
Abstract

Dear Editor,
Delirium tremens (DT) is a severe and potentially life-threatening complication of alcohol withdrawal. Although its prevalence is only 2% in individuals with alcohol dependence, it carries a mortality risk of about 30%. 1 It is a “short-lasting condition with a usual duration of 3–4 days.” 1 A few rare ones, though, are prolonged, especially in the presence of multiple medical and surgical comorbidities. 2 We present a unique case who had a 25-day “prolonged DT” despite having no obvious comorbidities for the most part. We provide a detailed description of the case to illustrate the management challenges and results of a literature review of 35 reported “prolonged DT” cases to explore underlying factors in the discussion.
Case Report
A 41-year-old married male, a fruit seller, with no significant past or family history and no medical comorbidity, was brought by his family members with disorientation and agitation for the past one day. He had a 20-year history of alcohol consumption in a dependence pattern with a current average daily intake of 720 mL of whiskey and 1 L of “kallu/toddy,” a form of country-made liquor (CML). He also has a history of chewing tobacco in a dependence pattern. Last use of both alcohol and tobacco was five days prior to the onset of symptoms. Upon examination, the patient had exhibited coarse tremors with constant agitation, disorientation to time, place, person, decreased attention span, Clinical Institute Withdrawal Assessment for Alcohol-revised (CIWA-Ar), 3 scale score of 13, Richmond Agitation-Sedation Scale (RASS), 4 score of +2. Patient was diagnosed with alcohol induced delirium and nicotine dependence, according to International Classification of Diseases–11th Revision (ICD-11). 5
He was admitted, and all routine investigations, including a complete blood count, liver and renal function tests, serum electrolytes, and electrocardiography (ECG), were within normal limits (
A magnetic resonance imaging (MRI) of the brain was performed to rule out any organic causes of prolonged delirium, which showed no abnormality. He was maintained on the same regimen for the next 10 days. On day 18, during an episode of aggression, he pulled out the urinary catheter, leading to urethral rupture and subsequent fever spikes, which were medically managed over the next five days. The CIWA-Ar scores gradually started declining from day 23. Diazepam was tapered and discontinued over the next 11 days. Motivational enhancement therapy and baclofen 40mg as an anticraving agent was initiated before being discharged, as the patient declined disulfiram and could not afford naltrexone or acamprosate. Consent for the publication of this report was obtained from the patient.
Summary of Overall Treatment Course.
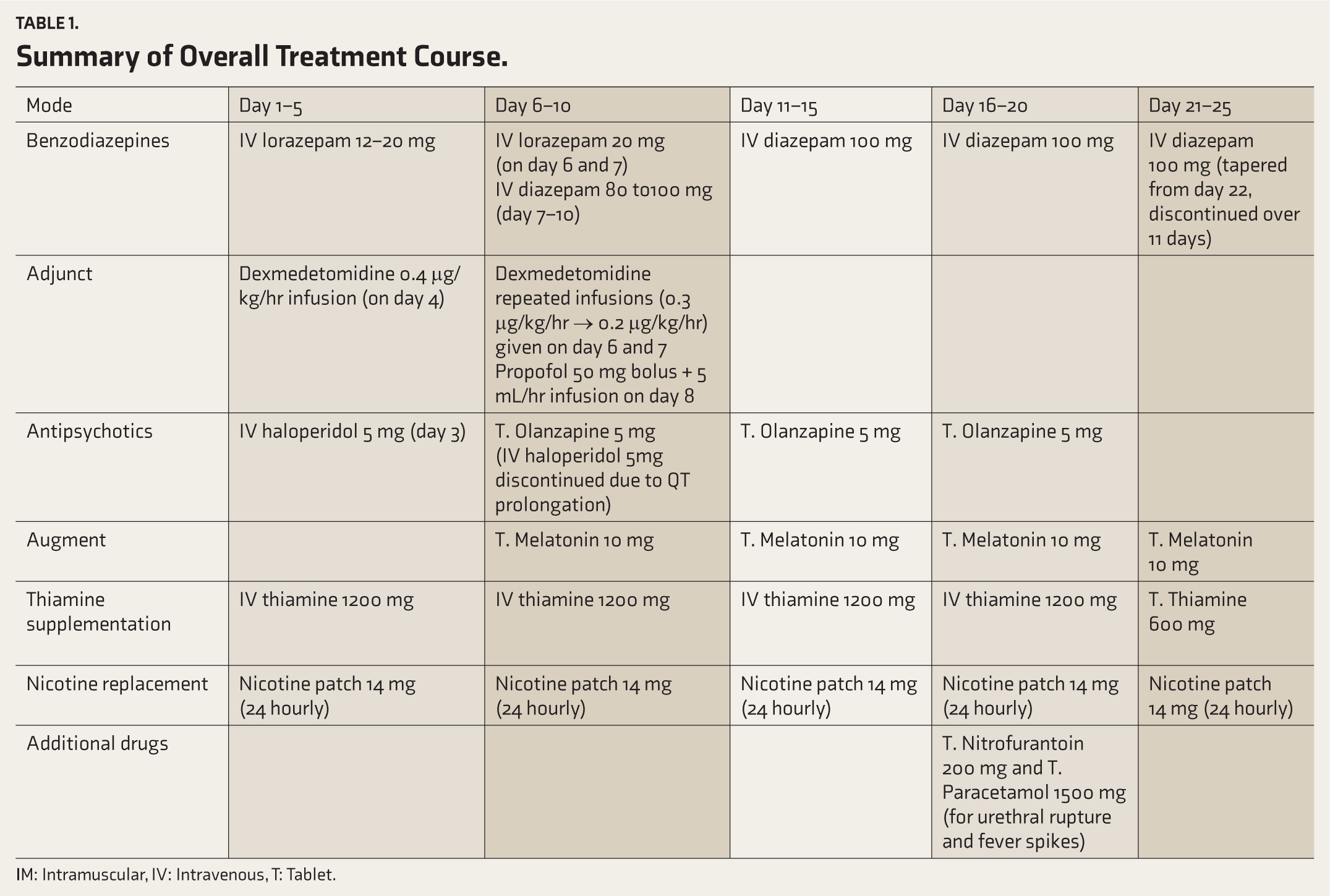
IM: Intramuscular, IV: Intravenous, T: Tablet.
Discussion
This report highlights a case of “prolonged DT” who required management with multiple pharmacological interventions, beyond the routine benzodiazepine-based detoxification, like most cases reported in the literature.
A literature review (see supplementary material;
Overall, there is also a need for the standardization of definitions and treatment protocols corresponding to the duration and severity of DT use, taking into account comorbidities.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.