
Abstract

Malaria continues to pose a major global health burden, with Plasmodium falciparum responsible for the most severe neurological complications. 1 While neuropsychiatric manifestations such as seizures, delirium, and coma are well recognized in acute cerebral malaria, delayed neuropsychiatric syndromes within 2 months after clinically proven recovered malaria and parasite clearance, collectively termed post-malaria neurological syndrome (PMNS), are less common and thought to be immune-mediated. 2 It occurs typically between 4 and 30 days after parasite clearance. A wide range of neuropsychiatric and neurological symptoms, including confusion, psychosis, ataxia, seizures, catatonia, myoclonus, mood disturbances, and movement abnormalities, characterizes it. 2 Unlike acute cerebral malaria, PMNS presents with a symptom-free interval following malaria treatment, normal neuroimaging, and negative parasitemia, making it diagnostically challenging and often mistaken for functional or primary psychiatric illness.1,2 Recognition of PMNS is clinically crucial in endemic regions, as its manifestations are typically transient and reversible with symptomatic treatment and supportive care, and do not require prolonged psychiatric or antipsychotic therapy.1,2 Awareness of this syndrome is essential to distinguish it from drug-induced effects, relapse of infection, or new-onset psychiatric disorders. We present three women with falciparum malaria who subsequently developed distinct, short-lived neuropsychiatric syndromes—complex motor tics, catatonia, and obsessive-compulsive symptoms—despite adequate treatment and parasite clearance, which has rarely been reported in the past. These cases expand the spectrum of PMNS and highlight reversible conditions that may otherwise be misdiagnosed as primary psychiatric illness.
Case Series
The patients presented to a tertiary-care health center in a mining and industrial belt in Jharkhand; their clinical information is detailed below and in Table 1. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision, was used for diagnosis. 3 No past history or family history of mental illness and substance use, or chronic medical illness, was present. All patients were initially diagnosed with Plasmodium falciparum malaria by peripheral smear and quantitative buffy coat estimation (QBCe). All patients received 3 days of artemether-lumefantrine, primaquine on day 2, and paracetamol 650 mg as needed for fever. These were prescribed in accordance with the national guidelines for malaria treatment. 4 Complete blood counts, liver, and renal function tests, serum electrolytes, blood sugar, and thyroid function tests were unremarkable, with higher C-reactive protein levels in all the cases. Non-contrast computed tomography of the brain and QBCe performed after the onset of neuropsychiatric symptoms were normal in all cases. The Bush–Francis Catatonia Rating Scale 5 and the Yale–Brown Obsessive Compulsive Scale 6 were used to assess Cases 2 and 3, respectively. No psychiatric symptoms or neurocognitive deficits were found till 3 months of follow-up after discharge. Written informed consent was obtained from the patients for publication purposes. CARE reporting guidelines were used to report this case series. 7 All patients reported sustained improvement at the time of discharge and during the follow-up period.
Case Summaries.
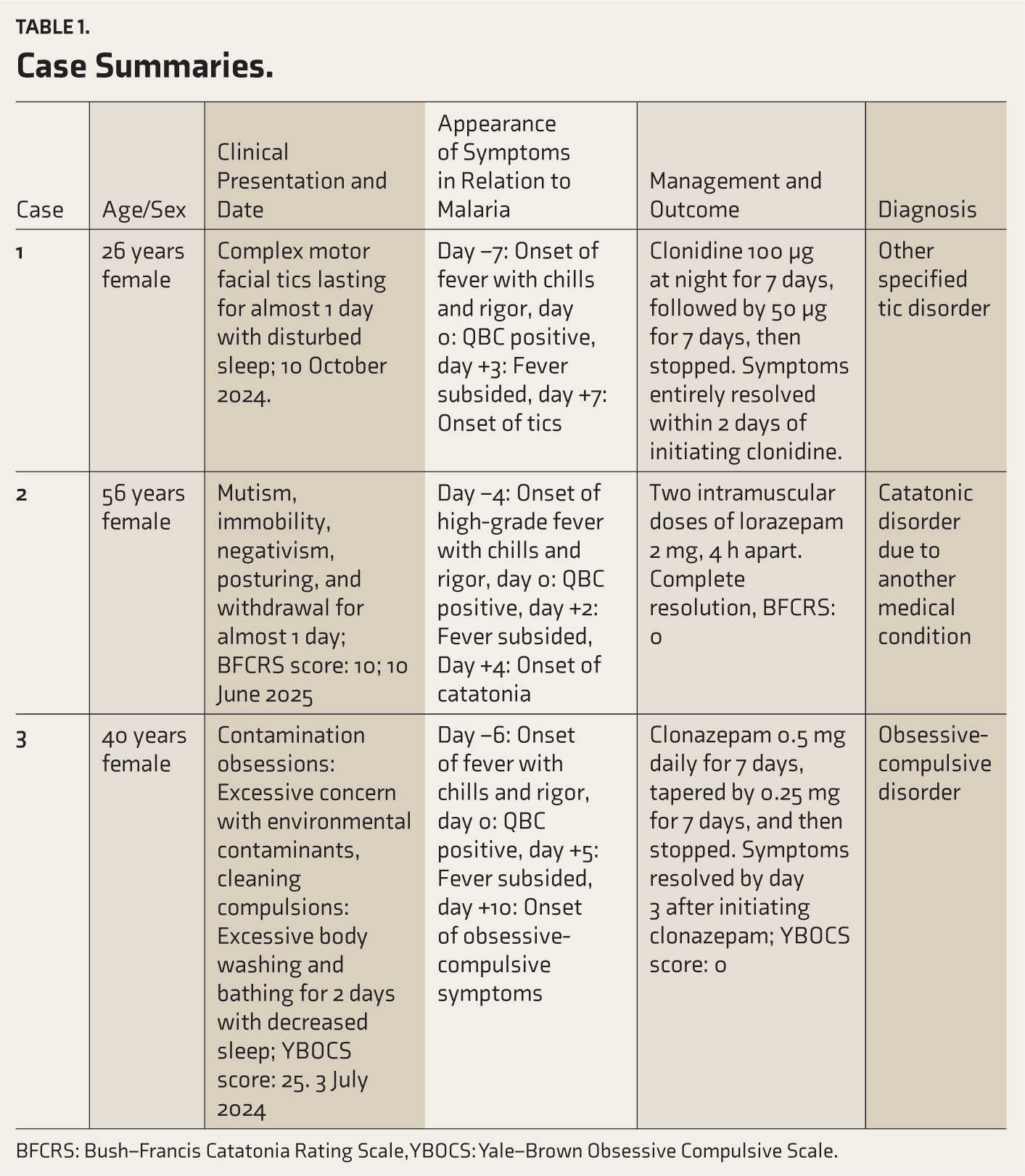
BFCRS: Bush–Francis Catatonia Rating Scale, YBOCS: Yale–Brown Obsessive Compulsive Scale.
Discussion
The pathophysiology of PMNS is poorly understood. Proposed mechanisms include the cerebral microvasculature by the parasitized red blood cells, an immune-mediated rise in pro-inflammatory cytokines, and involvement of inflammatory pathways.1,2 Further previous studies have reported white matter abnormalities and gray matter abnormalities in the cortex, thalamus, and basal ganglia. 1 Abnormalities in the basal ganglial pathways, along with overactive immune responses, have been discussed in the past in relation to the occurrence of tics and obsessive-compulsive symptoms after infections, especially streptococcal infections. 8 Also, a decrease in psychomotor activity is slowed as a response to infection, and subtypes of depression, such as atypical depression and melancholic depression, where psychomotor activity is affected, are associated with raised pro-inflammatory markers. 9 Tics, catatonia, and obsessive-compulsive symptoms appeared after the Plasmodium falciparum malaria diagnosis, and QBCe was negative during these presentations. Given the above-discussed mechanisms and a lack of nullifying evidence regarding the in-between association, it may be hypothesized that these neuropsychiatric symptoms may have occurred secondary to Plasmodium falciparum malaria. 10 There is also a possibility of the neuropsychiatric symptoms arising from artemether, lumefantrine, and primaquine use. One study previously reported dystonia following its use, 11 and another reported akathisia following interaction between artemether-lumefantrine, ciprofloxacin, and risperidone. 12 However, no study in the past has specifically mentioned neuropsychiatric symptoms in our case report after artemether-lumefantrine use. The mean symptom-free period between malaria diagnosis and the onset of PMNS was 15 days, but it can be as short as 4 days. 1 In our cases, the symptom-free period ranged from 1 to 4 days. Clonidine has been effective in the past for tics with doses ranging from 0.3 to 0.5 mg per day. 13 In our patient with tics, clonidine was used at 0.1 mg for 7 days and then tapered and stopped successfully. Clonidine was preferred, as the patient opted for a non-benzodiazepine drug and a non-antipsychotic drug, and it was available in our hospital pharmacy. Lorazepam has been used as a recognized treatment for catatonia, 9 and in our patient with catatonia, 4 mg of lorazepam was helpful. Clonazepam was beneficial in obsessive-compulsive patients in the past. 14 In our case, clonazepam was used at 0.5 mg for 7 days and then tapered and stopped successfully.
Conclusions
Our series is limited by the absence of cerebrospinal fluid studies, advanced neuroimaging, and immunological assays, which could have provided mechanistic insights, as well as by the small sample size. Nevertheless, these cases illustrate three unusual but reversible neuropsychiatric syndromes—tics, catatonia, and obsessive-compulsive symptoms—emerging after Plasmodium falciparum malaria in patients without prior psychiatric illness. They broaden the spectrum of PMNS and highlight the importance of awareness in endemic settings to avoid misdiagnosis and unnecessary long-term psychiatric treatment. Further studies are needed to explore underlying immune-mediated mechanisms.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Not applicable.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patients to publish this case report.
Prior Presentations
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.