
Abstract
Background:
Multiple challenges, including limited technical knowledge, privacy concerns, or financial constraints to afford a smartphone, limit the introduction and implementation of a mobile application-based intervention aimed at supporting medication adherence for people with schizophrenia (SZ) in a low-resource setting. Recognising these barriers, this study aimed to explore the perceived acceptability of a mobile application specifically designed to improve medication adherence among individuals with SZ and their caregivers (CG).
Methods:
A total of 64 individuals diagnosed with SZ, who had been in remission for the past six months, and 36 CG, attending the outpatient psychiatry department of a tertiary care teaching institution, were recruited based on predefined selection criteria. The SZ and CG participants were interviewed separately using an adapted version of the Treatment Acceptability and Preference Scale (TAPS), which assessed their perceptions of the appropriateness, suitability, effectiveness, and willingness to use a mobile application. TAPS was administered immediately after describing the proposed features and potential utility of the mobile application designed to improve medication adherence.
Results:
There were no significant differences in demographic characteristics between SZ and CG, except that CG were significantly more likely to be employed than individuals with SZ (p = .02). Comparison of TAPS scores between the two groups revealed no significant difference in perceptions regarding the acceptability of the mobile application. However, a greater proportion of CG (63.9%) compared to individuals with SZ (56.25%) considered the mobile application to be appropriate. Correlation analysis indicated that younger age (p = .004) and higher levels of education (p = .01) were significantly associated with higher TAPS scores.
Conclusion:
The mobile application was generally acceptable to patients and CG, with younger and more educated participants showing higher acceptability.
This study aimed to investigate the perceived acceptability of a mobile application designed to improve medication adherence in people with schizophrenia and their caregivers. The mobile application was generally acceptable to patients and caregivers, with younger and more educated participants showing higher acceptability.Key Messages
Schizophrenia (SZ) is a severe mental disorder that significantly disrupts the lives of the affected people and their families. Adherence to medications is an essential aspect of overall management. Discontinuation of medication increases the risk of relapse fivefold. 1 Numerous interventions, including mobile-phone-based approaches, have been developed to improve medication adherence in general medical conditions. 2 Individualised strategies, like setting alarms and using checklists, have shown significant improvement in adherence. 3 According to a systematic review, 7 of 11 studies reported that mobile applications enhanced treatment adherence. 4 The average participant satisfaction score across these mobile applications was 8.1 out of 10. However, very few mobile applications to date have specifically targeted individuals with SZ, despite findings from a 2016 meta-analysis indicating that 66.4% of individuals with psychosis globally owned a mobile phone. 5 In North India, 84.4% of individuals with severe mental disorders owned a mobile phone. 6 Mobile applications can improve medication adherence in individuals with SZ if appropriately used.
Mobile applications have been developed for symptom monitoring, diagnostics, therapeutic, and supportive roles for participants with SZ.7–11 In the United Kingdom, a small study on 36 participants of early psychosis reported that the mobile application was feasible and safe, with 90% of them recommending the application and none of them reporting adverse effects. 7 Improvements were reported in participants’ negative, general psychotic, and mood symptoms. After one year, cognitive fatigability was improved with a mobile application-based intervention in a randomised controlled trial among participants with SZ in Poland. 11 Using a mobile application called PRIME to improve the motivation of SZ participants in the USA, Schlosser and colleagues reported significant improvement in self- reported depression and self-efficacy. 8 Additionally, a mobile application with multiple functions for supportive therapy was acceptable and usable for 90% of its SZ users, with a significant reduction in psychotic symptoms and depression. 9
Researchers from Canada used a mobile application with multiple functions (scheduling and text-based functions) to self-manage, improve medication adherence, reduce psychotic symptoms, and enhance recovery among participants with SZ. 10 Although there was no significant improvement in medication adherence, there was a significant improvement (52.5%) in some symptoms and retention rate on the application.
There is a lack of studies on mobile application-based interventions among Indian individuals with SZ, mainly due to various challenges in developing and implementing such interventions. 12 Apart from the mobile application’s challenges, barriers like financial constraints to afford smartphones and poor technical knowledge may reduce use. The present study, therefore, aimed to investigate people with SZ and their caregivers’ (CG) perceived acceptability of using a mobile application to improve their medication adherence. This preliminary study was part of a larger project aimed at evaluating the feasibility of using a culturally appropriate mobile application, developed in a local language, to enhance medication adherence among individuals with SZ.
Method
Study Design
After obtaining the approval of the Institutional Ethics Committee, we carried out a cross-sectional study in a tertiary care teaching institute in India from March to September 2024.
Participants
The individuals receiving treatment for SZ group, currently in remission, aged between 18 and 65 years, of any gender, able to read and understand Malayalam, and able to provide consent, were eligible to participate in the study. Remission was defined as ‘a state where a participant’s core symptoms have improved to the point that any remaining symptoms do not significantly interfere with their daily functioning for at least 6 months’. 13 Participants with active psychotic or mood symptoms, a history of substance use (except nicotine), or suffering from any serious physical illness were excluded from the study.
For participation, a CG Group was defined as the individual who primarily supported the participant, resided with them, and acted as the main point of contact for their medical needs. 14 The CG with a history of any mental illness or cognitive impairment were excluded from the study.
Sample Size
The minimum sample size was calculated from a previous study, 3 which compared using a checklist and other techniques (Pharm CAT) versus med e-monitor versus treatment as usual. They included 142 participants, with 48 participants in the Med E monitor and 47 each in the other two groups. Adherence averaged 91% for the Med E monitor group, 90% for the pharm cat group, and 72% for the treatment as usual group. Considering 95% CI and 10% precision 3 and using the formula-Z1-α/2pq/d 2 where p is the proportion, q is 100-p. The sample size was calculated to be 43 people with SZ. Additionally, we included their CG if available.
Study Instruments
Socio-demographic Proforma
A semi-structured proforma was designed to collect socio-demographic factors, including age, gender, educational status, marital status, occupations, residence, and socioeconomic status. Clinical factors included the age of onset of illness, total duration of illness, current clinical status of participants, time since remission, treatment details, including the medications and supportive treatment methods. Information about other comorbidities and the availability of smartphones for individuals with SZ and CG was also included.
Description of the proposed mobile application: The mobile application featured educational videos on SZ in Malayalam. The educational videos included information about the illness, education, awareness about the need for medications, side effects, and a video about common doubts and answers regarding SZ. This content was aligned with the perceived needs of individuals with SZ and their CG, as reported in previous studies from India.15, 16 The application provided reminders for taking medication and offered virtual rewards (e.g., badges) to enhance adherence. The application also included reminders for follow-up visits. Recorded question-and-answer sessions, relevant reading materials addressing common doubts, and information about the illness and medications were available.
Treatment Acceptability and Preference Scale (TAP) 17
The TAP was developed by Sidani et al. (2009) and is free for academic and clinical use. The TAP consists of four items assessing the appropriateness of using a mobile application for this condition, suitability for you/your family member, effectiveness for your/your family member, and willingness to comply with the use of the mobile application. The ratings are given on a 5-point scale ranging from not at all (0) to very much (4); thus, higher scores indicate a perception that the treatment option is appropriate, suitable, and effective, and participants are willing to adhere to it. A total scale score is computed as the mean of the four items’ scores to reflect the level of perceived treatment acceptability. The possible range for the total scale score is 0–4, with a high score reflecting high acceptability. The scale was translated into Malayalam and back-translated into English. The Malayalam translated version of the scale was used to collect the data. The items measuring treatment acceptability were internally consistent (alpha >80) and demonstrated validity, evidenced by a one-factor structure and differences in the scores between participants with preferences for specific interventions. 17 Along with this scale, we added one question to assess the confidence of participants and family members in using the mobile application. The question was ‘Do you think you will be able to use the mobile application?’ Three more open questions with qualitative responses were added to assess the mobile application’s perceived barriers and facilitators. We included participants’ and CG’ suggestions for improvement and perceived barriers to using the mobile application. These questions were ‘Do you want to include any particular feature in the mobile app?’ ‘Do you think you will face any barriers when using this mobile application?’ ‘How can we help you overcome those barriers?’
Procedure
The study population was individuals with SZ (diagnosed per ICD-10) and their CG. A purposive sampling method was used. Initial screening was carried out by the treating psychiatrist in the psychiatry outpatient department. Participants in clinical remission and their family members were informed about the study, and their written informed consent was obtained. Thereafter, both groups were interviewed separately.
A semi-structured proforma was used to collect socio-demographic and clinical data. Following this, participants were presented with detailed descriptions of the features and utility of mobile applications designed to improve medication adherence as described above. Our actual mobile application was not given to the participants directly. Only a detailed description of the application was provided. A script was used to ensure the uniformity of description. After describing the mobile application’s features and utility, the adapted version of the treatment acceptability scale was applied, followed by open-ended questions about suggestions, perceived barriers, and possible solutions for the perceived barriers.
Statistical Analysis
Scores on the TAP scale were added, and the mean score was calculated separately for the individual with SZ and CG. Statistical analyses were conducted using SPSS version 20. 18 The continuous data’s mean and standard deviation, as well as the discrete data’s frequency and percentage, were calculated. The Mann-Whitney U test was used to compare the perception scores of participants and their CG. The correlation analysis assessed the correlation of perception scores with various socio-demographic parameters.
Results
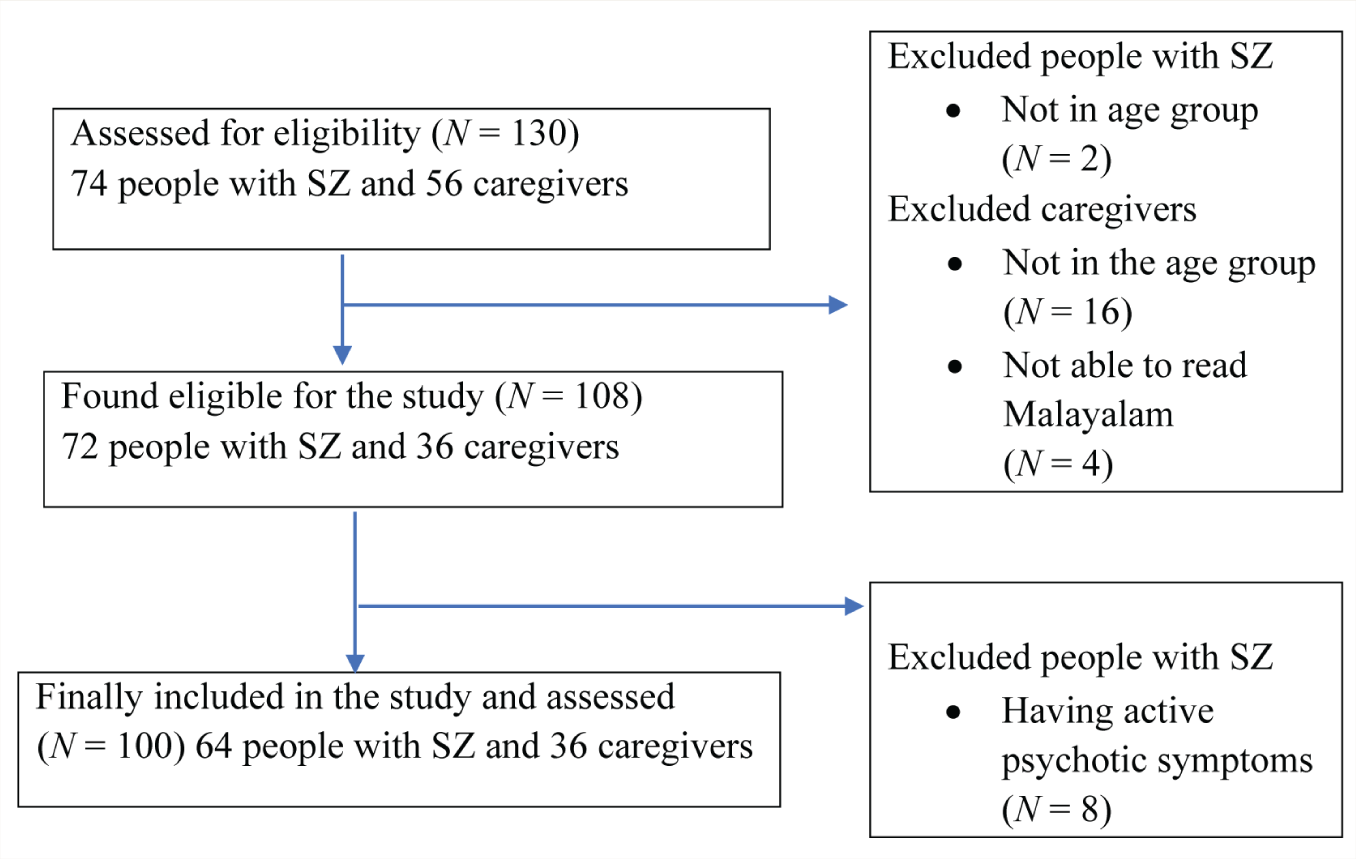
After screening all the patients attending the Psychiatry OPD over the study period, 74 people diagnosed with SZ and 56 CG were assessed for eligibility. Finally, 64 people with SZ and 36 CG completed the study (Figure 1). The demographic profile of the study groups is shown in Table 1. There were no differences in demographics between SZ and CG groups, except that participants in the CG group were significantly more employed than those in the SZ group (p = .02). The mean age of the people with SZ was 43.47 years (SD ± 12.4) while the mean age of their CG was 48.22 years (SD ± 11.6), and there was no significant difference between them (p = .06). The mean age of onset of illness was 26.64 years (SD ± 9.6), with a mean total duration of illness of 14.63 years (SD ± 9.6), and there was no significant difference between male and female participants (p = .75, p = .77), respectively. In keeping with our inclusion criteria, all people with SZ were in remission at the time of study and did not report any active psychotic symptoms. However, two participants reported occasional sleep disturbances, and another two reported occasional anger outbursts. All the participants were on oral antipsychotics, and 14 (21.9%) were receiving clozapine. One participant was receiving an additional depot injection of Fluphenazine along with oral antipsychotics. Six participants had co-morbid diabetes and were on oral hypoglycaemic drugs. Five participants had hypothyroidism. Two participants were taking treatment for Hypertension. Out of 100 participants, 24 with SZ (37.5%) and 14 CG (38.9%) owned a smartphone.
Flow Diagram.
Sociodemographic Profile of Participants.

p value <.05 is considered as significant.
SZ: Schizophrenia.
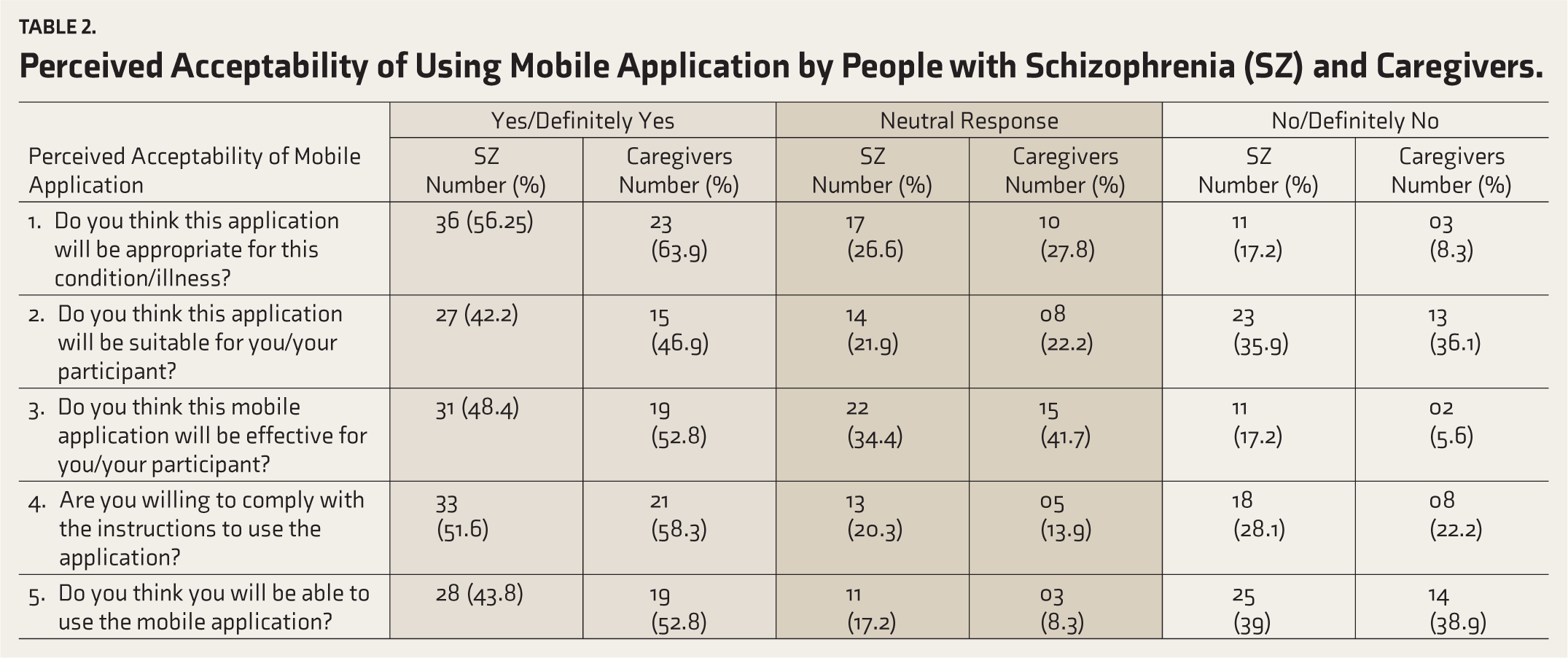
Participants’ responses to various measures of perceived acceptability of mobile applications demonstrate that a greater number of CG versus SZ felt the mobile application would be appropriate [36 (56.25%) SZ vs. 23(63.9%) CG]. A slightly greater proportion of CG than people with SZ felt that the proposed application would be suitable [27 (42.2%) SZ vs. 15 (46.9%) CG] and effective [31(48.4%) SZ vs. 19 (52.8%) CG]. Similarly, a larger proportion of CG [28 (43.8%) SZ vs. 19 (52.8%) CG] believed they would be able to use the mobile application (Table 2).
Perceived Acceptability of Using Mobile Application by People with Schizophrenia (SZ) and Caregivers.
A comparison of TAP scores between participants and CG revealed no significant difference between the perception of mobile application acceptability scale scores between the SZ group and the CG group (p = .37) (Table 3).
Comparison of Perception of Mobile Application Acceptability Scale Score Between People with SZ and Caregivers.

p value < .05 is considered significant.
Correlation analysis showed a significant relationship between age and the TAP score (p = .004), in that the lower the age, the higher the TAP scale score. A significant correlation was also found between education and the TAP score. Intermediate and higher education participants had significantly (p = .01) higher TAP scores. None of the other parameters, including employment status, residence, or socioeconomic status, had any significant correlation with TAP scores in people with SZ or CG.
Between 40% and 50% in both groups agreed that the mobile application is valid or definitely useful. The people with SZ and CG suggested a few specific additional features. Three participants asked for online counselling sessions through the mobile app. One participant suggested adding social media-like connections to find job opportunities, another to add the facility to consult the doctor over a mobile application, and a third to add services to reduce the stigma of mental illness.
Thirty people with SZ (46.9%) did not know how to use a smartphone. Four participants reported a lack of internet connection at home, and two reported they did not prefer to use their mobile phones, as people might find out about their illness. However, they indicated they were comfortable using their CG mobile phones.
Discussion
Despite the high number of mobile mental health applications available globally, the use of these applications remains low among people with mental illness and their caregivers.19, 20 There is a lack of adequate literature about the use of digital applications in SZ from low to middle-income countries like India. Community engagement and direct information from persons with SZ and their CG are necessary, along with scientific evidence and technical expertise, in developing any digital tool for people with severe mental illness.21, 22 Hence, we aimed to assess the perceived acceptability, needs, and barriers of using mobile applications designed to increase medication adherence among people with SZ and their CG.
Although this was a pilot study, we recruited an adequate sample representative of our population, using a culturally acceptable translation of the TAP. Unlike the results from a meta-analysis, which showed a majority of male participants (61.1%), 5 our study sample consisted of 53% male and 47% female participants with SZ, along with an equal distribution of male (50%) and female (50%) CG. The mean age of individuals with SZ in our sample was 43.47 years, which closely aligns with the mean age of 43.3 years reported in a meta-analysis comprising 3,227 participants. 5 Globally, employment rates among individuals with SZ vary widely, ranging from 4% to 50.4%. 2 3 This variability is likely influenced by a range of socio-cultural factors that affect both the acquisition and sustainability of employment, including stigma, workplace accommodations, family support, and broader economic conditions. Notably, 46.9% of our participants were currently employed, a proportion higher than that reported in previous studies from Malaysia (30%), as well as the pooled employment rate of 25.3% found in the meta-analysis mentioned above.5, 24 This comparatively higher employment rate may be attributed to the fact that all participants in our study were in clinical remission, which is likely to have positively influenced their functional capacity and vocational engagement.
The mean age of onset of illness in our sample was (26.64 ± 9.6 years), similar to previous Indian (23.8 years) and USA (25.5 years) studies. 25 The mean total duration of illness was 14.63(9.6) years, higher than the Indian study (7.5 years) reported by Dev et al. 16
We found that only 38% of our participants owned a smartphone. This finding is similar to those reported in a previous North Indian study (38.6%) and the national average in 2018 (30%),16, 26 but much lower than in the US (63% in 2013). 27 Multiple factors could contribute to this low prevalence. Most of our participants (60, 93.8%) were from a low socioeconomic status, and 61 (95.3%) were from a rural background. In many cases, the household had only one phone shared by the entire household.
Despite the low prevalence of smartphone ownership among participants and CG, we found that the perceived acceptability of using the mobile application to improve medication adherence was high. This is in line with the results of a qualitative study conducted in Madhya Pradesh, India, among patients with SZ and CG, in which participants perceived that a single mobile application with comprehensive information would be helpful. 15 Our acceptance rates were significantly higher than those of a 2013 US-based needs assessment survey (56.25% of participants and 63.9% of CG in our group, compared to 44% in the US). 27 In this older US survey, only 44% of participants expressed interest in using a mobile application for medication reminders, and only 31% were interested in receiving psychoeducation and information about treatment and services. Compared to another US online survey on 457 people with SZ, our rates for future assurance of medication compliance were also higher, even higher than the actual use of digital applications to improve medication management among the US SZ participants (only 28% of participants used technology for medication management). 25
In our sample, younger age (p = .004) (r = -0.355) and higher education (p = .01) (u = 289) significantly correlated with higher acceptability. This aligns with the growing interest in digital technology among the younger generation and has had a positive impact on general education globally. 28
Our participants requested additional features and services for the proposed mobile application. They requested online counselling sessions, online doctor consultations, measures to reduce the stigma towards illness, opportunities for interpersonal connections with other people with SZ, and opportunities to find jobs for the patients. Online doctor consultations are possible through ‘E Sanjeevani’, a telemedicine initiative in India. 29 Internationally, peer-to-peer support has been used in a few mobile applications designed for persons with psychosis.8,10,30 However, around the world, fewer patients and CG utilise the opportunity for bigger interpersonal networks and occupational opportunities via digital interventions. 21
Several participants reported barriers, including a lack of a smartphone, not knowing how to use the smartphone, a lack of internet connection, and doubts regarding privacy issues. Some of these barriers, like the cost to afford the smartphone and a lack of technical knowledge, were reported in another study from North India. 31 Patients and CG raised concerns regarding data privacy in another qualitative study from Madhya Pradesh, India. 15 We could solve the language barrier mentioned by participants in previous studies by tailoring mobile app content in the local language, Malayalam. 32 As smartphones’ cost, user-friendliness, and security features improve over time, these barriers may crumble. Despite these drawbacks, our participants were hopeful of the usefulness of our proposed mobile application. Some participants were ready to buy a smartphone to improve medication adherence. It suggests that if a mobile application-based intervention is available in their local language, it is acceptable to individuals with SZ even in India.
Based on these inputs, we intend to add some features to our proposed mobile application, such as suggestions to reduce stigma. We will use a non-stigmatising name for the mobile application (‘Pathivu’ in Malayalam, meaning ‘as usual’ in English), and the app will provide proper information about the illness to reduce the stigma in the community. 15
Limitations
Unlike other studies on the acceptability and usability of mobile applications, our actual mobile application was not given to the participants directly. Only a detailed description of the application was provided. This method likely limits them from fully understanding its use and utility. Moreover, we only recruited participants from one outpatient clinic and only those who spoke the local language, which may limit the generalisability of results. Only persons in remission were included in the study. It may affect the generalisability of the results in all persons with SZ.
Despite these limitations, our study helped to identify the needs and barriers to using mobile mental health applications in patients with SZ. Our findings will help further modify the mobile application and deliver to participants in a people-centred, culturally and socially appropriate way. This study also helped prioritise other patient and caregiver needs for future interventions.
Conclusion
Before providing an intervention, it is important to identify the needs, perceived acceptability, and potential barriers to providing that intervention to that specific patient population. Globally used intervention practices might be unacceptable to our population. This study helped to identify the perceived acceptability, barriers, and specific needs of people with SZ and their CG before introducing a mobile mental health application. The mobile application was generally acceptable to patients and CG, with younger and more educated participants showing higher acceptability. The insights from the study will be used to modify the intervention according to the requirements of specific patient populations. They will also help to design better interventions in the future.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The authors thank Professor V. L. Nimgaonkar and Dr Triptish Bhatia. The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of NIH or FIC, who had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication. We acknowledge Dr Ajithra M for her valuable input in the study design.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Obtained from Government Medical College, Palakkad (IEC/GMCPKD/02/2023/103/PKD) on 20/6/2023.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the project ‘Psychiatric Research Infrastructure for Intervention and Implementation in India (PRIIIA)’ (D43 TW009114; HMSC File No. 2019-7623 dated January 6, 2020), funded by the Fogarty International Centre, NIH.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.