
Abstract
Response rates to adequate trials of antipsychotics in schizophrenia range from 20% to 68%. 1 Around 30% of patients with schizophrenia have inadequate response to various antipsychotic trials, and clozapine is considered effective in treatment-resistant schizophrenia (TRS). 2 Despite proven efficacy in TRS, it remains underutilized due to various factors such as lack of prescribing experience, the need for monitoring, and the perceived burden of adverse effects. 3 With regards to the latter, weight gain, insulin resistance, and alteration in lipid metabolism are of primary concern. 4 Clozapine and olanzapine have been associated with higher weight gain compared to all other atypical antipsychotics. 5 In contrast, weight loss has been rarely reported with clozapine. We aim to report the clinical details of patients with TRS who experienced weight loss with clozapine.
Case Series
This case series is from a tertiary care hospital with a general hospital psychiatry setting. All patients who were identified to have clinically significant weight loss associated with clozapine in the past 10 years (between 2013 and 2023) were included. Clinically significant weight loss was defined as unintentional loss of more than 5% body weight over a period of 6–12 months. 6 Socio-demographic details, psychiatric diagnoses, clinical features, course of the symptoms, medical comorbidities, biochemical and metabolic parameters, treatment details, and outcomes were extracted using a semi-structured proforma through a retrospective file review.
We identified six patients (three male and three female) with a mean age of 39.3 years (SD 7.3) during the study period who had clinically significant weight loss while on clozapine. All patients in our report had a diagnosis of schizophrenia along with various medical comorbidities. The clinical details are summarized in Table 1. The mean dose of clozapine was 520 mg (SD 192; range, 200–700 mg). Serum clozapine assays were not available. All patients were also on augmentation with divalproate sodium. Weight loss ranged from 10.6% to 45% of body weight, with a median loss of 10 kg interquartile range (IQR 17). In five patients, weight loss was noted within a year of clozapine initiation. One patient had weight loss after nine years of clozapine trial. In all these patients, the clinically significant weight loss was attributed to clozapine after a thorough panel of investigations to rule out other causes, including complete hemogram, thyroid and endocrine profile, blood glucose levels, renal functions, HIV serology, upper gastrointestinal endoscopy, colonoscopy, and computed tomography of the abdomen to rule out malignancy. There was no change in the dietary pattern or changes in the physical activity levels before the weight loss. All patients except one had a poor response to clozapine (serial number 6 in Table 1). The patient who responded to clozapine had improvement in negative symptoms; however, there were no changes in tobacco use patterns after introducing clozapine. Stopping clozapine or dose reduction resulted in weight gain in four patients.
One patient was found to have esophageal candidiasis and continued to have weight loss even after successful management of the same (serial number 1 in Table 1). One patient experienced nausea and vomiting secondary to clozapine, which interfered with food intake and could have thereby contributed to the weight loss (serial number 5 in Table 1). However, no structural gastrointestinal abnormality was noted in this patient’s imaging. In three patients who had comorbid type 2 diabetes mellitus (T2DM), there was stable glycaemic control, and there was no change in the dose of oral hypoglycemic agent (OHA) temporally coinciding with the observed weight loss. There was an improvement in glycaemic control in all of these patients during the weight loss period, and one of them achieved remission and no longer required OHA.
The Clinical Profile of Patients with Clozapine-associated Significant Weight Loss.
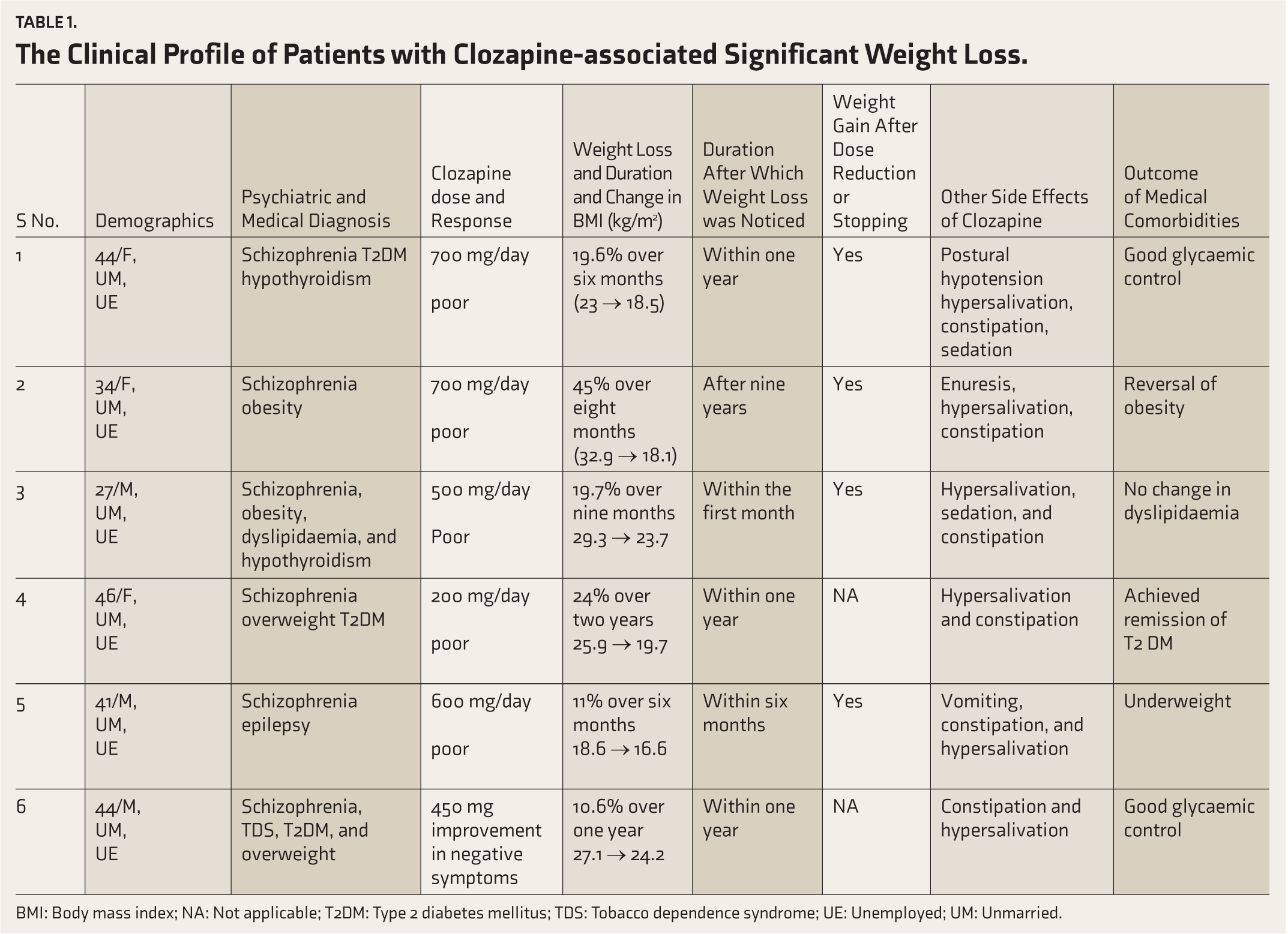
BMI: Body mass index; NA: Not applicable; T2DM: Type 2 diabetes mellitus; TDS: Tobacco dependence syndrome; UE: Unemployed; UM: Unmarried.
Discussion
In this case series, we have highlighted significant weight loss associated with clozapine in six patients, which contributes to the existing literature on this rare and less explored phenomenon. 7 Review of extant literature, which is primarily based on a few case reports, reveals three patterns of weight loss associated with clozapine. The first pattern is related to the response to clozapine, which resulted in improvements in symptomatology and functioning, leading to better management of adverse effects, a healthier diet, and a more active lifestyle, ultimately contributing to weight loss.8–10 Second pattern is probably related to pharmacogenetic variability, where weight loss was directly attributed to clozapine. 11 In the third pattern, weight loss early in the course of the clozapine trial was associated with poor or partial response to clozapine.7, 12 Our observation aligns with the third pattern in five of the six patients who experienced weight loss early in the course.7, 12 This needs to be interpreted in the context of a few earlier studies, which have highlighted weight gain with clozapine as a predictor of treatment response.13–15 Delayed onset weight loss in one of our patients could be attributed to the second pattern, hypothetically. Sedation and obsessive–compulsive symptoms secondary to clozapine leading to compulsive dieting or exercise, resulting in weight loss, were reported earlier. 16 This was ruled out in our patients.
Potent antagonistic action at dopaminergic D2, serotonergic 5-HT2C, muscarinic M3, and histaminergic H1 receptors is implicated in antipsychotic-induced weight gain. 17 In contrast, weak antagonism or agonism at the 5-HT2C subtype of receptors is implicated in the lesser propensity to cause weight gain and anorexigenic effect by a few antipsychotics. 18 However, it is currently unclear about the mechanism of clozapine-associated weight loss, and genetic variation has been postulated to lead to this variability. 7
Most of the patients (four out of six) in our study had either an overweight or an obese status before initiating clozapine, similar to an earlier report. 11 Whether obesity or overweight status at the baseline predicts clozapine-associated weight loss subsequently needs to be explored further. Among the patients who had T2DM before commencing clozapine, all of them achieved reasonable glycaemic control, and one achieved remission, which is in alignment with an earlier report. Weight loss leading to improvement in insulin sensitivity has been postulated behind the apparent remission of diabetic status. 19
Conclusions
Although weight gain is traditionally reported with clozapine, clinicians need to be aware that weight loss is noted in a subset of patients. A thorough physical evaluation of the identified patients is warranted to exclude any other treatable medical conditions to which weight loss can be attributed. While the mechanism of weight loss associated with clozapine has not yet been understood, weight loss as a predictor of poor response to clozapine can be helpful in clinical decision-making and needs to be explored in the future.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethics Committee Details
This case series was approved by the Departmental Scientific Committee, Department of Psychiatry, Kasturba Medical College, Manipal Academy of Higher Education, Manipal. This case series was exempted from review by the Institutional Ethics Committee, as the committee only requires formal review for case series involving more than 10 cases (Kasturba Medical College and Kasturba Hospital Institutional Ethics Committee). The document can be found at the following link:
(
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Not applicable.
Previous Presentation
This work was presented as an oral article by Dr Janani at ANCIPS 2024.
This article has not been submitted to other journal simultaneously for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.