
Abstract
Aheterogeneous neurodevelopmental condition, autism spectrum disorder (ASD) is characterized by deficits in social communication and restrictive and repetitive behavior (RRBs). 1 The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) has provided a comprehensive diagnostic criterion of ASD, where not merely the deficiency of language competency but the overall deficits in social communication have been considered the central feature of ASD. 1 Symptoms often manifest through poor socio-emotional reciprocity, difficulty in non-verbal communication, developing and maintaining social connections, stereotypical movements, a fixed repertoire of interests, and atypical sensory needs 2 along with clinically significant internalizing and externalizing behavioral features which include anxiety, depression, somatization, aggressive emotional and behavioral outbursts, hitting others, inattention, hyperactivity, impulsivity, self-injurious behavior (SIB) and aggressive tantrums. 3 From an epidemiological point of view, the prevalence of minimally verbal (MV) individuals with ASD has been 18.5 per 1,000 children, that is, one individual out of 54 is MV.2,4 However, these MV individuals with ASD comprise a rapidly growing portion of this spectrum. 5
Many children with ASD can produce significantly fewer functional words while communicating, and these children are often identified as MV individuals with ASD. 6 Verbal skills are associated with multiple challenges across diverse domains, such as cognition, emotion, and behavior. One such important domain is emotional comprehension and appropriate channelization of emotion. 6 Articles published in the last 10–15 years show that approximately 25%–30% of individuals within the autism spectrum cannot develop functional language spoken skills and remain MV even after age five. 7 There are a few exclusive features of MV individuals with autism. Communication impairments in MV children often lead to social withdrawal. 8 They are associated with oral-motor difficulties, 9 as well as problems in adaptive behavioral skills, academic achievement, vocational success, and social relationships. 10
Recent research in this domain highlights interventions aimed at improving language acquisition, comprehension, production, and verbalization. Therefore, a sustainable intervention specifically designed to address the unexplored challenging areas involving emotional comprehension and channelization is required.
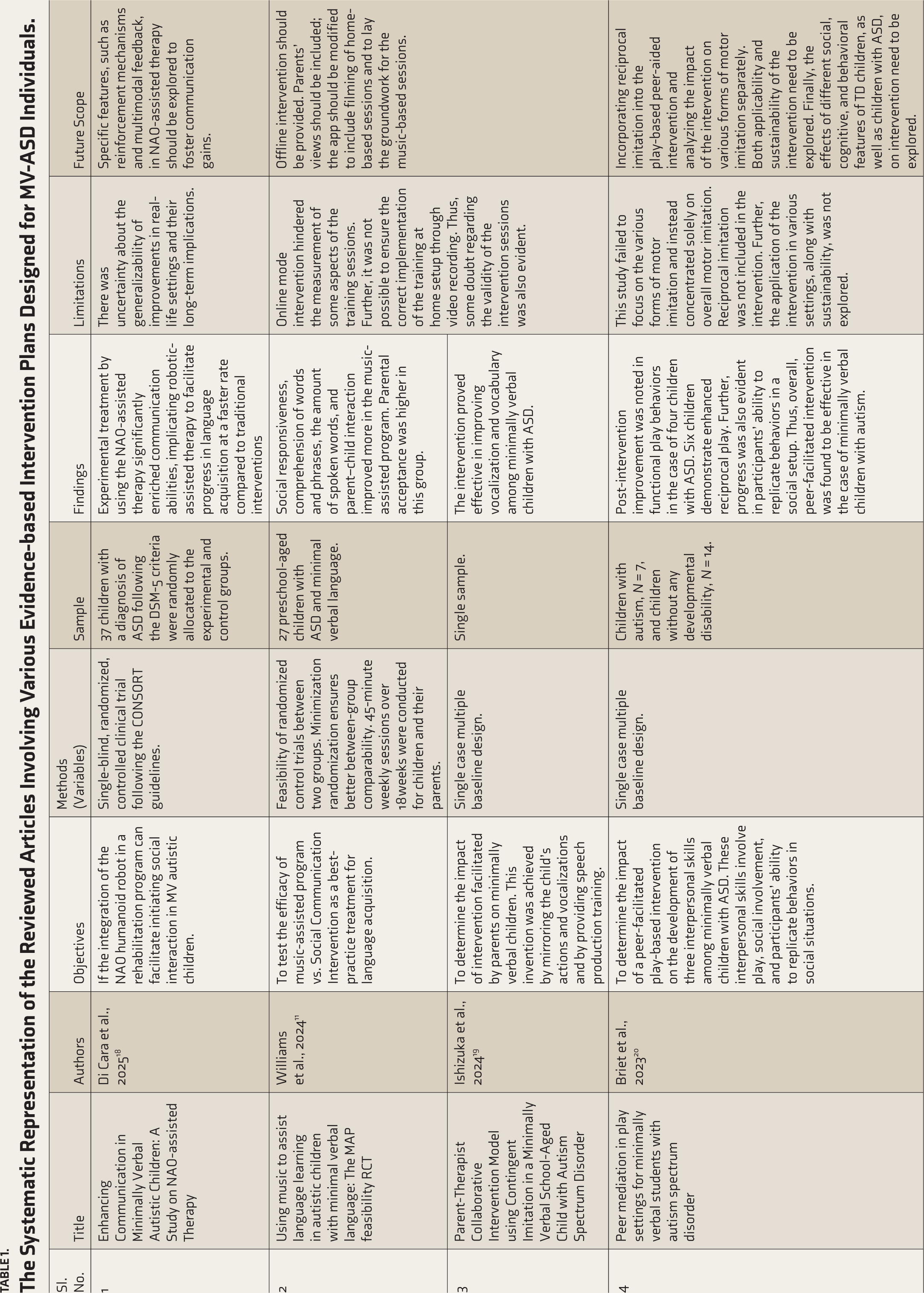
Table 1 presents a systematic review of articles describing various evidence-based intervention plans for individuals with MV-ASD.
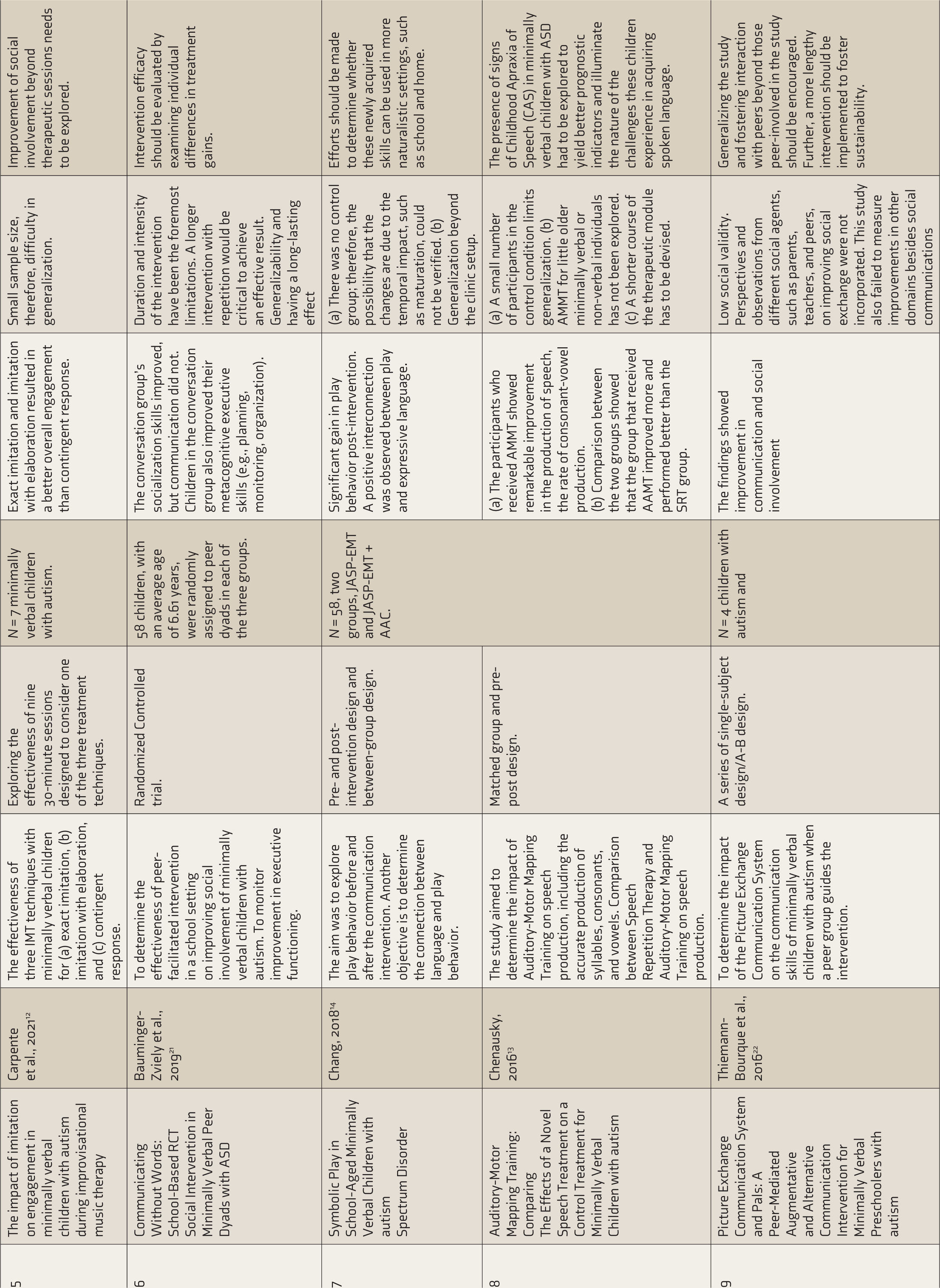
The Systematic Representation of the Reviewed Articles Involving Various Evidence-based Intervention Plans Designed for MV-ASD Individuals.
Discussion
Interventions Based on Modalities
Music-assisted Intervention
Williams et al. compared two types of interventions – music-assisted intervention and social communication intervention and found that music-guided intervention was effective in enhancing social interaction and communication. 11 In music-assisted intervention, target words were taught through music. However, both interventions were implemented at home and set up online. Thus, it was challenging to ensure the intervention was implemented correctly. Hence, the intervention’s validity is also doubtful. Another music-based intervention was employed by Carpente et al., known as Improvised Music Therapy. 12 The prime purpose of this intervention was to foster social involvement among MV-ASD through engaging them with various musical instruments. The therapist improvised music following the child’s footsteps. Despite its effectiveness, this intervention has restricted generalizability due to a small sample size.
Auditory-motor Mapping Training
Chenausky et al. implemented Auditory-Motor Mapping Training (AAMT) to promote linguistic skills in MV-ASD. 13 In this training, the auditory and motor representations of the same manual and vocal actions are jointly activated by coupling the recitation of 2-syllable target words or phrases with the beating of electronic drums using the same tunes as in the recitation. This intervention was found to be effective in enhancing the percentage of correct consonant and vowel production and refining the rate of syllable approximation. 13 However, the impact of AMMT on the older MV-ASD group was not explored in this study. Furthermore, the limited sample size restricted the generalizability of the findings.
Communication-based Intervention
Two more intervention strategies were reported by Chang et al. JASP-EMT and JASP-EET+AAC. 14 JASPER-EMT is the combination of two techniques. 14 It includes interventions on joint attention, symbolic play, engagement, and regulation. 15 along with Enhanced Milieu Teaching involving systematic prompts to facilitate speech. 16 On the other hand, JASP-EET-AAC includes a speech-producing device along with all other elements of JASP-EMT. 17 Both interventions were administered to participants in a natural setting while engaging in their preferred play-based activities. These interventions were found to be quite effective in facilitating play behavior among the MV-ASD cohort.
Intervention Involving the NAO Humanoid Robot
Di Cara et al. introduced an experimental treatment using NAO-assisted therapy with the Humanoid Robot NAO in a Single-blind, randomized, controlled clinical trial involving 37 individuals with ASD, following the CONSORT guidelines. 18 The intervention significantly enriched communication abilities, suggesting that robotic-assisted therapy can facilitate faster language acquisition than traditional interventions. However, there was uncertainty about the generalizability and long-term implications of individuals’ independent functioning.
Interventions Involving Varied Stakeholders
Ishizuka et al. designed parent-therapist collaborative interventions to enhance speech production in the MV-ASD cohort and found them quite effective. 19 Likewise, several peer-mediated interventions are also reported in this review. One such peer-meditated play-based intervention was employed by Briet et al. to enhance social reciprocity among individuals with MV-ASD. 20 First, peers were educated on various techniques for communicating with children with ASD, and subsequently, they were encouraged to play with the children using those techniques. Another such peer-involved intervention was reported in the study conducted by Bauminger-Zviely et al. 21 However, this was implemented in a school setting. A notable aspect of this intervention was its emphasis on enhancing executive functioning and social involvement. Thiemann-Bourque et al. also incorporated peers in picture exchange communication interventions. 22 In this intervention, peers assumed an active role in fostering social interaction through picture symbols among MV-ASD under the supervision of experts. All these facilitated interventions are identified as equally fruitful in promoting social interaction, engagement, and executive functioning of the individuals with MV-ASD. Thus, based on this observation, it can be assumed that involving different stakeholders in therapeutic sessions yields quite fruitful outcomes. However, these interventions have several limitations. First, the sustainability and generalizability of these interventions are questionable due to the small sample size. Besides, these interventions failed to incorporate the perspectives and observations of different stakeholders such as parents, peers, and teachers. Finally, apart from social communication, these interventions ignored improvements in other domains.
Limitations of Existing Research
Interventions explored to date have focused on the MV group, primarily on improving social communication skills, reciprocal interaction, and maladaptive behavioral manifestations. In addition, these interventions have drawbacks, such as their online delivery mode, which limits their practical implementation, and confusion about their applicability beyond therapeutic sessions. Further, the scope of these interventions has been restricted to communication domains. Apart from this, the usage of RRBs, internalizing-externalizing manifestations, and various emotional and cognitive aspects are not within the scope of these interventions. Additionally, the sustainability of the intervention even after the follow-up sessions was in question. Therefore, a sustainable intervention module is required to address this reported gap.
Future Recommendations
Therefore, a personalized treatment plan is suggested for addressing the unique hindrances that MV individuals with ASD face in comprehending and responding to emotional experiences. 6 An eclectic intervention plan involving theoretical, evidence-based approaches such as applied behavior analysis and the functional communication system, as well as experiential approaches such as projective art therapy, play-based intervention, and occupational approaches, is highly recommended. Further, a multi-sensory approach involving tactile, physical movements, and so on to alleviate linguistic burden should be incorporated. This eclectic intervention approach will include a dyadic interaction pattern in some sessions, with the parent or therapist, or a group setup, where play sessions will be encouraged among peer groups. Further, this intervention should become a part of their everyday curriculum. The strength of such an intervention lies in its design: the involvement of different modalities in separate sessions, with immediate family members, peer group, teachers, and other caregivers participating in dyadic or group modes. This may provide an opportunity to orient stakeholders on how to follow up on the techniques in everyday scenarios. Thus, sustainability can be ensured. This would be the first, to the best of our knowledge, involving a multimodal approach.
Conclusions
Our article highlights the urgency of developing a composition of intervention plans drawn from comprehensive approaches, such as applied behavior analysis, creative art interventions, play therapy, and augmentative and alternative communication modes, directed toward enhancing emotion comprehension and its channelization exclusively for individuals with MV-ASD. Therefore, we highly recommend a personalized, sustainable, and multimodal intervention plan for the MV-ASD.
Data Sharing Statements
Our article does not deal with any primary data. Hence, data sharing is not applicable.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The authors communicated the research work officially to the institutional review committee. The committee waived off the need for consent. Name of the Institutional Ethics Committee/ Independent Review Board: NA. Approval Ref. No: NA. Date: NA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
The article does not entail any active participation of human participants. Therefore, informed consent from participants is not required.
Prior Presentations
NA.
PROSPERO/CTRI Details
NA.
Registration
Not applicable as the article is not an experimental or clinical trial. Trial registry name: NA. URL: NA. Registration number: NA.
Simultaneous Submission to Another Journal or Resource
Not submitted to any journal.