
Abstract

Rajasthan has the highest number of natural-opioid users, unlike the global trend of heroin or prescription opioids. 1 Increasing difficulty in obtaining opium, due to legal issues or adulteration, may prompt dependent users to seek alternatives. 2 Opioid-containing herbal medicines are common in India as over-the-counter drugs. 3 Similar to natural opium, Ayurvedic and Unani preparations have cultural acceptance, fewer perceived side effects, and less harm.2,4 They are marketed for ailments such as cough and sexual health, and to improve wellness, often without ingredient or addictive potential information.5,6
A few of these Ayurvedic preparations are linked to lead toxicity, which can cause fatigue, abdominal pain, and anemia. 3 Since these tablets contain opioids, their uncontrolled use can lead to dependence 5 and may result in general harms related to opioid use. Unlike previous research on pharmaceutical or illegal opioids, our study focuses on opioid dependence from over-the-counter “wellness” products, exposing a regulatory gap. Five clinical cases challenge assumptions about the safety of traditional medicine, underscoring the need for stricter regulation and increased public awareness.
Case Report 1
A 55-year-old rural male farmer has had bipolar disorder in remission for four years on mood stabilizers. He also has nicotine dependence (40 years of chewable tobacco) and harmful alcohol use, but has been abstinent from alcohol for four years.
His opioid use started 15 years ago after a clavicle fracture, when he was prescribed tramadol. He developed tolerance and withdrawal symptoms when decreasing doses. In 2016, due to issues obtaining tramadol, he switched to natural opium (doda), which his neighbors commonly used. In 2020, to quit opium, he started taking “herbal” tablets recommended by his brother, believing they were a safe, non-addictive Ayurvedic alternative. The tablets were available as unlabeled small, round, black tablets in transparent packets. When he would consume these tablets, he would feel pleasant, and his pain would decrease. Whenever he would take fewer tablets, he would develop withdrawal symptoms (body aches/anxiety/diarrhea) more severe than what he experienced with doda. His use gradually increased from one to six to eight tablets daily. His preoccupation with these tablets increased too, as he would travel over 400 km monthly, spending most of his income and taking loans to buy these tablets. The patient now presented for de-addiction due to financial issues and trouble sourcing the tablets, unaware of health risks. He continued to deny worsening functioning and constipation as related to the herbal tablets, which he still viewed as harmless.
The patient had a Clinical Opiate Withdrawal Scale (COWS) 7 score of eight and was treated with 1.2 mg/day sublingual buprenorphine. The patient was offered opioid substitution therapy (OST) but refused due to logistical issues; hence, buprenorphine was tapered and stopped. The patient is currently doing well.
Case Report 2
A 25-year-old man from an urban area began using natural opium (afeem) three years ago due to peer pressure. He initially used less than 50 g monthly, once daily, but increased to 200 g three times daily, due to tolerance and craving. Spending more than ₹25,000 per month, he tried quitting a year ago as his use escalated and started being a significant financial burden to him, but was unable to quit on his own due to excessive withdrawals.
He visited a pharmacy and received an Unani paste called “Barshasha” containing opium, used as a cough suppressant. He was told to take a small pinch twice daily, but due to unresolved opium withdrawal, he consumed nearly 30 g daily, later increasing to 60 g, which is 60 times the recommended dose. He knew it was an opioid but viewed it as less harmful than natural opium. His opium use started costing him more than ₹20,000 monthly and would sometimes be unavailable, which prompted his visit for de-addiction. The patient had a COWS score of ten and was prescribed Tab Tapentadol 100 mg/day initially, as the patient was not willing for buprenorphine based detoxification or OST due to logistical issues; however, the patient did not perceive sufficient withdrawal control and restarted taking Ayurvedic tablets despite being offered alternative management options such as buprenorphine based detoxification or substitution therapy.
Case Report 3
A 45-year-old man presented with bipolar disorder and 18 years of natural opium (afeem) dependence, initially used as an aphrodisiac. He could not reduce intake due to withdrawal, craving, and sexual problems. He would also be unable to focus on anything else unless he had consumed opium. In 2023, he was admitted for an affective episode and treated with buprenorphine for opioid dependence, which was gradually tapered and stopped as the patient was unable to visit daily for OST.
He struggled to obtain buprenorphine locally, so a relative advised him to try “Kamini Vidrawan Ras,” claiming it mimicked opium’s effects. Marketed as increasing sexual performance and well-being, it was readily available at an Ayurvedic pharmacy. He continued purchasing it without any prescription, gradually increasing to six tablets daily, consuming one to two tablets every few hours, which helped manage withdrawal symptoms and sexual function. The tablets were round and black. Unaware of the risks or opium content, he was hospitalized in 2024 for an affective episode but kept using the drug after discharge. The patient is currently following up for psychotropics, but remains unmotivated to stop the herbal medication despite brief interventions.
Case Report 4
A 38-year-old man with six years of natural opium dependence (afeem) visited the de-addiction clinic. He started consuming afeem due to peer pressure, but tried to quit after recognizing its harms. All his attempts failed because of withdrawal symptoms, and he continued using opium for five more years.
He was recommended “Hamdard Barshasha” by a friend, marketed as a cough and cold remedy, but was told it would help him quit opium. He took two tablespoons daily, which effectively managed withdrawals. The stronger effect and intense euphoria led him to increase his intake to five to six tablespoons daily, nearly finishing a bottle each day, even though he would intend to consume a lesser quantity initially, and despite the financial issues it was causing him. Although “Papaver somniferum” was listed as an ingredient, the patient was unaware of dosage, tapering, and side effects. The patient found it readily available in stores and online without a prescription. He lacked knowledge about what he was consuming, and the practitioner did not provide details on opium quantity, contraindications, or drug interactions. The patient realized that trying to quit opium led to dependence on a stronger substance, with more severe cravings and withdrawal.
The patient had an initial COWS score of 11 initially, was prescribed 4 mg of buprenorphine, then increased to 8 mg, and was planned for detoxification as per the patient’s preference. The patient is now attending follow-ups, doing well, and is abstinent from opioid-containing Ayurvedic medication.
Case Report 5
A 41-year-old man with eight years of opium dependence sought help at a de-addiction clinic. He had never previously tried to quit, but decided to do so a month ago due to family relationship issues related to substance use. Four days after stopping, he experienced severe withdrawal symptoms such as body aches, rhinorrhea, lacrimation, diarrhea, anxiety, and sleep problems.
He visited an Ayurvedic doctor due to unbearable withdrawal symptoms, who prescribed “Tab. Kamini Vidrawan Ras (KVR)-80” or “Kamini Vidrawan,” claiming it contained only trace opium and could be taken freely. He started consuming thrice daily but soon developed tolerance and craving, increasing intake to six, consuming two tablets thrice a day, and ordering more online without a prescription, sometimes receiving bottles with no information on opium content.
It was much stronger than his previous opium, which had no effect when taken with Kamini Vidrawan. The patient noted his daily needs varied, sometimes consuming four to eight tablets, as he found he had no control over his intake. The practitioner did not advise tapering or discuss long-term effects on health or sexual function, despite the patient’s concerns. On presentation, his COWS score was zero, and he was started on buprenorphine 4 mg, which managed withdrawals. He chose outpatient detoxification due to logistical issues with OST, stopped the herbal medication, and is doing well at follow-ups.
In this case series, the diagnosis of opioid dependence was made according to the International Classification of Diseases, Eleventh Revision, 8 and withdrawal severity was assessed by COWS. 7 We have used the case report (CARE) reporting guidelines. 9
A comparison of demographic and clinical profiles of five cases is shown in Table 1.
Comparison of Demographic and Clinical Profiles of Five Cases.
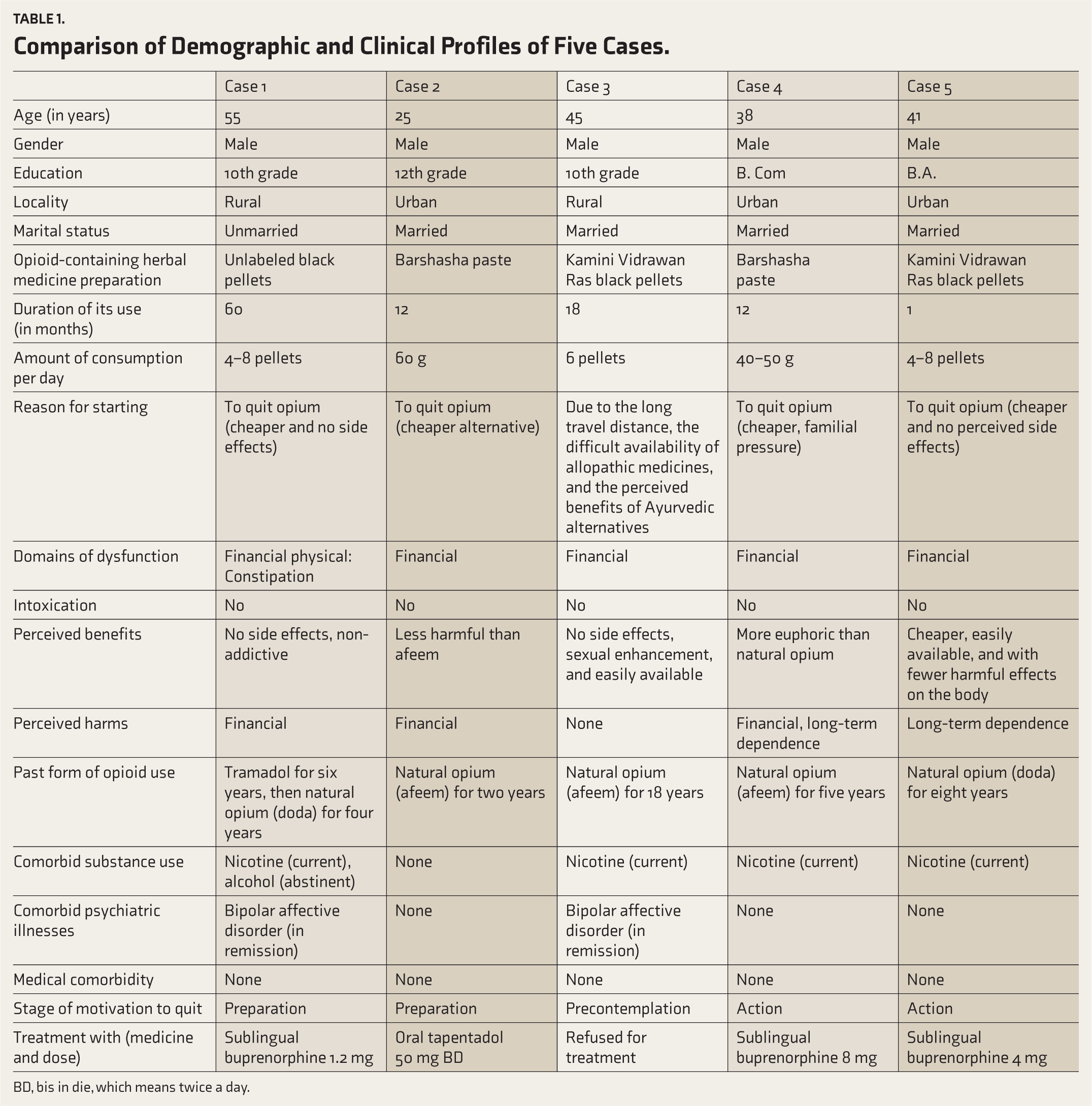
BD, bis in die, which means twice a day.
Discussion
This case series reports five males, aged 25–55, with confirmed opioid dependence. They used opium for 3–18 years and herbal opioids for one month to five years. Patients switched from natural opium (afeem/doda) to accessible Ayurvedic and Unani products such as “Kamini” and “Barshasha,” believing they were safe and non-addictive.
Ayurvedic and herbal products are regulated under the Drugs and Cosmetics Act and by the Ministry of AYUSH. Formulations containing opium are regulated as Schedule E1 drugs, which must carry mandatory labeling and must only be dispensed on a valid prescription via controlled channels, 10 yet this is not followed, as highlighted in all of our cases. All preparations containing opium also fall under the Narcotic Drugs and Psychotropic Substances (NDPS) Act, 1985. 11 Such products should be treated as controlled narcotics and not just herbal tonics, ensuring proper quality control and safety for de-addiction.
These cases highlight a growing public health concern, notably in Rajasthan, where natural opium use is common. 1 A key issue is iatrogenic dependence, as patients use these products seeking healthier or cheaper opioid options. Users often turn to herbal alternatives or try to avoid legal issues. 12 In our group, products were recommended by relatives, friends, or local practitioners and pharmacists, often with misleading or no information. This misinformation exploits the cultural acceptance and perceived safety of traditional medicine and mirrors Rajasthan’s pattern of natural opium initiation.2,13 These products are marketed for cough, sexual performance (Case 3), or pain relief (Cases 1–5), reflecting the rural Rajasthan pattern of natural opium use. 14
The preparations discussed here, Barshasha and Kamini, are known to contain significant amounts of opium, as confirmed by their ingredient lists and previous studies.5,12,15 Kamini comes in 500 mg tablets with 160 mg of opium, while 60 g of Barshasha contains 1.67 g of opium. 15
Case series from India, 14 and countries with Indian diasporas, such as New Zealand, 16 and Australia,5,17,18 show a similar dependence on specific products, primarily affecting males. Kamini is the most cited, followed by Barshasha. Our patients exhibited increased use, severe withdrawal, financial strain, and impaired functioning, consistent with other findings. 15
One key difference from the Australian case series5,17 is that all patients were already dependent on natural opium. They were not seeking a new high but rather a “harmless” way to escape addiction. This finding aligns with an Indian case series 15 but differs in that it reveals a more deceptive environment. Patients were often misled by friends or vendors, who sometimes denied opium, unlike the other study, where patients were more aware of opioid effects. Two of our five patients also had comorbid bipolar disorder. While neither developed opium-induced bipolar disorder, use of Kamini has been shown to trigger manic episodes, and patients must be psychoeducated regarding that. 19
Rajasthan’s large natural-opioid user base worsens the issue. Stricter laws on illegal opium may push users toward herbal substitutes, 2 which are poorly regulated, deceptively marketed, and lack labels, dosage information, or warnings. These products are sold online and in stores, as shown in our cases. While an Indian Ayurvedic report claims herbal opium risks are overstated, it too emphasizes the need for professional supervision, a precaution all five of our patients did not follow. 20
This regulatory gap fosters a new kind of opioid dependence disguised as wellness. Patients report that many young people purchase herbal medications with opioids, such as Indian Viagra, to enhance sex drive, risking an opioid dependence epidemic.
This case series is limited by its small size and the lack of toxicological analysis of the tablets to determine opioid content, especially for Case 1, as the tablets were not labeled, and the content was judged to be an opioid only based on the nature of withdrawals and effects. We also did not screen for adulterants, such as heavy metals, as reported in some Ayurvedic medicines. 3 Future studies should focus on large-scale research to estimate the prevalence of herbal opioid misuse, analyze product composition and potency variability, and evaluate prevention, regulation, and treatment strategies.
Conclusion
These cases show that herbal remedies containing opioids are not entirely safe and can unknowingly lead to opioid dependence. Our findings emphasize the importance of asking about Ayurvedic, Unani, or herbal treatments when discussing opioid use and sexual health. Be cautious of unlabeled products as potential sources of opioids. We recommend improved labeling, monitoring of over-the-counter sales, stricter regulation of Papaver somniferum formulations, use of these formulations only under the supervision of a qualified AYUSH doctor, and increased public education about the risks of addiction.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Appropriate Permissions from the Concerned Authorities
None.
Data Sharing Statements
The deidentified participant datasets generated and/or analyzed during the current study are not publicly available but can be obtained from the corresponding author upon reasonable request (Email:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Committee Details
No Institutional Ethics Committee (IEC) approval was required for the case studies. However, an IEC waiver has been obtained from the Institute’s Ethics Committee, as detailed below:
Name of the IEC/Independent Review Board: IEC AIIMS Jodhpur Ref. No: AIIMS/JDH/IEC/4870 Date: 10 September 2025
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants for their involvement in the study and for the publication of their data.
Prior Presentations
None.
PROSPERO/CTRI Details
Not applicable.
Registration
Not applicable.
Simultaneous Submission to Another Journal or Resource
None.
Status of Your Study (for Study Protocol)
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.