
Abstract

Dear Editor,
Tobacco use remains a leading cause of preventable death in India, with 38%–42% of adult men and 8.9%–14.2% of adult women using tobacco, 1 resulting in 1.35 million deaths annually and costs of ₹ 1,773.4 billion. 2 Despite effective comprehensive tobacco cessation services, including 612 district tobacco cessation centers, mCessation services (011-22901701), and the National Tobacco Quitline Services ([NTQLS]: 1800112356) established under the National Tobacco Control Program (NTCP),3–6 significant awareness gaps persist. 7 Evidence demonstrates that hospital-initiated tobacco cessation programs can be an effective intervention strategy by reducing all-cause readmissions by 11.7% and mortality by 6.0% at one year. 8 This awareness deficit represents a significant barrier to accessing evidence-based cessation services, particularly in hospitals where brief interventions can be delivered effectively. Despite the proven effectiveness of interventions and the availability of infrastructure, no systematic data exist on awareness levels among patients and providers at district hospitals in India.
This study, conducted from 2020 to 2022, examined the awareness of tobacco cessation services among patients and healthcare providers across four district hospitals in Karnataka (Mandya, Chikkamagaluru, Vijayapura, and Bidar), which have dedicated tobacco cessation centers. 9 The participants included patients, doctors, and nurses in the following proportions (80:10:10): patients (n = 406), doctors (n = 50), and nurses (n = 52). Patients included individuals visiting outpatient departments across various specialties for routine consultations, follow-up visits, or health screening. Both tobacco users and non-users were included in this survey study. A bilingual (English–Kannada) semi-structured questionnaire was developed by subject experts using Google Forms. 10 Due to the absence of validated instruments, the questionnaire was designed and pilot-tested for content validity and usability. The instrument comprised eight sections with conditional skip logic, focusing on awareness of tobacco cessation facilities, knowledge of government programs (mCessation and NTQLS), current tobacco use patterns, and preferences for cessation support. Data collection was conducted through trained personnel using structured face-to-face interviews. Statistical analysis employed chi-square tests and logistic regression using Statistical Package for the Social Sciences (SPSS) version 29.0.2, with significance set at p < .05.
Overall, 19.1% (n = 97) of all respondents reported being aware of a tobacco cessation facility at their hospital. When examined by respondent type, awareness was significantly lower among patients, with only 7.8% (n = 32 out of 406 patients) aware of such facilities. Less than 2% of all respondents were aware of telephonic cessation services (mCessation and Quitline).
Healthcare providers (doctors and nurses) reported significantly higher awareness of “existing Tobacco Cessation Center in their hospital,” “mCessation,” and “NTQLS” compared to patients (Table 1). Among the 11 participants aware of the NTQLS, only two (18.2%) could correctly identify the phone number, with advertising as their primary source of information. Overall, 82.1% replied that they were unaware of any “cessation services.”
The Awareness of the Tobacco Cessation Services from the Four Districts of Karnataka (
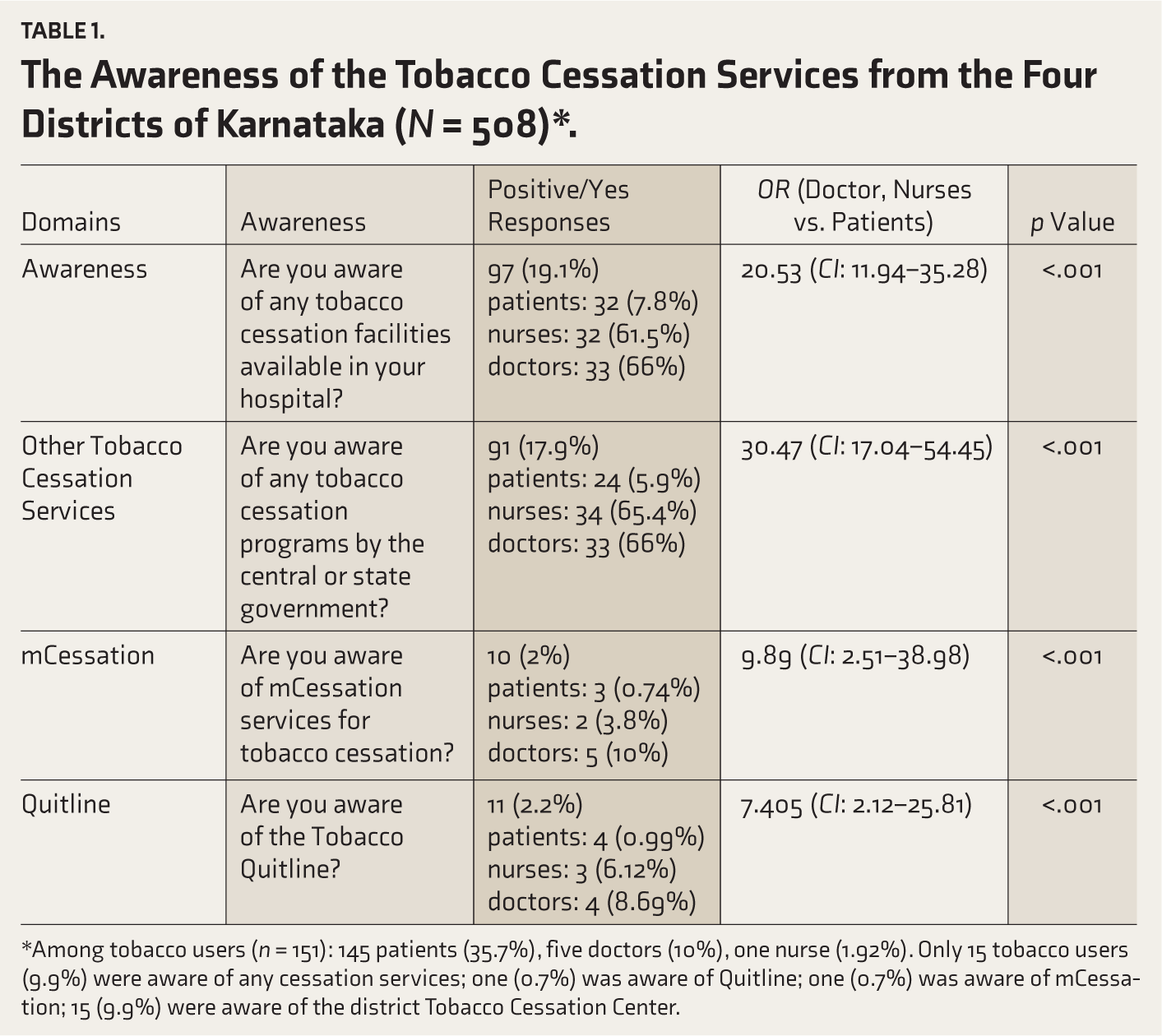
*Among tobacco users (n = 151): 145 patients (35.7%), five doctors (10%), one nurse (1.92%). Only 15 tobacco users (9.9%) were aware of any cessation services; one (0.7%) was aware of Quitline; one (0.7%) was aware of mCessation; 15 (9.9%) were aware of the district Tobacco Cessation Center.
One in three interviewed (29.7%, n = 151) for this study is an active tobacco user (used tobacco in the last six months), comprising 145 patients (35.7% of all patients), five doctors (10% of all doctors), and one nurse (1.92% of all nurses). Among active tobacco users, patients were 30.22 times more likely to be unaware of cessation services compared to healthcare providers (p < .001). Only 15 tobacco users (9.9%) were aware of any cessation services in their hospital, only one tobacco user (0.7%) was aware of Quitline services, and one tobacco user (0.7%) was aware of mCessation. Despite this awareness gap, tobacco users expressed a preference for receiving cessation support from government hospitals.
Discussion
In line with previous studies, 7 the current survey supported a significant lack of awareness of the existing tobacco cessation services among patients visiting the district hospitals, including tobacco users.
The 7.8% awareness rate among patients contrasts sharply with international studies, which show awareness rates exceeding 60% in healthcare settings. 11 A study in Saudi Arabia reported that 60% and 26% of tobacco users were aware of fixed Smoking Cessation Clinics (SCCs) and mobile SCCs, respectively. 11 Less than 1% of patients knew either mCessation or Quitline services. This holds for both tobacco users and nonusers. One possible reason is that the services are available only at the district hospital and not at health centers. 12
The near-absence of awareness regarding telephonic services (2% vs. >50% in other studies,13,14 highlights missed opportunities for extending cessation support beyond hospital boundaries. The physician’s awareness of Quitline in the USA was 23.3%, 15 almost three times that of the current study (8.69%).
However, limitations such as a small sample size, the cross-sectional nature of the study, and the fact that it was conducted only in four districts may limit the generalizability of the findings.
Conclusions
Given the substantial burden of tobacco-related diseases and the significant awareness gaps identified in our study, there is a need to implement comprehensive, multi-layer interventions that address both service delivery and awareness barriers. 16 This requires (a) integration with national programs, including the National Tuberculosis Elimination Program, the National Program for Prevention and Control of NCDs, and the National Mental Health Programs, as well as Health and Wellness Centers, to leverage existing infrastructure and maximize resource utilization. Evidence demonstrates that integrating tobacco cessation interventions into existing NCD clinics is feasible and implementable, 17 alongside (b) targeted awareness campaigns designed explicitly for rural populations, incorporating culturally sensitive approaches that have proven effective, 18 and (c) standardized documentation of tobacco use status in patient records as a vital sign can enable regular screening and intervention by health care professionals. These approaches can help the current fragmented tobacco control program become a more cohesive system.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
Thanks to Mr Vishnu Prasad and Mr Pradeep Kumar CB, Research Assistants (NTCP), for data collection.
Anonymity
There is no name of the organization or any identifier in the manuscript.
Data Sharing Statements
Not required as it is not a trial.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
Grammarly and Claude (Anthropic) were used for grammar checking and enhancing sentence clarity, respectively. The data collections, content, table, and text are contributions by the authors. The authors assume full responsibility for all content, including parts generated by the AI tools.
Ethics Committee Approval
NIMHANS/EC (BEH.SC.DIV.) 19th Meeting/2019 Date: 02 July 2019.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The State Anti-Tobacco Cell, NTCP, Department of Health and Family Welfare, Government of Karnataka, India, funded this study.
Prior Presentation at a Meeting
No.
Simultaneous Submission to Another Journal or Resource
No.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.