
Abstract

Obsessive-compulsive disorder (OCD) affects 1%–3% of the population, with ~50% not responding to standard treatments. 1 Brain stimulation techniques like transcranial magnetic stimulation (TMS) and deep brain stimulation (DBS) show promise for treatment-resistant OCD (TR-OCD). 1 Deep TMS is FDA-approved, and new protocols are under investigation. 2 The most evidence-based TMS approaches target the right dorsolateral prefrontal cortex (DLPFC) and supplementary motor area using an inhibitory protocol and high-frequency deep TMS over the DLPFC. 2 TMS shows a medium effect size (Hedges’ g = 0.64) and a threefold increase in the odds for response, with 40%–50% of patients benefiting and generally tolerating well.3,4
However, FDA-approved TMS requires daily sessions over 6–8 weeks, which can be bothersome. 5 Accelerated TMS (aTMS), offering two or more sessions/day with short intersession intervals, has FDA approval for depression.5,6 Early studies and case reports suggest that aTMS is tolerable and potentially more effective.7,8 This case series presents outcomes from 11 OCD patients with persistent symptoms treated with aTMS targeting the right DLPFC, adding to growing evidence for this approach.
Case Series
Eleven OCD patients underwent aTMS targeting the right DLPFC between July 2022 and November 2024 at the Clinical Research Centre for Neuromodulation in Psychiatry, at Kasturba Medical College, Manipal, a tertiary care centre in South India (Table 1). The treatment chart was reviewed from the register maintained for all patients who received brain stimulation at the center. The mean age of the participants was 34.5 ± 12.2 years, and the average illness duration was 9.0 ± 7.0 years. Referrals were made for treatment resistance, persistent symptoms, medication intolerance, or the need for rapid symptom relief. All but two had failed at least one anti-obsessive medication, with a mean of 1.6 ± 0.8 failed trials (range: 0–3). All provided written informed consent and were screened for eligibility using the TMS adult safety screen of Keel et al. 9 Case series are exempted from approval from the institutional ethics committee of Kasturba Medical College and Kasturba Hospital.
Demographic, Clinical Details, and Treatment Protocols of the OCD Patients.
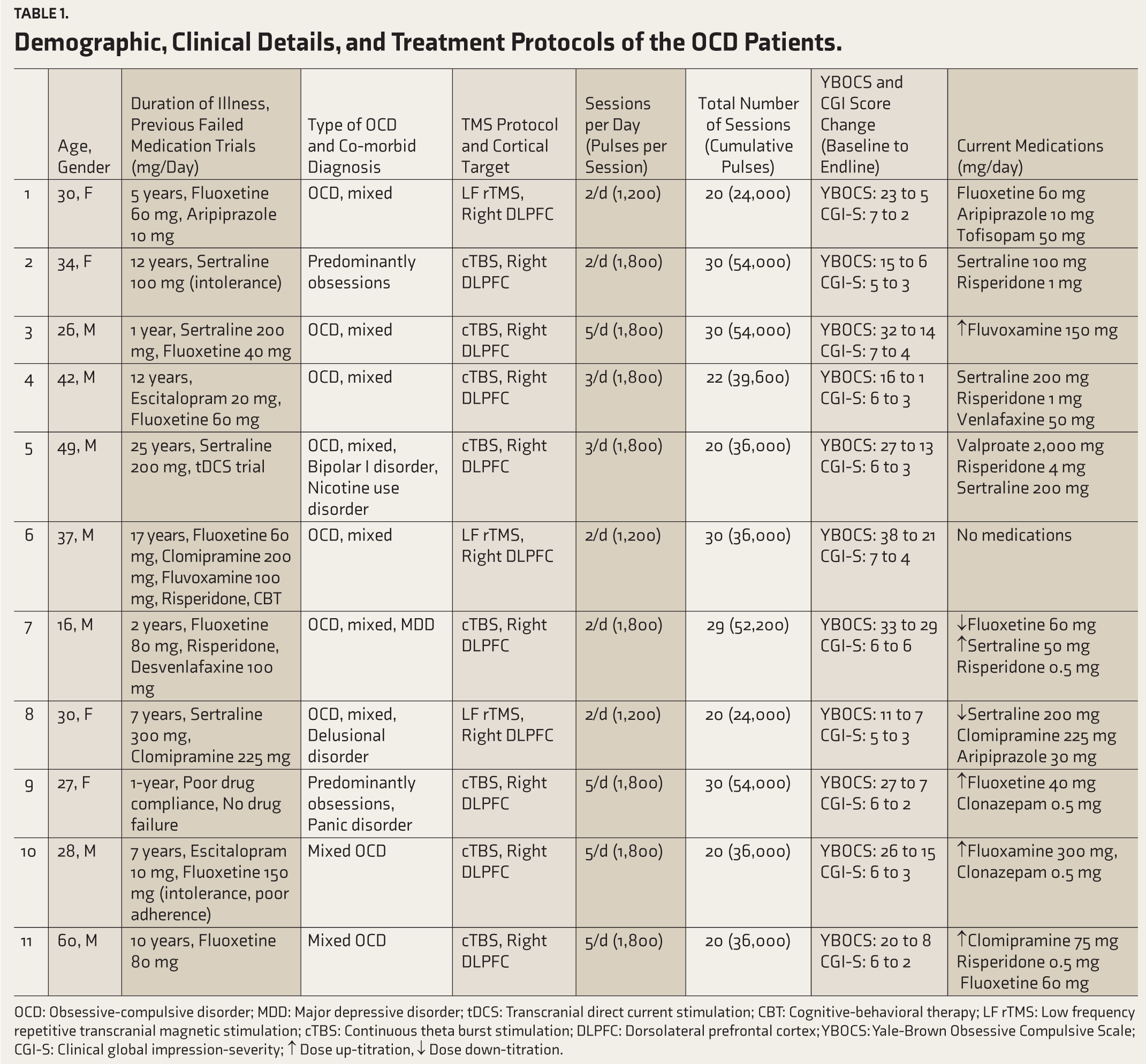
OCD: Obsessive-compulsive disorder; MDD: Major depressive disorder; tDCS: Transcranial direct current stimulation; CBT: Cognitive-behavioral therapy; LF rTMS: Low frequency repetitive transcranial magnetic stimulation; cTBS: Continuous theta burst stimulation; DLPFC: Dorsolateral prefrontal cortex; YBOCS: Yale-Brown Obsessive Compulsive Scale; CGI-S: Clinical global impression-severity; ↑ Dose up-titration, ↓ Dose down-titration.
The rTMS treatment included 1Hz low-frequency (LF) rTMS (1,200 pulses, 20 mins/session) for patients receiving two sessions daily, and 50Hz continuous theta burst stimulation (cTBS; 1,800 pulses, 2 mins/session) for those with more than two sessions daily. Treatments were delivered using Cool-B70 Magventure MagPro X-100 coils (posteroanterior, 45° coil angle), targeting the right DLPFC localized via the Beam F3 method. 10 Resting motor thresholds (RMTs) were determined using the Rossini-Rothwell method at the right motor hotspot for the left hand’s first dorsal interosseus muscle, per Groppa et al. 11 Treatments were delivered at 110%–120% of RMT, and side effects were monitored after each session using the TMS Side Effect Questionnaire by Giustiniani et al. 12 Patients underwent an accelerated protocol averaging 3.3 ± 1.4 sessions/day (range: 2–5), totaling 24.6 ± 5.0 sessions over 9.0 ± 3.6 days. The mean cumulative dose of rTMS was 40,527 ± 11,455 pulses.
Symptom severity was assessed using the Yale-Brown Obsessive-Compulsive Scale (YBOCS) 13 and the severity item of the Clinical Global Impression (CGI-S), 14 with progress monitored every five sessions. Response was defined as a >35% reduction in YBOCS score. Baseline symptom severity was high, with mean YBOCS and CGI-S scores of 24.2 ± 8.3 and 6.1 ± 0.7, respectively. The mean YBOCS score reduced by 12.9 points (95% CI: 9.2–16.6), showing a significant reduction from baseline (M = 24.2, SD = 8.3) to post-treatment (M = 11.5, SD = 8.1), t (10) = 7.8, p < .001, with a large effect size (Cohen’s d = 2.35). Significant improvements were seen in obsession (mean difference (MD) = 6.5, t (10) = 7.3, p < .001, Cohen’s d = 2.20) and compulsion (MD = 6.4, t (10) = 5.1, p < .001, Cohen’s d = 1.53) subscales. CGI-S scores also improved significantly from 6.1 ± 0.7 to 3.2 ± 1.2, t (10) = 7.4, p < .001, Cohen’s d = 2.24. As shown in Figure 1, 10 of 11 patients (91%) met the response criterion post-treatment. There was no difference in mean YBOCS score change in those receiving LF-rTMS (n = 3, M = 13.0, SD = 7.8) as compared to cTBS (n = 8, M = 12.9, SD = 5.1) (Mann-Whitney U = 11, p = .91).
Changes in YBOCS Score for Individual Patients Before and After rTMS.

Scores for patients 4, 5, 8, 10, and 11 are not available post-25th session.
End assessment was available for all patients.
Both baseline YBOCS score (r = 0.374, p = .257) and YBOCS change after five sessions (r = 0.599, p = .052) positively correlated with post-treatment YBOCS score change. The YBOCS change score had minimal correlation with age of onset (r = 0.217), duration of illness (r = 0.025), total number of sessions (r = 0.174), and total number of pulses (r = 0.092). YBOCS score change was lower in those with any comorbidity than those without (rpb = –347, p = .296). The treatment was well-tolerated, with no serious adverse effects at 110%–120% RMT. No patients discontinued due to adverse effects. Common side effects included stimulation-site pain, eyebrow twitches, coil pressure discomfort, and headaches—all resolved without interventions.
Discussion
We observed a rapid and significant symptom reduction within approximately ten days, aligning with findings from previous aTMS studies in OCD.7,15 CGI-S scores also showed marked improvement, reflecting overall improvement in both symptoms and functioning. Unlike conventional TMS, which typically requires 6–8 weeks of daily sessions, aTMS offers substantial symptom relief over a shorter duration, addressing the limitations of extended treatment schedules. 5 Our findings suggest that aTMS can effectively reduce symptoms within two weeks, making it a viable acute treatment option. Similarly, an open-label study using fMRI-guided aTMS (10 sessions/day over 5 days) targeting the right frontal pole reported significant YBOCS reduction and a 57% response rate by day 14. 7
In our study, 91% of patients met the criteria for treatment response—higher than rates reported in prior aTMS studies. For example, a randomized controlled trial found response rates of 60.8% with aTMS and 31.8% with conventional TMS. 15 Our results further support the safety and tolerability of aTMS, with all patients completing treatment without serious adverse effects. Although the choice between cTBS and LF rTMS was based on convenience, both protocols are backed by prior evidence for efficacy and tolerability.7,16 We used a 60-minute intersession interval (ISI), in line with research showing ISIs over 30 minutes yield optimal cortical excitability changes. 5 Most aTMS studies adopting ISIs of 50–60 minutes have reported significant clinical benefits.6,7,15
Greater baseline symptom severity was associated with greater symptom reduction following rTMS. Improvement after the fifth session strongly predicted overall outcomes. Symptom reduction showed minimal correlation with age of onset, illness duration, session count, or pulse number, but was lower in those with co-morbid disorders. Due to the small sample size, firm conclusions about these associations cannot be drawn, and previous studies have reported conflicting findings.17–19
TMS has emerged as a promising treatment for TR-OCD, offering significant symptom reduction and improved quality of life where other interventions have failed.2,4 In our study, patients unresponsive to multiple antidepressant trials showed significant improvement with aTMS. Neuromodulatory approaches such as TMS and deep brain stimulation (DBS) are especially promising, as they directly target hyperactivity in the cortico-striato-thalamo-cortical (CSTC) circuit implicated in OCD. 20 TMS targeting DLPFC has been shown to reduce activity in the cognitive control network, leading to symptom reduction. 21 Our choice of the right DLPFC was based on this neurobiological rationale and supported by a recent systematic review identifying inhibitory TMS to the DLPFC as having the strongest evidence base for OCD treatment. 2 Additionally, a recent study found that inhibitory TMS to the right frontal pole reduced DLPFC activation in responders, further validating this target. 7 The right DLPFC is also a practical site for neuromodulation with standard figure-of-eight coils due to its superficial location. In contrast, deeper targets such as the orbitofrontal cortex (OFC) and medial prefrontal cortex (mPFC) require specialized deep TMS coils, making them more complex to use in routine clinical settings. 22
The main limitations of our study are the absence of a control group and the small sample size. Also, treatment involved two different treatment protocols, LF-rTMS and cTBS, in this case series. Furthermore, medication doses were adjusted for six patients, which could confound the findings. Nonetheless, the findings support the clinical utility and feasibility of inhibitory aTMS targeting the right DLPFC as an acute intervention for persistent OCD symptoms. Future research should prioritize large-scale randomized controlled trials to validate efficacy, refine treatment protocols, and overcome the limitations of small-scale studies.
Conclusions
This case series demonstrates that aTMS protocols can be effective for patients with treatment-resistant or persistent OCD symptoms, showing significant improvements in YBOCS and CGI-S scores and a faster time to response. However, controlled studies are needed to further validate efficacy and tolerability. Future research should also include follow-up assessments to evaluate the durability of symptom improvement.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
Nil.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Approval
Case series are exempted from review by institutional ethics committee of Kasturba Medical College and Kasturba Hospital.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JTJ’s salary is supported by the Clinical/Public Health Research Centre Grant from the DBT/Wellcome Trust India Alliance (IA/CRC/19/1/610005). SKP is the site PI of the funded Clinical Research Centre for Neuromodulation in Psychiatry project.
Informed Consent
Written informed consent was obtained from all the participants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.