
Abstract

Levetiracetam, an S-enantiomer pyrrolidone derivative, has demonstrated notable effectiveness in treating both focal and generalized epilepsy.1–2 It was approved by the U.S. Food and Drug Administration in 1999 for the adjunctive treatment of partial-onset seizures. It is proposed to act by interfering with chloride influx at gamma-aminobutyric acid (GABA) and glycine receptors, thereby reducing neuronal excitation. 3 While its antiepileptic effects are well-documented, a significant but often overlooked aspect of levetiracetam therapy is its association with neuropsychiatric side effects, including behavioral and psychotic symptoms. 4 However, according to Aggarwal et al. psychosis has been infrequently reported with levetiracetam. 3 Studies show that about 16% of patients on levetiracetam may experience behavioral side effects, with 13.3% of adults experiencing symptoms of depression, emotional lability, and less frequent psychosis.5–6 Severe symptoms such as agitation and hostility are observed in only 0.7% of cases, while the estimated prevalence of developing psychosis is approximately 1.4%. 6 Our review of the literature indicates evidence of levetiracetam-associated behavioral disturbances. However, there are only limited case reports on manic and psychotic manifestations with limited emphasis on symptomatology and patterns of resolution. Here, we present a case series of six patients who developed acute neuropsychiatric symptoms, including three cases with psychotic symptoms and three cases with manic symptoms, shortly after initiation or dose escalation of levetiracetam. To systematically assess the severity and progression of psychiatric symptoms, we employed the Brief Psychiatric Rating Scale (BPRS) for evaluating overall psychopathology and the Young Mania Rating Scale (YMRS) for quantifying manic symptoms. Through this case series, we aim to underscore the clinical significance of vigilant monitoring for psychiatric symptoms in patients on levetiracetam.
Case Series
This case series highlights six patients with no past or family history of mental illness developing significant neuropsychiatric symptoms after starting or increasing the dose of levetiracetam. The first case (Table 1, S. No:01) involved a 34-year-old woman with focal seizures who, following a dose increase, became excessively talkative, irritable, and had insomnia. Her symptoms resolved once levetiracetam was replaced with sodium valproate. The second case (Table 1, S. No:02) involved a 35-year-old woman who, within a week of the levetiracetam dose increase, developed irritability, agitation, and emotional instability. Switching her to sodium valproate led to a full recovery. The third case (Table 1, S. No:03) was a 17-year-old boy with a known case of seizure disorder who, within three days of a levetiracetam dose increase for break-through seizures, became restless, irritable, and unable to sleep. His symptoms disappeared after switching to sodium valproate. The fourth case (Table 2, S. No:01) was a 38-year-old man who had suffered a traumatic brain injury and was started on levetiracetam for anti-seizure prophylaxis. Two weeks later, his family noticed he was unusually irritable and had unprovoked aggression and suspiciousness of being harmed. His symptoms improved upon switching to brivaracetam. The fifth case (Table 2, S. No:02) was a 54-year-old male who developed seizure episodes after a head injury and was started on levetiracetam, following which he experienced paranoia, anger outbursts, and hearing non-existing voices. He returned to his premorbid self after switching to sodium valproate. The sixth case (Table 2, S. No:03) was a 37-year-old man with a history of dissociative episodes who, after starting levetiracetam, developed paranoia, food refusal, and distressing visual hallucinations. His symptoms improved within days of stopping the medication. In all cases, the Naranjo scale suggested a likely link between initiation or dose escalation of levetiracetam and emergent psychiatric side effects, emphasizing the importance of monitoring mood and behavior changes in patients on this medication. 7
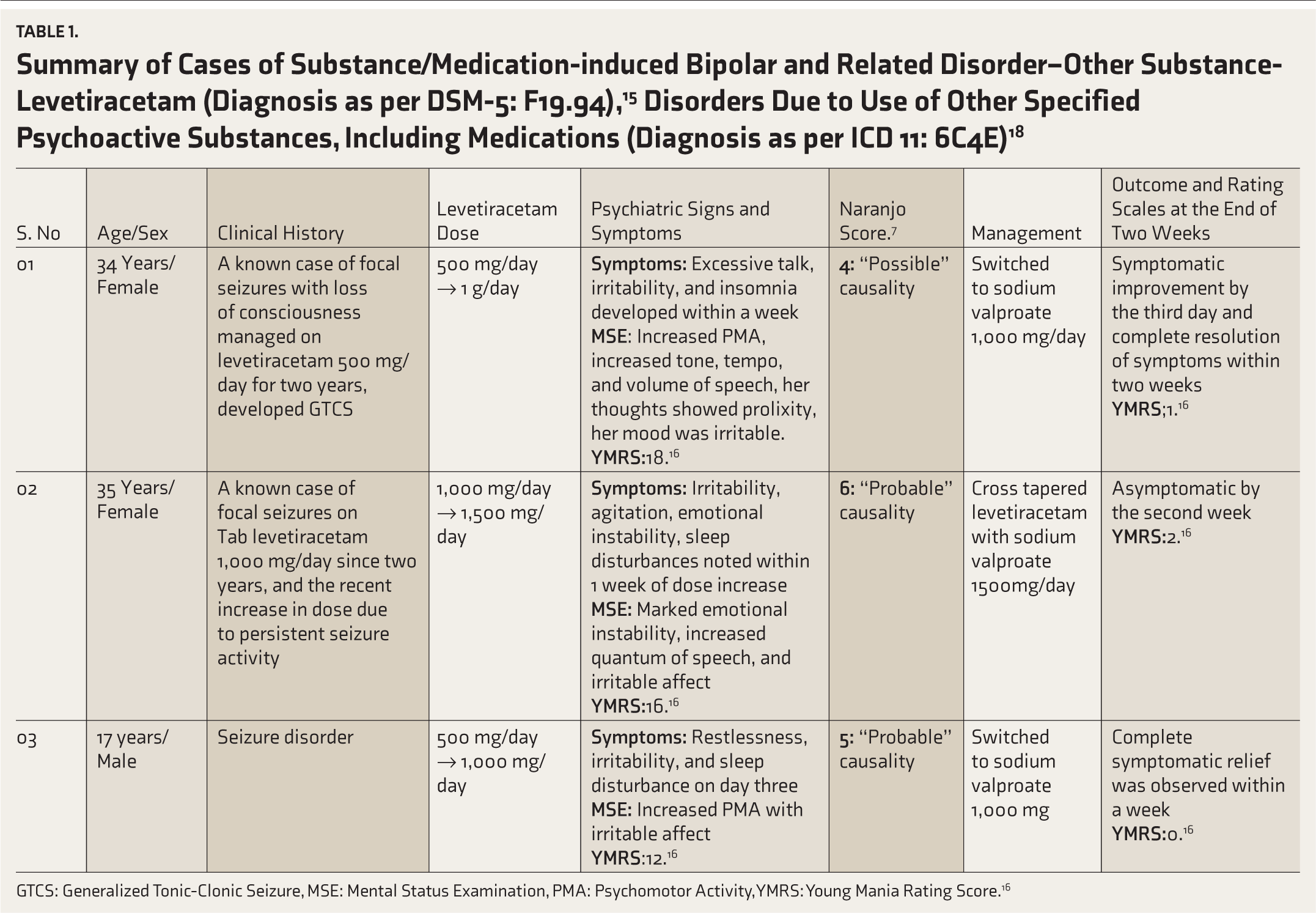
GTCS: Generalized Tonic-Clonic Seizure, MSE: Mental Status Examination, PMA: Psychomotor Activity, YMRS: Young Mania Rating Score. 16
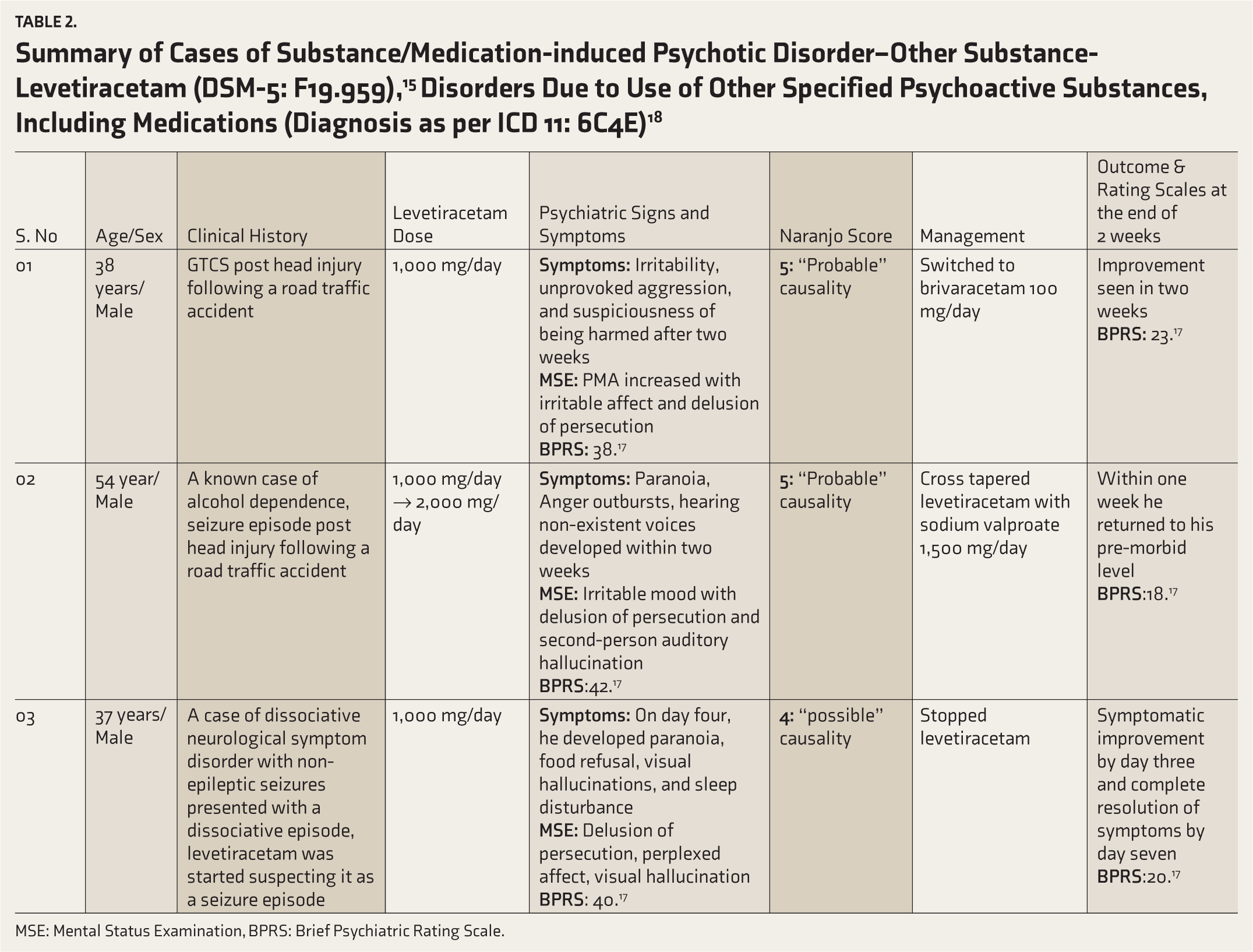
MSE: Mental Status Examination, BPRS: Brief Psychiatric Rating Scale.
Discussion
Levetiracetam binds to the synaptic vesicle protein 2A, a glycoprotein implicated in neurotransmitter release. Though not fully understood, its antiepileptic action likely involves modulating neurotransmitter exocytosis, reducing calcium currents, enhancing GABA levels, dampening glutamate action via α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPA receptor) receptor modulation, and modulating serotonergic and adrenergic pathways. These mechanisms suggest levetiracetam’s broad pharmacological effects that may contribute to anti-seizure effects and adverse behavioral effects like anxiety, suicidal thoughts, irritability, aggression, and tantrums. 8
In a study by Campbell et al. levetiracetam produced neuropsychiatric side effects in about 18% of epilepsy patients, often leading to dosage modifications or discontinuation of the drug. These adverse reactions exhibit a broad spectrum of manifestations, including affective and behavioral symptoms and suicidal thoughts. Notably, levetiracetam is linked to a roughly 1% incidence of drug-associated psychotic symptoms, a rate significantly higher than that seen with other anti-seizure medications. 9 In a long-term follow-up study by Delanty et al. levetiracetam demonstrated a favorable safety profile. However, psychiatric side effects were reported in up to 13.3% of adults and 37.6% of pediatric patients, with notable symptoms such as depression, agitation or hostility, and psychotic symptoms occurring in 0.7% of cases. 10 A systematic review by Cramer reported that psychiatric symptoms caused by levetiracetam were reversible after discontinuation of the medication. 11 This finding is important as it indicates that psychiatric side effects caused by levetiracetam have a causal relationship that is usually transient and subsides once the medication is discontinued.
In our case series, we described six cases presented with manic and psychotic symptoms, respectively, requiring inpatient care. In cases 1–3, an initial diagnosis of bipolar affective disorder was considered, and in cases 4–6, a diagnosis of brief psychotic disorder was diagnosed. However, upon further clarification, a temporal relationship between initiation or dose escalation of levetiracetam and onset of symptoms was established, and the diagnosis was revised to drug-associated manic symptoms and psychotic symptoms, respectively. The symptoms resolved upon discontinuation of the offending drug and/or shifting to different antiepileptic and supportive medications. To systematically evaluate the causality between levetiracetam use and the observed psychiatric symptoms, we employed the Naranjo Adverse Drug Reaction Probability Scale in each case. 7 In our cases, Naranjo scores ranged from 4 to 6, indicating a “probable to possible” relationship between levetiracetam and the observed adverse neuropsychiatric outcomes. This assessment aligns with literature reports indicating that levetiracetam may be particularly likely to provoke behavioral side effects. Based on the temporal sequence of events, evidence showed in previous literature of levetiracetam-associated neuropsychiatric manifestations and also the complete resolution of symptoms after stopping levetiracetam strengthened the hypothesis of the case series. The Naranjo Adverse Drug Scale also revealed a probable relationship between levetiracetam and the manifestations. The exact mechanism by which certain antiepileptics cause psychotic symptoms remains unknown. However, it is possible that individuals who experience this side effect could have an underlying vulnerability for a psychotic disorder that has not yet manifested clinically. Some studies report that pre-existing psychiatric conditions may increase the likelihood of behavioral side effects due to levetiracetam. 12 In these cases, the antiepileptic drug might serve as a precipitating factor.
Patients starting on antiepileptic treatment, particularly with levetiracetam, need long-term and comprehensive clinical monitoring with awareness of emergent adverse symptoms. 13 Clear diagnostic guidelines for levetiracetam-associated neuropsychiatric symptoms are yet to be established. However, in our cases, the full recovery from psychotic/manic symptoms upon discontinuation of levetiracetam aligns with the possibility of an adverse reaction, as indicated by Naranjo’s algorithm, thereby supporting the diagnosis. 14
Conclusion
There is emerging evidence of a correlation between levetiracetam and new-onset psychiatric symptoms. Although the causality in this correlation is less definitive, the diagnosis primarily relies on the temporal association. A limitation of our case series was the inability to analyze serum levetiracetam level. This case series highlights the need for close monitoring of neuropsychiatric manifestations, especially during the dose initiation or escalation. Early identification and drug modification can reduce patient morbidity and improve the quality of life. In addition, further large-scale studies are needed to assess levetiracetam’s behavioral profile and identify the risk factors for levetiracetam-associated neuropsychiatric manifestations.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank the patients and their families for consenting and willingness to participate in this case series
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Patient Consent to Participation and Publication
The authors certify that they have obtained all appropriate patient consent forms. In the form the patients and their legal representatives have given their consent for anonymized patient information, images, and other clinical information to be reported in the journal.
The patient(s) understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed. The patient(s) also understand that their consent can be withdrawn at any time, and this will not affect their ongoing or future treatment in anyway.
Declaration Regarding the Use of Generative AI
None used.
Ethical Considerations
Written informed consent was obtained from the patients and their legal representatives for publication of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Prior Presentations
This work has not been previously presented at any conferences or academic meetings.
Reporting Guideline (Supplementary Online Material)
We used the CARE checklist when writing our report (Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D; the CARE Group. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Development).
Simultaneous Submission to Another Journal or Resource
This work manuscript has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.