
Abstract

Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT), also known as Hashimoto’s encephalopathy (HE), is an autoimmune disorder that can present with a wide range of neuropsychiatric symptoms. 1 The characteristic feature of SREAT is the dramatic response to steroids. 2 The most commonly associated neuropsychiatric symptoms are psychosis, followed by depression and dementia.1,3 There have been a few reports of SREAT-related generalized anxiety disorder, mania, conversion, and amnestic disorders.3,4 This, to our knowledge, is the first documented case of personality changes associated with SREAT.
Case Report
A 45-year-old married female was brought by her husband with nicotine use disorder 5 for 16 years and stealing behavior for 10 years. She started using nicotine in flavored chewable form, driven by its smell, and later by the kick it gave. She remained abstinent from nicotine for about five years due to its unavailability following the government-imposed ban. However, after five years, she managed to procure it. Due to increased craving for nicotine, she started stealing petty cash from her husband. Then she started stealing expensive items from friends and family, selling them, and then buying jewellery, expensive clothes, and accessories. After a few thefts, she felt guilty and confessed everything to her husband. However, she continued to steal, feeling an urge to do so. About eight years ago, she underwent infertility treatment, during which she was given de-addiction therapy. She eventually conceived through in vitro fertilization. There were no records of thyroid abnormalities in the patient, but the child had neonatal hypothyroidism. Occasionally, she was found to exhibit episodes of abnormal behaviours such as licking water and walking on four legs like a dog, and rolling on the floor, claiming to be a mentally ill person. She sometimes undressed herself and jumped on the bed to attract her husband’s attention. Husband noticed she became manipulative, self-centred, short-tempered, a habitual liar, and adamant. She was keen on grooming herself well. She was disrespectful toward her relatives, which was unlike her usual self. She was reluctant to care for her child or to handle household chores. There was one event of an impulsive drug overdose following a trivial conflict with her husband and repeated threatening behaviour. She was taken to a psychiatrist and was treated with divalproex (1,000 mg/d), fluvoxamine (80 mg/d), paroxetine (50 mg/d), and aripiprazole (5 mg/day) for an adequate trial with no response. There was no evidence of medication-related exacerbation of symptoms (Figure 1).

*Manipulative, impulsive, self-centred, short-tempered, habitual lying, and adamant.
Mental status examination revealed anxious affect, nicotine craving, an intense urge to steal, impaired personal judgment, and an insight of five. Neurological examination was within normal limits.
She was stealing valuable items, unlike kleptomania, and neither had associated tension or guilt. The acts were predominantly impulsive. There were no hyper-sexuality, hyper-religiosity, or sleep disturbances, which ruled out mania. There were no obsessive thoughts or behaviour. There was no evidence of psychotic symptoms. There was no low mood, suicidality, or aggression. The behavioural changes did not follow any stereotypy, nor were they associated with any seizure-like event, which helped exclude seizure. There was no other psychoactive substance use. It is noteworthy that her sister had a history of nicotine use, but is currently abstinent.
Investigations revealed hypothyroidism, and an ultrasound of the thyroid showed features suggestive of thyroiditis. Anti-thyroid peroxidase and anti-thyroglobulin antibodies were elevated, suggesting Hashimoto’s thyroiditis3,6 (Table 1).
Reports of Investigations.
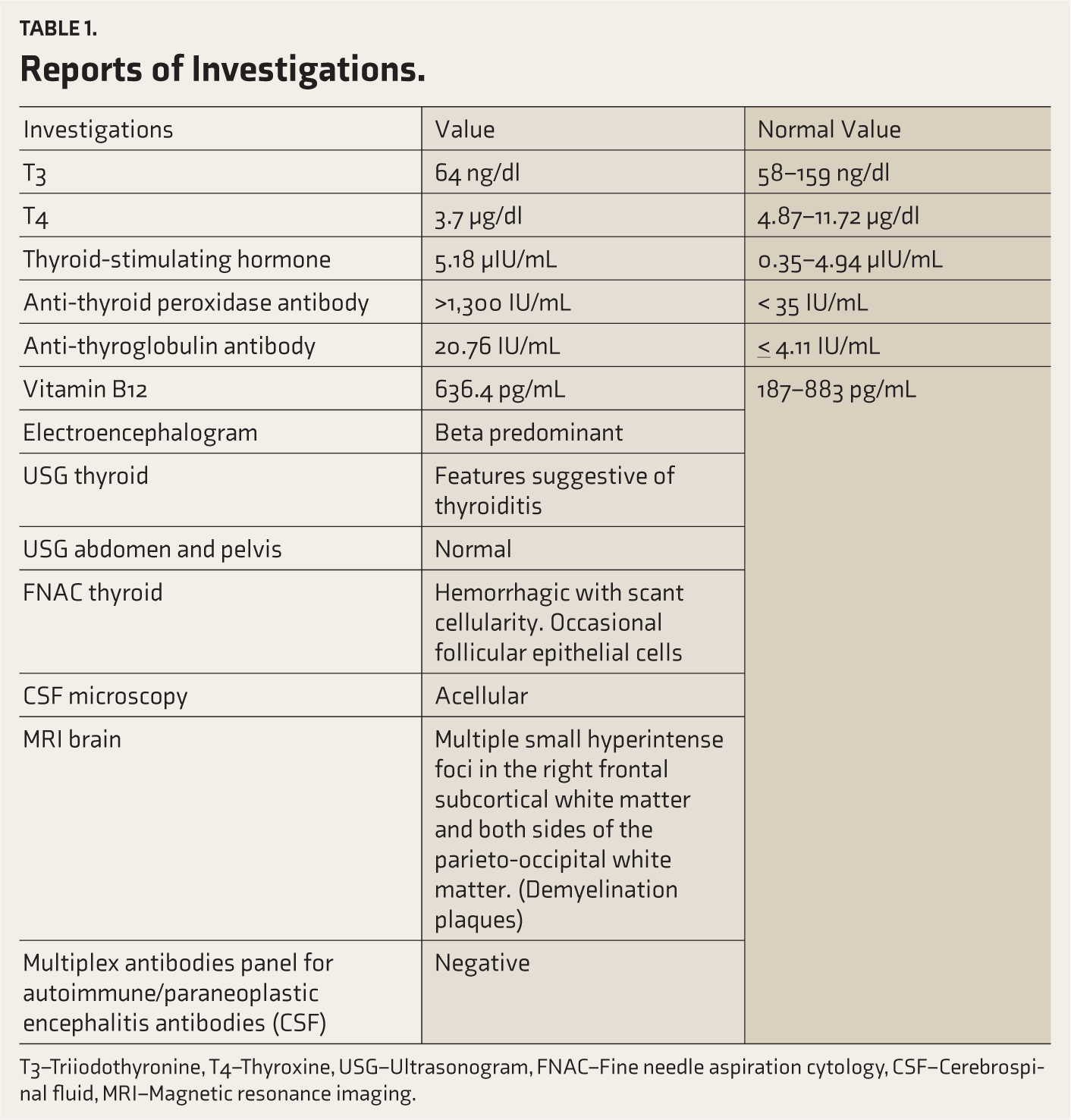
T3–Triiodothyronine, T4–Thyroxine, USG–Ultrasonogram, FNAC–Fine needle aspiration cytology, CSF–Cerebrospinal fluid, MRI–Magnetic resonance imaging.
The neurologist’s opinion was sought, and the patient was treated with parenteral steroids: A methylprednisolone 1 g infusion in 500 mL of normal saline for 5 days. The patient showed improvement in the presenting symptoms within 10 days of treatment. She was started on oral thyroxine supplements. After about one month of treatment, she denied craving for nicotine and the urge to steal. She was followed for six months, during which no previously reported behavioural changes were observed.
In conclusion, the patient exhibited personality changes compatible with SREAT/HE, supported by symptom reversal following immunotherapy and thyroid management. The predominant features were impulsivity, emotional lability, social disregard, and family neglect. As per diagnostic and statistical manual of mental disorders (DSM-5-TR), 5 personality change due to another medical condition, disinhibited and labile type, compatible with HE was made after systematically excluding primary mood, psychotic, dissociative, delirium, seizure, and substance causes.
Discussion
The absence of the presenting personality traits until the age of 35 and the resolution of symptoms after steroid therapy suggest a strong causal association with HE. Thyroid assessment is an essential element of the infertility work-up. A seemingly euthyroid state may have obscured an early diagnosis of HE. Neonatal hypothyroidism in the child reflects the presence of thyroid antibodies in the maternal circulation, suggesting chronicity of thyroiditis. Poor response to adequate trial of antipsychotics and mood stabilizers also underscores the active organicity in the background.
The HE can present with neuropsychiatric symptoms, such as seizures, involuntary movements, dementia, psychosis, and behavioural abnormalities. The course can range from acute, sub-acute, chronic, and relapsing-remitting types. 7 The hallmark of diagnosis is elevated thyroid antibody levels in serum. However, the antibody titres do not correspond to the severity of the illness. 8 It can occur in the background of hypothyroidism, euthyroid, or hyperthyroidism. 9 The presence of an euthyroid state usually settles the suspicion of underlying thyroid abnormalities. The electroencephalogram and neuroimaging can be normal or show non-specific background changes. 3
Although a single case cannot serve as strong clinical evidence, in the context of HE being a rare condition, even one clinical finding is valuable and helps identify unreported cases. However, with the current data, it is difficult to distinguish a pre-existing psychiatric condition with a superimposed, steroid-responsive encephalopathic episode. There is little evidence that long-term undiagnosed HE remains unnoticed for a long time.
Conclusions
Thyroid disorders are frequently reported to be associated with psychiatric illnesses, whereas Hashimoto’s thyroiditis is a rare entity. The presentation can be predominantly psychiatric, which hinders the early diagnosis. Considering the pronounced response to steroids, early diagnosis is the essential element for effective management. The late-onset atypical symptom with poor response to conventional management should prompt further evaluation for underlying organicity.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Appropriate Permissions from the Concerned Authorities
NA.
Data Sharing Statements
Deidentified individual participant data will not be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Statements
Ethics approval is not required for case reports according to the Institutional Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for publishing this case report.
PROSPERO/CTRI Details
NA.
Prior Presentations
This manuscript has not been presented in any scientific forum.
Registration
NA.
Simultaneous Submission to Another Journal or Resource
This manuscript has not been submitted to any other journal or resource.
Status of Your Study (for Study Protocol)
NA.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.