
Abstract

Obsessive-compulsive disorder (OCD) is a chronic neuropsychiatric disorder characterized by recurrent, intrusive thoughts (obsessions) and repetitive behaviors (compulsions) aimed at reducing anxiety. 1 Once considered rare, OCD is now recognized as a prevalent condition, with a lifetime prevalence of 1%–3% worldwide. 2 Twin studies have demonstrated a strong genetic component in OCD, with heritability estimates ranging from 40% to 65%. 3 However, the phenotypic variability observed in monozygotic twins suggests that environmental and epigenetic factors also play a critical role in shaping symptom expression. 4 This case series adds to the existing literature by documenting phenotypic divergence in both monozygotic and dizygotic twins with OCD, while also highlighting a rare pharmacogenetic vulnerability— fluoxetine-induced hyperpigmentation—occurring in both dizygotic siblings. Unlike earlier twin reports that primarily emphasized concordance or symptom overlap, our report underscores the multifactorial nature of OCD expression and management, integrating genetic, environmental, and treatment-related perspectives. The novelty lies in combining divergent clinical phenotypes with an unusual shared adverse drug reaction, thereby advancing understanding of individualized treatment strategies and the importance of vigilance for rare side effects in genetically related individuals. Written informed consent for participation and publication was obtained from all patients. Ethical approval was obtained from the institutional ethics committee, and appropriate referrals and treatments were ensured for all detected abnormalities.
Case 1
This case shows 35-year-old monozygotic twin brothers from Central India, diagnosed with OCD 20 years ago. The diagnosis of OCD in both patients was established according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria. 5 Despite their shared genetic makeup and upbringing, their symptomatology and clinical presentation differed significantly. Informed consent was taken from both patients.
Twin A
Twin A’s OCD symptoms were primarily centered on contamination fears, leading to compulsive hand washing and checking behaviors. He also experienced distressing sexual obsessions, which he attempted to neutralize by imagining inappropriate sexual scenarios. His pre-treatment score on the Yale-Brown obsessive-compulsive scale (Y-BOCS) 6 was 30, indicating severe OCD. These symptoms significantly impaired his interpersonal relationships and occupational functioning.
Twin B
In contrast, Twin B’s OCD symptoms revolved around perfectionism and symmetry. While he exhibited some checking behaviors, he did not engage in overt compulsions, such as handwashing. Similar to Twin A, he experienced sexual obsessions but relied on mental rituals to alleviate distress. His pre-treatment Y-BOCS score was 26, indicating moderate severity. Twin B’s symptoms also disrupted his daily life, particularly in social and professional contexts.
Past History
Only partial records from different periods were available. Both twins had poor drug compliance and limited response to treatment. Twin A had an adequate trial of escitalopram up to 30 mg/day, which was his mainstay for several years, and about 5–6 years earlier had briefly taken fluoxetine 20 mg/day but discontinued due to poor tolerability. He also attempted cognitive behavioral therapy (CBT) around seven years ago but dropped out after three sessions. Twin B had been on fluvoxamine up to 100 mg/day in the past with minimal benefit. Neither had received structured CBT before the current episode.
Treatment and Prognosis
Both twins received standard evidence- based treatments for OCD, including CBT and selective serotonin reuptake inhibitors (SSRIs), tailored to their distinct symptom profiles. Twin A was started on sertraline (200 mg/day) with aripiprazole augmentation (5 mg/day) and underwent exposure and response prevention (ERP) for contamination fears and sexual obsessions. Twin B was prescribed fluoxetine (60 mg/day) with risperidone augmentation (2 mg/day) and received CBT focusing on cognitive restructuring and ERP for perfectionism and mental rituals.
Twin A showed gradual improvement in managing obsessions, though compulsions persisted; his Y-BOCS score reduced to 16. Twin B’s response was more variable, with ongoing challenges related to perfectionism, and his Y-BOCS score at follow-up was 20.
Case 2
This case involves 19-year-old dizygotic twin sisters from Central India, diagnosed with OCD according to the DSM-5 criteria, but presenting with distinct symptom dimensions and illness courses. Informed consent was taken from both patients.
Twin C
Twin C reported an illness duration of approximately five years. Her symptoms were dominated by harm-related obsessions, including intrusive thoughts of harming family members or herself. These caused significant distress and avoidance behaviors, including avoidance of kitchens, balconies, and crowded spaces. She developed mental compulsions like silent prayers and frequent reassurance-seeking from family. Over time, she exhibited emotional lability, social withdrawal, and academic decline. Her baseline Y-BOCS score was 28, reflecting severe OCD with substantial functional impairment.
Twin D
Twin D had an illness duration of around seven years, characterized by contamination obsessions and compulsive handwashing—sometimes dozens of times a day. She also had checking compulsions, such as repeatedly verifying doors, switches, and taps. These rituals were time-consuming and caused significant academic impairment and interpersonal conflict at home. Initially, she had limited insight, but later recognized the irrationality of her behavior. Her baseline Y-BOCS score was 25, indicating moderate to severe OCD.
Past History
Both twins had been receiving psychiatric treatment from another practitioner for approximately one year prior to presentation. Twin C had an earlier trial of escitalopram up to 20 mg/day for about 12 weeks, with no significant response. Twin D was already receiving fluoxetine 60 mg/day at the time of presentation. Neither had received structured CBT before the current episode.
Treatment and Prognosis
Twin C was initially started on fluoxetine, gradually titrated to 80 mg/day, alongside structured CBT. After approximately eight weeks of initiation of fluoxetine, she developed hyperpigmented macular lesions on her forearms along with mild symptoms suggestive of serotonin overload, including restlessness, sweating, and irritability. Despite the high dose, she exhibited minimal clinical improvement. The Naranjo Adverse Drug Reaction Probability Scale,7 score was calculated as 8, indicating a probable association between fluoxetine and the observed hyperpigmentation. Consequently, fluoxetine was tapered over one week, and she was initiated on sertraline, which was gradually titrated to 200 mg/day over two months. Additionally, risperidone was added at 2 mg/day for augmentation. Over the next four months, her Y-BOCS score improved significantly, reducing to 14, and her hyperpigmentation resolved.
Twin D was already taking fluoxetine 60 mg and demonstrated partial symptomatic improvement. In view of this, the dose was increased to 80 mg/day, following which she showed further clinical response; however, six weeks after dose escalation, she developed hyperpigmented macules involving the lips and perioral region. The Naranjo Adverse Drug Reaction Probability Scale score 7 was calculated as 9, indicating a probable association between fluoxetine and the observed hyperpigmentation. Due to cosmetic concerns and the potential risk of worsening pigmentation, fluoxetine was discontinued. She was subsequently started on sertraline and showed a clinical response at 150 mg/day without further adverse effects. Her compulsions reduced notably, and her Y-BOCS score decreased to 16 over three months. Both twins received tailored CBT with ERP; Twin C’s therapy focused on cognitive restructuring and harm-related exposures, while Twin D’s sessions targeted contamination fears and checking rituals. Both demonstrated good engagement and adherence throughout treatment.
Discussion
This report constitutes a case series of two twin pairs (one monozygotic and one dizygotic) comprising four individuals in total, each diagnosed with OCD but presenting with distinct symptom "dimensions and clinical trajectories (Table 1). The case series offers valuable insights into the phenotypic diversity, treatment responsiveness, and rare adverse effects associated with OCD. Despite shared familial and environmental backgrounds, all four individuals displayed divergent presentations, " underscoring the complex interaction between genetic, neurodevelopmental, and psychosocial factors in the manifestation of OCD.
Comparative Clinical Summary of Obsessive-compulsive Disorder in Monozygotic and Dizygotic Twin Pairs.
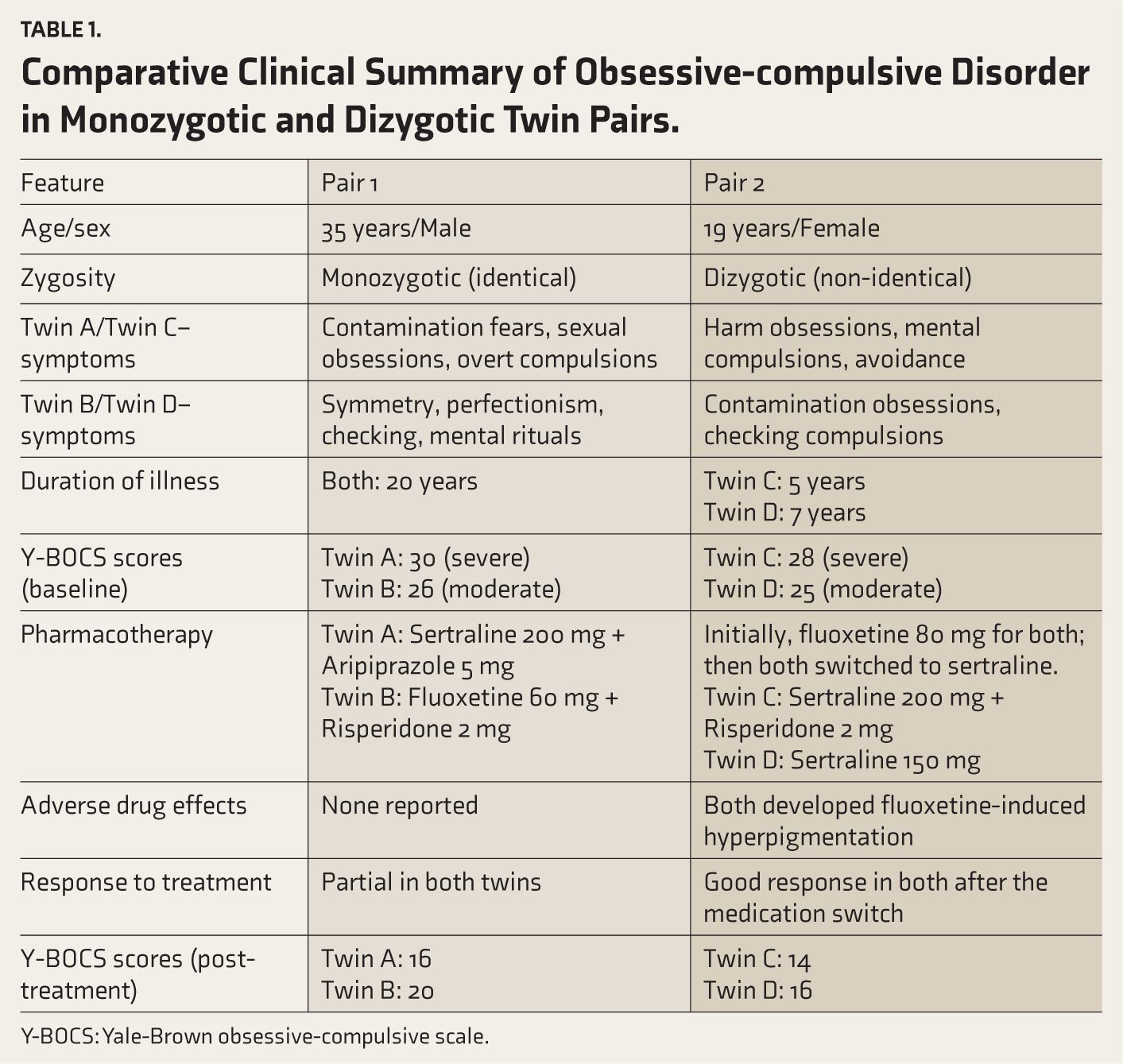
Y-BOCS: Yale-Brown obsessive-compulsive scale.
The monozygotic twin pair demonstrated divergent OCD profiles—one with contamination fears and overt washing compulsions, and the other with symmetry/perfectionism-related obsessions and mental rituals. In contrast, the dizygotic twin sisters, who share only approximately 50% of their genetic material, presented with distinct symptom dimensions: one had harm- related obsessions with covert mental compulsions, while the other exhibited contamination obsessions and overt checking behaviors. Given their shared genetic material and upbringing, this phenotypic divergence highlights the impact of non-shared environmental factors, developmental stressors, and possibly epigenetic modifications. Genetic studies support a heritability estimate of 40%–65% in OCD, but the expression of specific symptom dimensions appears to be shaped by additional factors beyond genetic predisposition.3,4,8 Their symptom divergence further supports the role of individual experiences, cognitive appraisals, and possibly different neural circuitry in the manifestation of OCD subtypes.9,10
A notable shared feature in the dizygotic twins was the development of fluoxetine-induced hyperpigmentation on the arms in one and around the lips in the other. This rare adverse effect may be related to melanin-drug binding or photosensitivity reactions. 11 The presence of this side effect in both individuals, despite different symptom clusters and differential drug response, raises the possibility of a shared pharmacogenetic vulnerability. 12
Following the medication switch to sertraline, both showed clinical improvement, with one requiring augmentation with risperidone. This aligns with evidence supporting augmentation with atypical antipsychotics in SSRI- refractory OCD, particularly for patients with intrusive thoughts or inadequate insight. 13 CBT, particularly ERP, was administered in both twin pairs and adapted to their predominant symptom clusters, in keeping with best-practice recommendations. 14
These cases are consistent with previous literature documenting discordant OCD phenotypes in twins. For example, a case report by Alvarenga et al. 15 described monozygotic twins with different OCD symptom dimensions and levels of severity. Similarly, a study by van Grootheest et al. 16 reviewed twin research on OCD and concluded that, despite high genetic concordance, monozygotic twins often display discordant symptom profiles, reinforcing the role of non-shared environmental factors and the need for a dimension-based diagnostic and therapeutic approach.
This case series highlights phenotypic divergence in both monozygotic and dizygotic twins with OCD, providing a unique comparative framework within a familial context. The inclusion of standardized symptom severity assessment (Y-BOCS), detailed treatment trajectories, and systematic evaluation of an unusual adverse drug reaction with the Naranjo scale strengthens the clinical and academic value of this report.
The primary limitation of this series lies in its observational nature and the absence of genetic or neuroimaging investigations, which could have offered deeper mechanistic insights into the divergent phenotypes. The small sample size, inherent to case series design, limits generalizability. Additionally, long-term follow-up was not systematically conducted, restricting conclusions about sustained treatment outcomes.
Conclusion
This case series of monozygotic and dizygotic twin pairs with OCD highlights the striking phenotypic divergence that can occur despite shared genetic and environmental backgrounds. The clinical variations observed underscore the multifactorial nature of OCD, where symptom expression and treatment response are shaped by a complex interplay of genetic, neurobiological, environmental, and possibly epigenetic factors. Notably, the shared experience of fluoxetine-induced hyperpigmentation among the dizygotic twins suggests potential pharmacogenetic susceptibility, warranting further investigation. These findings reinforce the need for personalized, symptom-dimension-oriented treatment strategies and vigilance for rare adverse drug reactions, especially in genetically related individuals. Future research exploring neurobiological correlates, gene-environment interactions, and individualized pharmacotherapy may further elucidate the pathways contributing to OCD heterogeneity.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Appropriate Permissions from the Concerned Authorities
Nil.
Data Sharing Statements
Deidentified individual participant data will not be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethics Committee Details
Name of the institutional ethics committee/independent review board: Institutional Ethics and Review Board, MGM Medical College and MY Hospital, Indore. Approval reference number: MGM/EC/2025/10. Date of approval: 10 June 2025.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Assent
Informed consent was obtained from all the patients
Prior Presentations
Nil.
PROSPERO/CTRI Details
Nil.
Simultaneous Submission
The manuscript has not been submitted simultaneously to another journal or resource.
Status of Your Study (for Study Protocol)
Completed.
Trial Registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.