
Abstract
Catatonia is a complex neuropsychiatric syndrome seen across various psychiatric, neurological, and medical disorders. According to the Diagnostic and Statistical Manual Fifth Edition, Text Revision (DSM-5-TR), it is defined by the presence of three or more of the 12 mentioned features: Stupor, catalepsy, waxy flexibility, mutism, negativism, posturing, mannerism, stereotypy, agitation, grimacing, echolalia, and echopraxia. 1 Although specific features, such as autonomic dysregulation, delirium, grasp reflex, excitement, history of seizures, or other neurological conditions, raise suspicion of an organic etiology, the absence of these features cannot completely rule out organicity. 2 The International Classification of Diseases-11 (ICD-11) categorizes cases of catatonia resulting from a medical condition as “secondary catatonia syndrome.” 3 In fact, the coexistence of both medical and psychiatric conditions is not uncommon.4,5
Given varied presentation and etiology, it is often recognized late in medical settings, leading to a delay in treatment initiation. In such cases of long-standing catatonia, response to benzodiazepines is not as robust or rapid as that of those with acute catatonia, and electroconvulsive therapy (ECT) is used as the next resort. 6 However, if there is a contraindication or intolerance to ECT, a treatment dilemma arises with no clear consensus on the next steps in management. In light of this, we have highlighted three cases of coexisting medical and psychiatric conditions and one case of benzodiazepine withdrawal catatonia, each posing diagnostic challenges, limiting therapeutic options, and making it difficult to treat. Figure 1 depicts the symptom course and management approach of these cases in a general hospital setting.
Flow Diagram Representing Symptom Course and Management.

Case 1
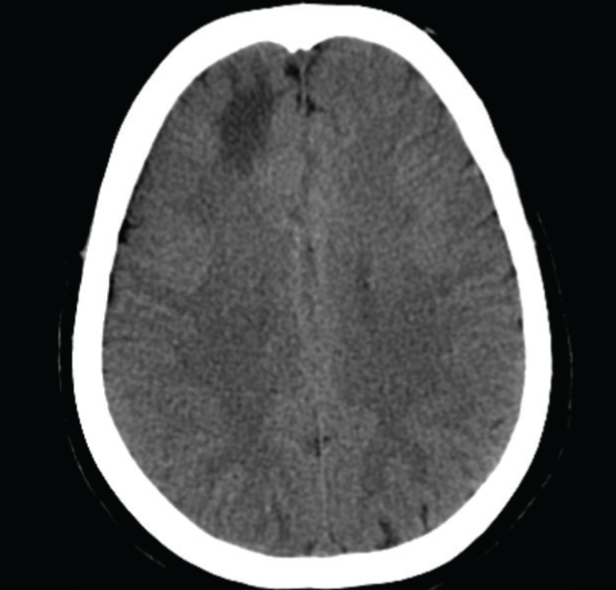
A 35-year-old female, with nil significant family history, previously on conservative management of migraine and one episode of acute transient psychotic disorder (ATPD) three years ago lasting for two months, presented with an abrupt onset of symptoms for one week of overtalkativeness, agitation, irritability, and frequent headaches, followed by three days of mutism, withdrawal, negativism, and grasp reflex. The initial score on the Bush Francis Catatonia Rating Scale (BFCRS) was 24, with a positive lorazepam challenge test (LCT). However, the patient did not show significant improvement with oral lorazepam 20 mg for two weeks. Supportive care, including Ryle’s tube feeding and bladder catheterization, was provided. Inability to titrate benzodiazepines further due to sedation and positive grasp reflex with a background of headaches raised a suspicion of underlying organicity. Non-contrast computed tomography (CT) brain revealed a hypodense region in the right frontal area, with follow-up CT venogram confirming partial anterior cortical venous thrombosis (CVT) (Figure 2). Diagnosis of secondary catatonia syndrome was made as per ICD-11. The medical team adopted a conservative approach after extensively ruling out possible systemic causes and initiated her on prophylactic enoxaparin 120 mg subcutaneous and oral warfarin 5–10 mg. After five days, she showed gradual and sustained improvement in catatonia. However, resolution of catatonia unmasked symptoms of fearfulness and auditory hallucinations, which were managed with olanzapine 15 mg.
CT Venogram Brain Findings. A Hypodense Region was Noticed in the Right Frontal Lobe with Partial Filling.
Case 2
A 27-year-old unmarried male from a lower socio-economic status, with no relevant past or family history, presented with a 10-day history of acute onset of neuropsychiatric symptoms such as confusion, irritability, and disorientation, along with constitutional symptoms of initial somnolence followed by decreased sleep. These symptoms were followed by fleeting nihilistic ideas, mutism, withdrawal, and immobility. He was admitted to the medicine ward with suspicion of meningitis and started empirically on ceftriaxone and doxycycline. Although cerebrospinal fluid analysis was within normal limits, the magnetic resonance imaging (MRI) of the brain revealed hypertrophic pachymeningitis. Since the patient did not respond to the complete antibiotic course, and no clear underlying etiology could be established, a diagnosis of idiopathic hypertrophic pachymeningitis was made. At this stage, after two weeks of initial presentation, he was referred to psychiatry. The patient showed a significant response to LCT. He showed a partial response to lorazepam (up to 24 mg), with poor oral intake and self-care, which was concerning. Thus, ECT was initiated, and after a course of six sessions, the BFCRS score dropped to zero. On mental status examination, fearfulness and hallucinatory behavior were noted. With an additional diagnosis of ATPD along with catatonia associated with another mental disorder, he was given olanzapine up to 15 mg. The patient was continued on maintenance ECT (12 sessions) and olanzapine 15 mg with a successful taper of lorazepam up to 10 mg with no recurrence of symptoms.
Case 3
A 33-year-old married female presented with a history of multiple episodes of ATPD. She experienced her first episode one week postpartum in 2010, marked by sleep disturbances, hallucinatory behavior, and persecutory delusions. Achieving remission after three months of treatment, she remained well without medication for eight years. Subsequent episodes in 2018, 2019, and 2023 were characterized by symptoms of mutism, staring, rigidity, negativism, and withdrawal with brief periods of persecutory and referential delusions before the onset of catatonic symptoms. During these years, she responded well to lorazepam and olanzapine. She would default on medications whenever she was symptomatically better, leading to recurrence. She had never received ECT before. Her current presentation involved acute symptoms of 13 days of mutism, posturing, withdrawal, negativism, staring, rigidity, and persecutory ideas precipitated by the abrupt self-taper of lorazepam dosage from 20 mg to 8 mg due to increased sedation. Though she had a positive LCT, she did not respond adequately with increasing doses of lorazepam (20–24 mg). She was diagnosed with catatonia associated with another mental disorder as per ICD-11. ECT was initiated, and complete resolution of catatonia was seen after eight sessions. Psychotic symptoms resolved subsequently with olanzapine 15 mg. She was discharged and continued on maintenance ECT (15 sessions). Lorazepam was successfully tapered off in outpatient follow-up visits with no further symptom recurrence.
Case 4
A 45-year-old female, with a six-year history of continuous psychiatric illness characterized by irritability, delusions of persecution, delusions of infidelity, and hallucinatory behavior, has been relatively well without any psychotropic medication for the last six months, and presented with a gradual onset of immobility, mutism, staring, rigidity, withdrawal, and sleep disturbances over the previous two months. Upon presentation, she was incidentally diagnosed with type 2 diabetes mellitus with diabetic ketoacidosis and hyponatremia, following which she was admitted to the medicine ward. Other blood investigations, including creatine phosphokinase, were within normal limits. However, even after medical stabilization, her condition did not improve, warranting a psychiatric referral. Upon examination by the psychiatric team, she was found to be oriented, responding minimally to commands in whispers, with compromised oral intake and self-care. Her BFCRS score was 20 with an inconclusive LCT. Due to past psychiatric history, a provisional diagnosis of schizophrenia was made, and she was transferred into psychiatric care. She had global left ventricular hypokinesia with an ejection fraction of 40%–45% limiting treatment options. With lorazepam 20 mg, her BFCRS score reduced to 10. However, due to persistent symptoms of asymmetrical rigidity with upward gaze deficits, an MRI of the brain was performed. A chronic infarct in the left inferior frontal gyrus with midbrain atrophy was noted. A diagnosis of progressive supranuclear palsy (PSP) was made in consultation with the neurology team, and levodopa–carbidopa (300 + 30 mg) was started. The final psychiatric diagnosis was kept as secondary catatonia syndrome. Antipsychotics were not started as psychotic symptoms were under remission. With a combination of levodopa and carbidopa, along with lorazepam, the patient demonstrated sustained improvement in her symptoms, achieving a BFCRS score of zero over a one-month follow-up period. There was no re-emergence of psychosis.
Discussion
Catatonia, once exclusively linked to schizophrenia, is now recognized to be an independent disorder that can be associated with other mental disorders, substances, or medications, secondary to medical conditions, and unspecified according to ICD-11. 3 DSM-5-TR also recognizes similar changes wherein catatonia can occur secondary to other mental, medical, or unspecified conditions. 3 Identifying medical and psychiatric conditions associated with catatonia often relies on clinical judgments. Evidence suggests that approximately 20% of unselected catatonia cases and over 50% in acute medical settings have an associated medical disorder, rising to nearly 80% in older patients. 2 In a systematic review, inflammatory brain disorders, especially encephalitis, were the most common category (28.8%). 2 Neural injury, toxins or medications, structural brain pathology, epilepsy, and miscellaneous disorders are other common medical conditions associated with catatonia.
From a neurobiological perspective, catatonia reflects dysfunction in cortical-subcortical motor and affective networks. A systematic review on brain imaging of catatonic patients revealed hypoactivity, particularly in the orbitofrontal cortex, supplementary motor area, parietal cortex, and basal ganglia. 7 At the neurotransmitter level, reduced γ-aminobutyric acid (GABA) and dopaminergic activity contribute to motor inhibition, explaining the response to benzodiazepines. Glutamatergic hyperactivity may further destabilize cortico-striatal circuits, with improvement often seen with N-methyl-D-aspartate (NMDA) antagonists such as memantine. 8 Together, these findings support the view that catatonia reflects disruption across interconnected neurotransmitter systems rather than any single deficit. Moreover, neuroinflammatory and immune-mediated processes observed in conditions such as encephalitis and hypertrophic pachymeningitis can disrupt cortico-striato-thalamo-cortical networks through cytokine release, blood–brain barrier dysfunction, and antibody-mediatedeffects, thereby precipitating catatonic symptoms. 9
According to Bradford Hill’s criteria, temporality, biological plausibility, and consistency must be carefully scrutinized to decipher any potential causation. We have described four cases of catatonia associated with CVT, hypertrophic meningitis, benzodiazepine withdrawal, and PSP. In all our cases, the medical or psychiatric condition clearly preceded the onset of catatonia.
Catatonia associated with CVT has been described in earlier reports. 10 Hypometabolism in the basal ganglia, along with hypoperfusion in frontal, parietal, and temporal lobes, has been postulated as the underlying pathophysiology, providing a biological explanation for catatonia in the context of CVT. Convergence of temporality, plausibility, and consistency supports attributing catatonia to CVT in this case. However, unlike other cases reported in literature, our patient reported under Case 1 did not have other structural brain lesions such as convulsions, infarction, or hemorrhage.
To the best of the authors’ knowledge, only one case of catatonia caused by recurrent idiopathic hypertrophic pachymeningitis has been documented, in which a decrease in regional cerebral blood flow was observed in the orbitofrontal and anterior cingulate cortex, accompanied by a delta wave focus in the electroencephalogram. This patient required high-dose steroids for symptom resolution in addition to benzodiazepines, which might be due to the long-standing nature of the medical illness and older age. 11 In contrast, our patient, described in Case 2, showed significant improvement with lorazepam and ECT, without the need for immunotherapy, highlighting novel clinical aspects not previously described.
Catatonia, though uncommon, has been reported in the context of benzodiazepine withdrawal in both substance users and patients with psychosis. This is thought to result from dysregulation of multiple neurotransmitters, including GABA, dopamine, glutamate, and serotonin. Abrupt discontinuation of benzodiazepines can lead to relative GABA deficiency, destabilizing neural circuits that regulate motor and behavioral functions, precipitating catatonic symptoms in vulnerable individuals.12,13 Case 3 illustrates benzodiazepine withdrawal catatonia resistant to high-dose lorazepam, necessitating ECT. Notably, in some patients, response to ECT may take longer than expected, highlighting the importance of individualized treatment planning and the need for compliance in such patients with recurrent catatonia.
In a retrospective study of 12 patients with catatonia in the neurology emergency, at least six had catatonia due to a general medical condition, two of them being PSP. 14 Although typical PSP presents with axial rigidity, gait instability, falls, and eye movement abnormalities, there are other less recognized variants that add to diagnostic confusion. In Case 4, MRI findings and eye signs aided diagnosis. In a similar case report, authors have discussed poor response to benzodiazepines and ECT in such cases. 15 Symptomatic treatments with L-dopa, dopamine agonists, and benztropine have been suggested in various combinations, which proved effective in our case as well.
Derived from prior descriptions of treatment-refractory catatonia and our clinical experience, we propose a preliminary framework for “difficult to treat catatonia.”16,17 This includes any case where standard treatment is complicated by one or more of the following: (a) Delayed recognition, (b) partial or poor response to benzodiazepines, (c) contraindication or difficulty in initiating ECT, and/or (d) co-morbid medical condition. This framework is intended as a clinical tool to aid conceptualization and management, rather than a validated diagnostic construct. Drawing an analogy with a similar concept of difficult to treat depression, which is a well-established condition, describing “a kind of illness that continues to cause significant burden despite usual treatment efforts due to non-adherence, treatment delays, past life experiences, current social circumstances, and comorbidities,” we aim to provide a clinical approach to conceptualize similar challenges in treating catatonia. 18
Although such “difficult to treat” cases often bring unique challenges, the best approach is to carefully delineate the cause through a thorough diagnostic workup with a high index of suspicion. Irrespective of cause, benzodiazepines and/or ECT remain the mainstay of management. 19 Two of our cases required ECT due to inadequate lorazepam response consistent with evidence. Treatment of catatonia involves addressing two distinct aspects: Specific interventions for catatonia itself and treatment for the underlying disorder(s) when identified. While either approach may be practical, there are instances where success is achieved through the use of the other or a combination of both. 19 Additionally, attention must be directed toward preventing and managing medical complications associated with catatonia. Research indicates that patients with shorter durations of illness are more likely to exhibit a favorable treatment response. 20 As three of our patients were initially managed in the medicine ward, where catatonia was overshadowed by medical issues such as CVT, pachymeningitis, and metabolic imbalances, it resulted in delayed referral and treatment. Additionally, the presence of issues related to medical conditions in two cases, such as the need for anticoagulation and issues with heart function, restricted our treatment options. These circumstances emphasize challenges and complexities involved in recognizing and managing catatonia outside of specialized psychiatric facilities, where maintaining a strong clinical suspicion, early referral, and collaboration is crucial, with initiation of treatment at the earliest. Lastly, in all of our patients, successful remission was achieved only after treating the underlying condition along with catatonia itself.
Conclusions
Considering the abundance of evidence and probable rationale that catatonia exhibits reduced responsiveness to treatment over time, there is a need for prompt identification and management. The cases reported above highlight the crucial role of psychiatric consultation services in the early detection and treatment of catatonia in medical settings. Implementing strategies to enhance recognition and treatment of catatonia is essential for improving clinical outcomes in general hospital patients experiencing this reversible syndrome.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Copyright Declaration
The authors declare that they have not used any tables, figures, instruments, rating scales, or other copyrighted material.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
As per the institute’s ethical committee policy, ethical approval is not required for this case series as the data is retrospective and anonymized.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors certify that they have obtained all necessary written patient-informed consent forms. In the form, the patients have given consent for the use of images and other clinical information to be reported in the journal. The patients understand that every effort will be made to conceal their identity and maintain anonymity.
Prior Presentations
The article was presented at the 39th Annual National Conference of the Indian Psychiatric Society Tamilnadu chapter in Coimbatore from 27 to 28 July 2024.
Simultaneous Submission to Another Journal or Resource
The case series being submitted has not been published, simultaneously submitted, or already accepted for publication elsewhere.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.