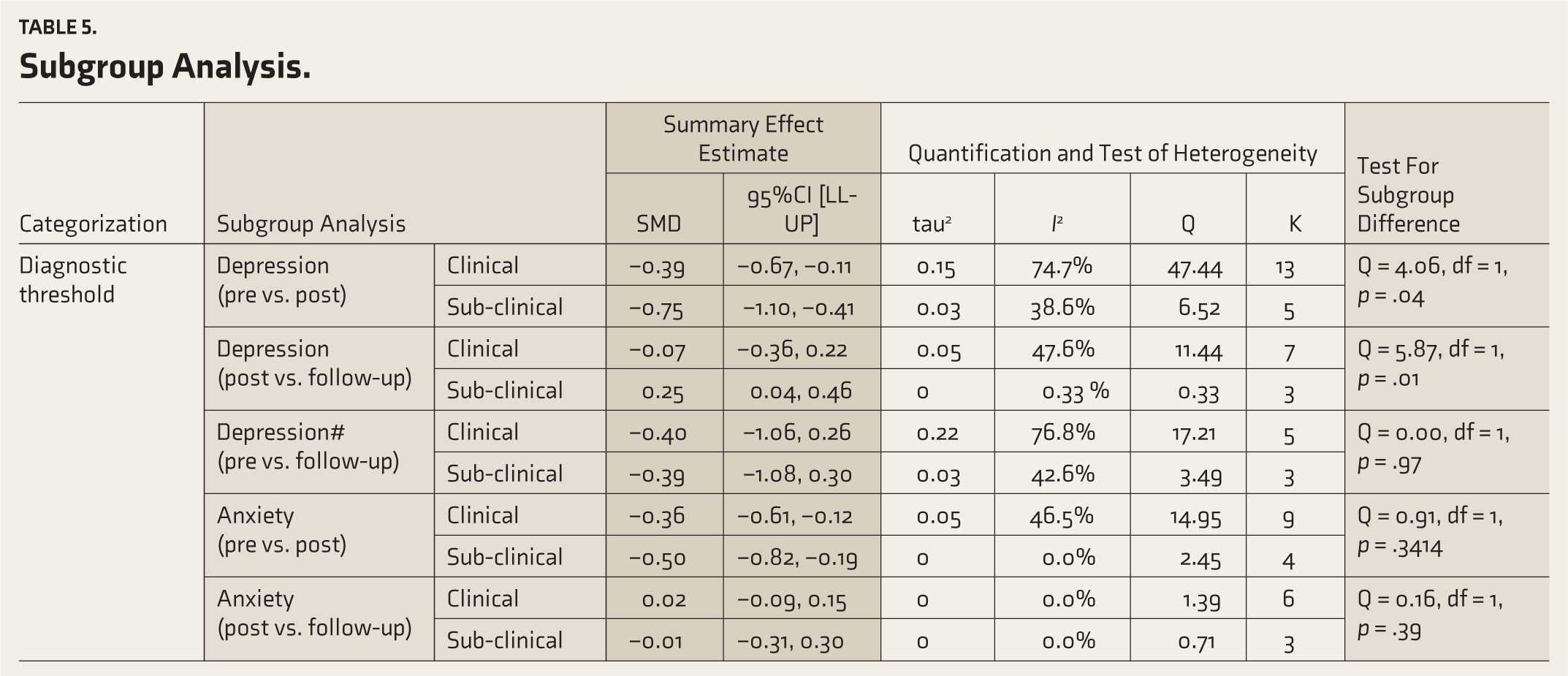
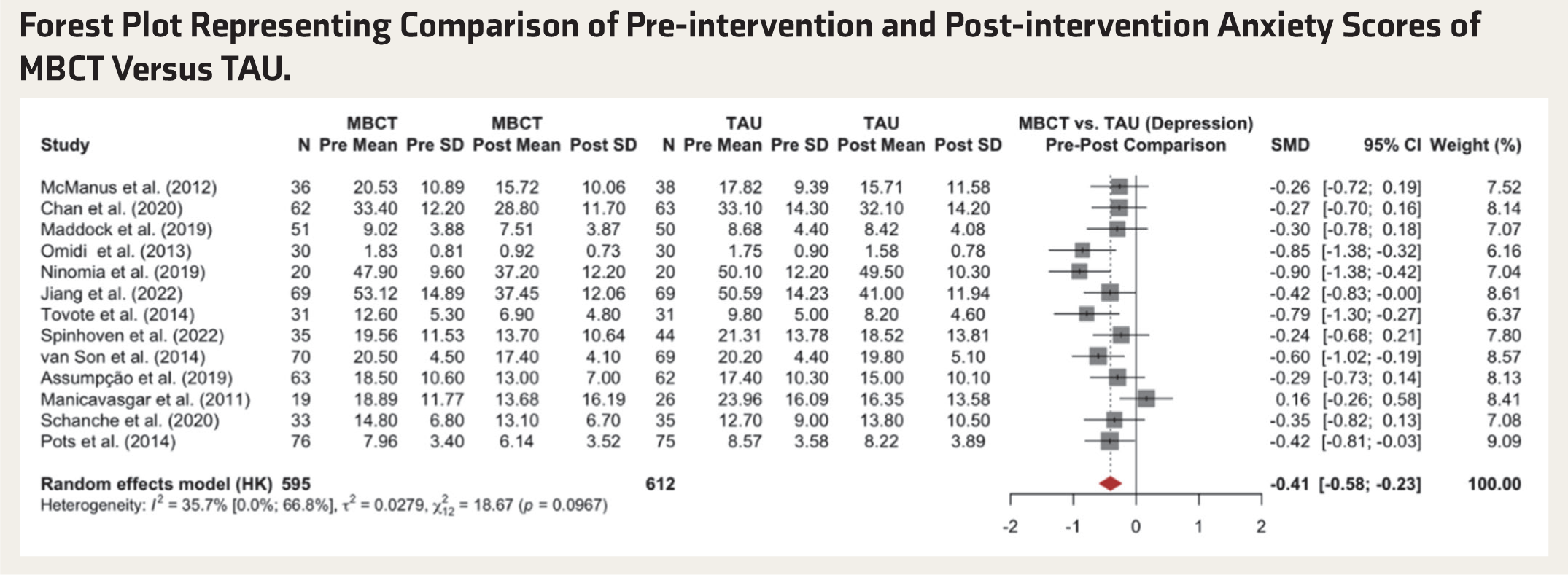
In response to the commentators’ comments and the methodological debate regarding the use of a fixed correlation value in dppc2, we imputed study-level correlations in the revised analyses. Similar to the published findings, MBCT significantly reduces depressive symptoms compared with TAU (SMD = –0.50, p < .001; I2 = 72.9%). For anxiety, MBCT produced significant symptom reduction (SMD = –0.40, p < .001; I2 = 36%) (revised Tables 2–4). Further, commentators raised concerns about unexplained heterogeneity; subgroup analyses were conducted, and the findings revealed that MBCT is more effective for subclinical than for clinical depression (SMD = –0.75 vs. –0.40). No subgroup differences were found based on the current phase of illness and risk of biases, both for anxiety and depression (Table 5).
Forest Plot Representing Comparison of Pre-intervention and Post-intervention Depression Scores of MBCT Versus TAU.
Consolidated Corrections to Table 2-4 in the Published Article.
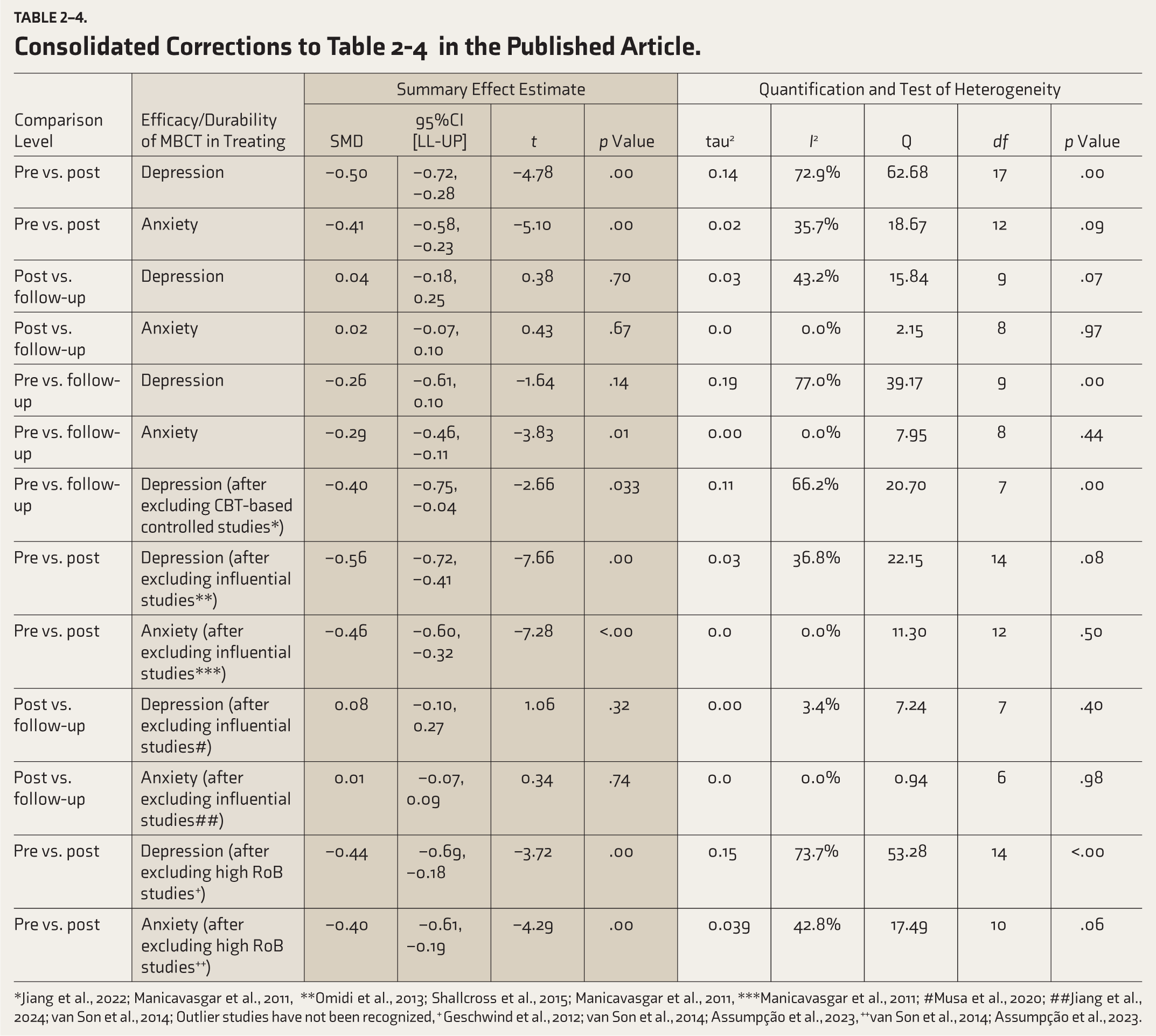
*Jiang et al., 2022; Manicavasgar et al., 2011, **Omidi et al., 2013; Shallcross et al., 2015; Manicavasgar et al., 2011, ***Manicavasgar et al., 2011; #Musa et al., 2020; ##Jiang et al., 2024; van Son et al., 2014; Outlier studies have not been recognized, + Geschwind et al., 2012; van Son et al., 2014; Assumpção et al., 2023, ++van Son et al., 2014; Assumpção et al., 2023.
Subgroup Analysis.
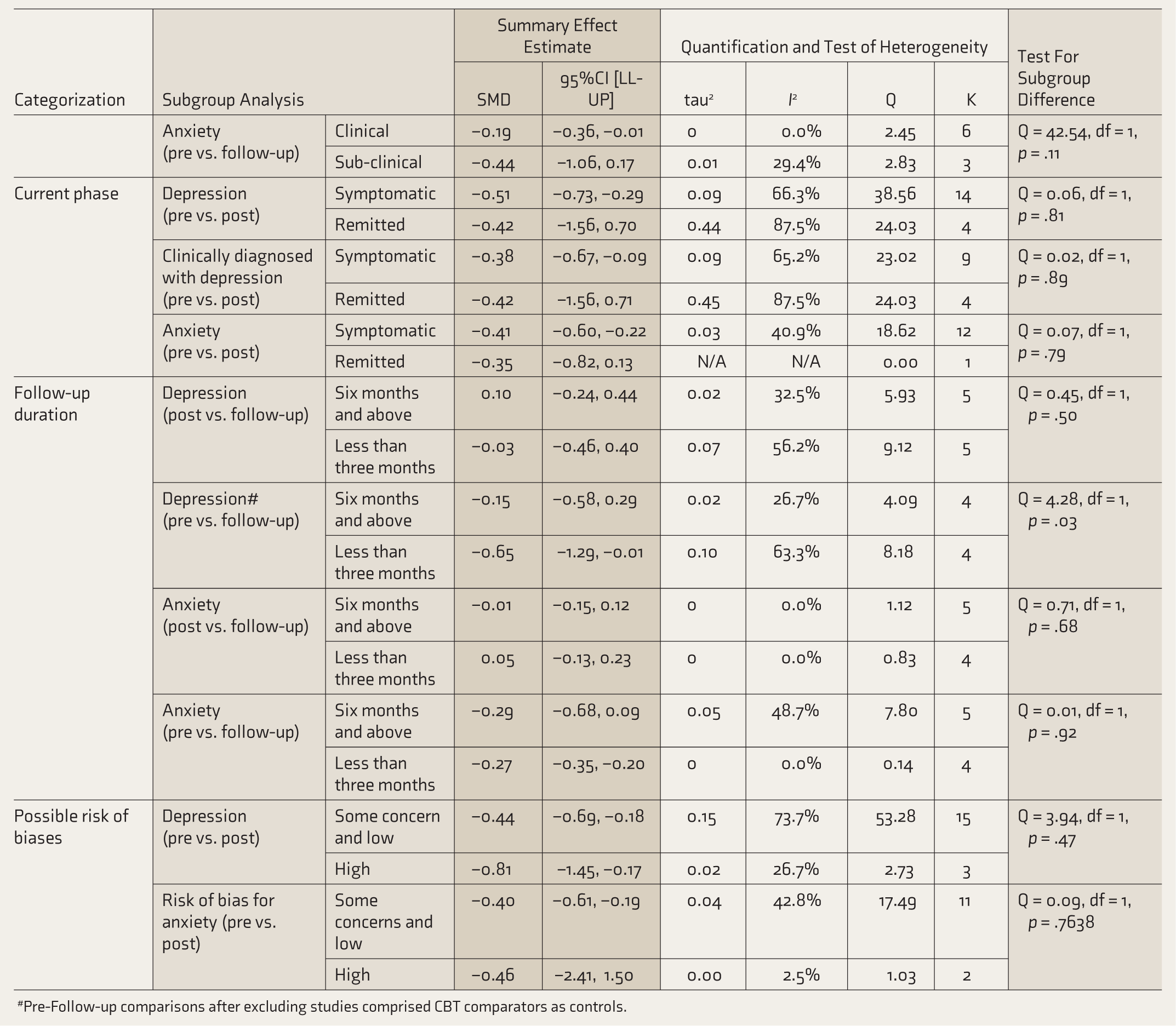
#Pre-Follow-up comparisons after excluding studies comprised CBT comparators as controls.
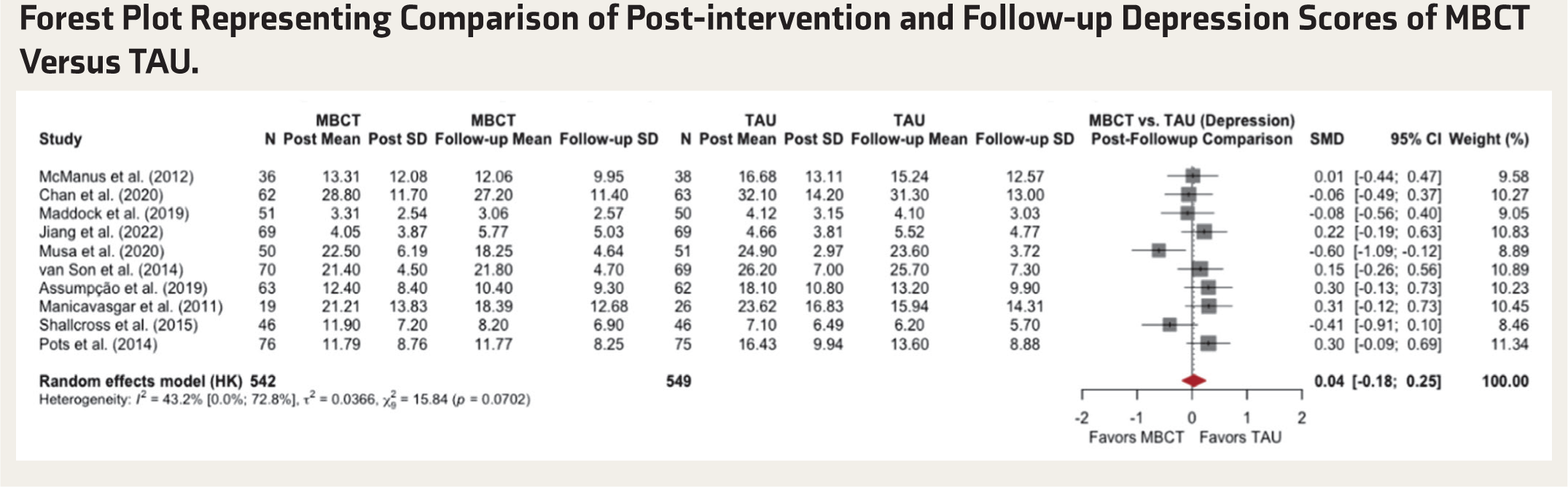
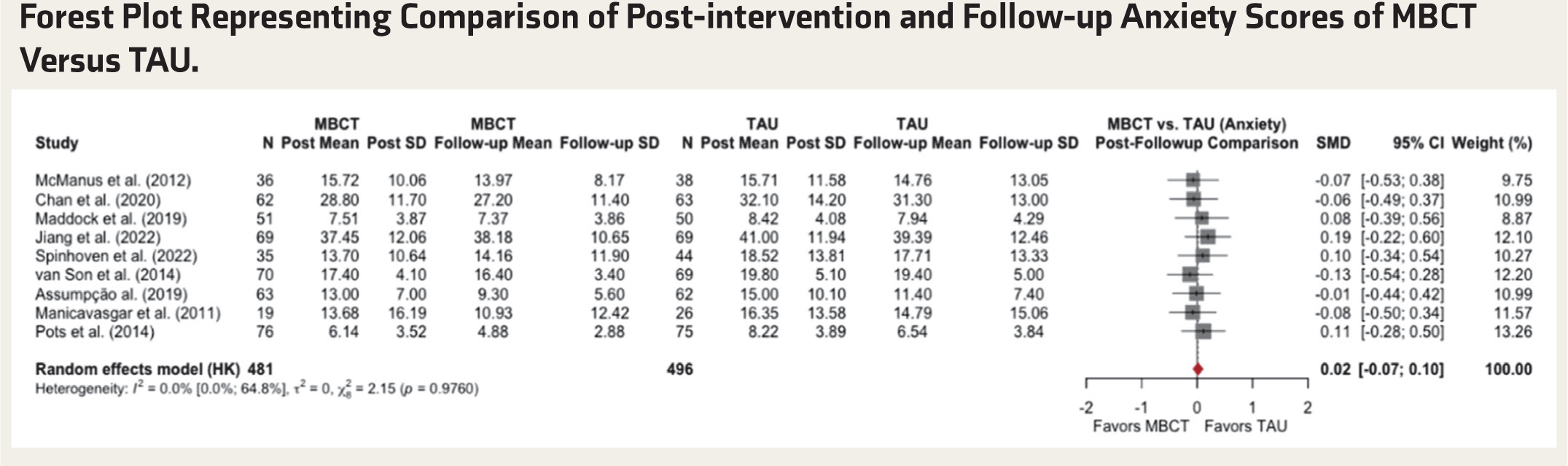
Similar to the original manuscript, MBCT showed durability in treating both depression and anxiety, as differences between post-intervention and follow-up period scores were non-significant for depression (SMD = 0.03) and anxiety (SMD = 0.02). As per the commentators’ comments regarding the definition of durability, we add analysis related to baseline-to-follow-up comparisons, and findings also confirmed the durability of MBCT in managing depression (after excluding those studies that used CBT as a control group) and anxiety-related symptoms (revised Figures 3–6; Tables 2–4). As per the subgroup analysis for depression, short-term follow-ups (<3 months) showed better maintenance of symptom reductions (SMD = –0.65) than long-term follow-ups (≥6 months; SMD = –0.15) (Table 6).
Forest Plot Representing Comparison of Pre-intervention and Post-intervention Anxiety Scores of MBCT Versus TAU.
Forest Plot Representing Comparison of Post-intervention and Follow-up Depression Scores of MBCT Versus TAU.
Forest Plot Representing Comparison of Post-intervention and Follow-up Anxiety Scores of MBCT Versus TAU.
Sensitivity Analysis of Imputed Pre-post Correlations (r) on Aggregated MBCT Treatment Effect on Anxiety and Depression.
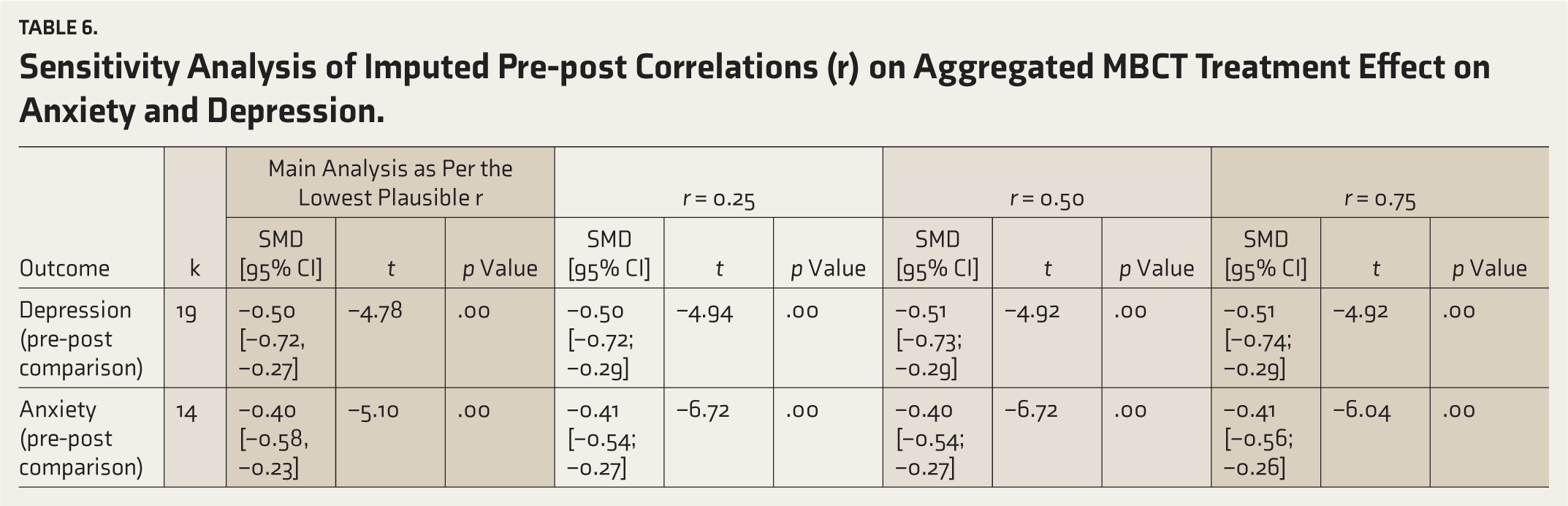
Lastly, as per the commentators’ comments, we performed a sensitivity analysis with different imputed correlation values, and all the findings were similar to the main findings, indicating the robustness of the results (Table 6).
Conclusion
As per the revised analysis and commentators’ comments, the overall findings should be interpreted with caution, as most of the included studies were rated as “some concerns” of bias, and the results showed moderate to high heterogeneity.
Figures
In response to the commentator’s comments, pre-, post-, and follow-up outcome scores (both mean and SD) and the number of participants in each study are included in the forest plots (revised Figures 3–6).
Reference
Nandarathana, Nikapitiye: 0009-0000-2530-5597
Jay Kumar Ranjan: 0000-0002-5948-9360
Incorrect: Musa ZA, Lam SK, Mamat FB, et al. Effectiveness of mindfulness-based cognitive therapy on the management of depressive disorder: systematic review. Int J Africa Nurs Sci, 2020; 12: 100200.
Correct: Musa ZA, Soh KL, Mukhtar F, et al. Impact of mindfulness-based cognitive therapy on depressive symptoms reduction among depressed patients in Nigeria: a randomized controlled trial. Issues Ment Health Nurs 2020; 42(7): 667–675. DOI: 10.1080/01612840.2020.1821139
The authors are grateful to the commentators for raising their concerns, and we apologize for these errors. We also thank the reviewer for the critical analysis and thoughtful comments.
Footnotes
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.