
Abstract
The concept and definition of primary care have undergone various revisions since its use in 1961.
1
The World Health Organization has described Primary health care as
essential healthcare which is universally accessible to individuals and families in the community and provided as close as possible to where people live and work. It refers to care which is based on the needs of the population which is decentralized and requires active participation from the community and family.
2
The Institute of Medicine (IOM) also describes it similarly, stating primary care as accessible, comprehensive, coordinated and continual care delivered by accountable providers of personal health services. 3 The translation of this description into community healthcare service delivery through a decentralized approach in India was given by the Bhore Committee in 1946. 4 This has been a successful service delivery model in limited resource and inequitable distribution settings like India. This decentralized approach was also utilized in primary care delivery through non-specialists like Accredited Social Health Activists (ASHA), Auxiliary Nurse Midwives (ANM), Community Health Workers (CHWs), and Multi-Purpose Workers (MPW) through task shifting and task sharing.5, 6
Discussion
Mental health forms an indivisible and integral component of overall health. To take mental health care beyond the four walls of a hospital to the community, it is crucial to integrate mental health care with primary care. However, clear frameworks are not available to facilitate this process.7, 8 This involves understanding mental health through the lens and construct of primary care. 9 However, expanding primary care to mental health care has merits and challenges. The authors aim to give their viewpoints on what “primary” and “care” mean about mental health and the priorities, skills, and values proposed for defining them.
Describing Primary Mental Health Care: What Constitutes “Primary” in Primary Care?
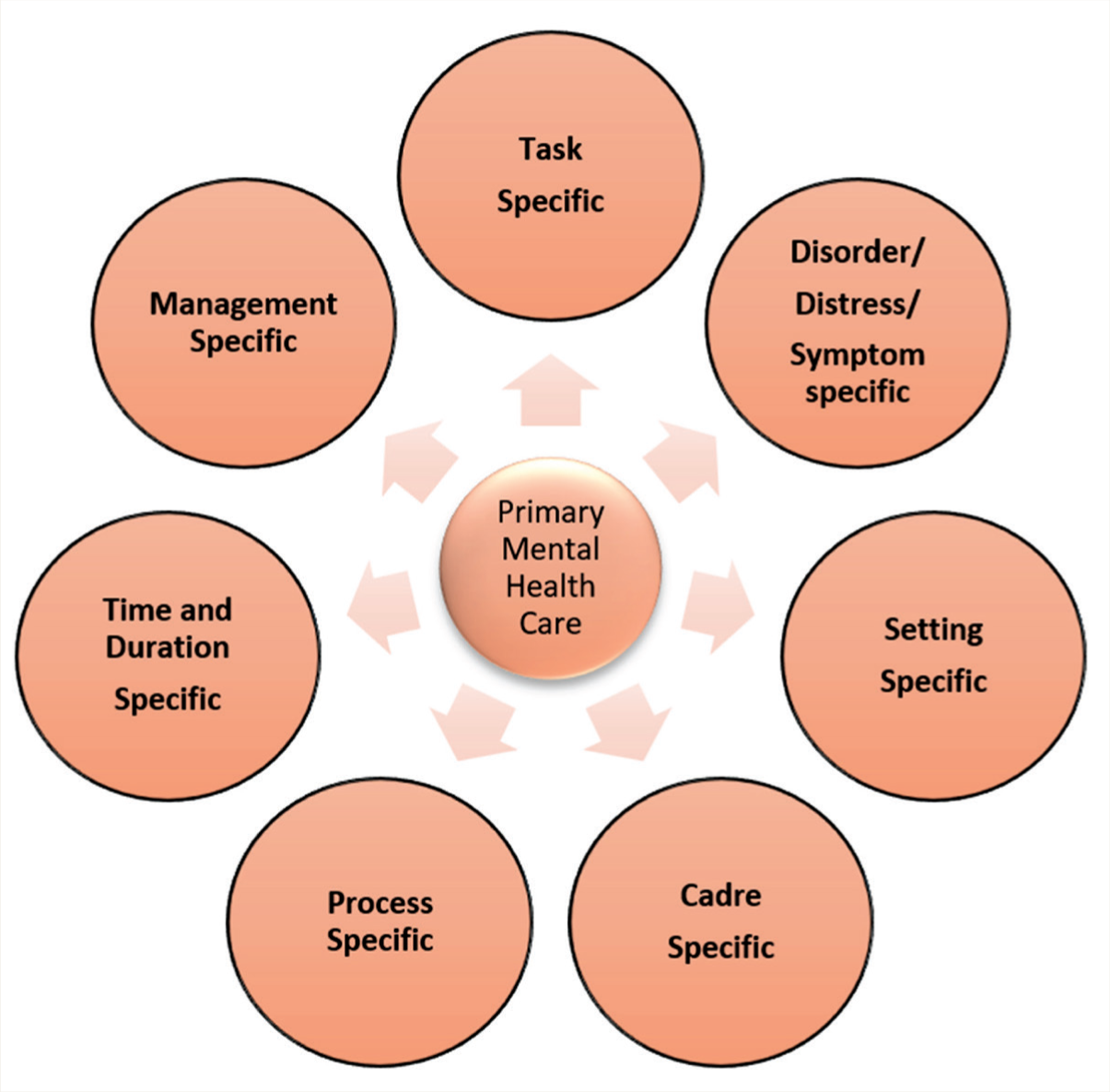
The concept of “primary” in primary care has been examined from various angles. Though it has been used commonly in a sequential approach, it encompasses a plethora of specific domains, including disorders, tasks, settings, time/duration, cadre, process, and management. Description of “primary” care in the context of mental health encompasses the following major domains, as shown in Figure 1.
Domains of Primary Mental Health Care.
Cadre Specificity
In this context, primary mental health care can be considered care delivered by non-specialist cadres, including primary care providers like medical officers, General Physicians, Family physicians, AYUSH practitioners, Accredited Social Health Activists (ASHA), and the relatively newer cadre of Community Health Officers (CHO).
Task Specificity
Task specificity in primary mental health care can refer to the tasks of identifying/screening, referring to care providers, and managing mental health disorders specifically. These tasks are specific across the cadres of service providers. At the level of ASHA workers, it can refer to the screening for mental illnesses utilization of standard, validated mental health screening tools like Symptoms in Others, 10 Patient Health Questionnaire (PHQ), 11 and MERIT, 12 psychoeducating the community about common symptoms of mental illness and ensuring they are on regular follow-up and encouraging people to seek help for mental illness. At the level of CHOs, the task specificity may be the identification, referral, and follow-up of patients with mental illness and refill of prescribed drugs. At the level of Medical Officer, the task specificity could be prescribing the first line of management for commonly prevalent and uncomplicated mental health disorders in the community who visit primary health centers. Validated tools like the Clinical Schedules in Primary Care Psychiatry for Doctors 13 and Nurses/CHOs have been developed to aid this process. 14
Disorder/Symptom/Distress Specificity
This approach considers primary mental healthcare delivery limited to specific symptoms or, more broadly, to specific disorders. This approach utilizes alternative ways of disorder classification than International Classification of Diseases for Mortality and Morbidity (ICD) 15 and Diagnostic and Statistical Manual (DSM) 16 like the trilateral transdiagnostic approach: Severe Mental Disorder (SMD) comprising of Psychosis and Bipolar Affective Disorder, Common Mental Disorder (CMD) comprising of Depression, Anxiety and Somatoform disorder, Substance Use Disorder (SUD) which includes predominantly management of alcohol and tobacco use disorders and Suicide. 13 Another approach advocated is the Trishul (trident) approach of mental wellness, mental distress, and mental illness. 17
Unlike medical diagnoses, psychiatric diagnoses can be challenging in primary care settings. In addition to the current presenting symptoms, a patient’s past history significantly influences the lifetime diagnosis, which can be difficult for a primary care provider to make. This can often lead to a different cross-sectional current diagnosis when compared to the longitudinal/lifetime diagnosis.
Another dimension to consider is the dynamic nature of psychiatric diagnoses. Psychiatric diagnoses are also known for their subjective variability. Despite the existence of standard manuals (such as ICD and DSM) for diagnosing psychiatric illnesses, achieving a consensus on psychiatric diagnoses remains a challenge, even for experienced psychiatrists. In addition, as time progresses, new symptoms may emerge, leading to a change in diagnosis. Because of these reasons, making a psychiatric diagnosis can be a difficult task for primary care professionals. To overcome this difficulty, primary care professionals can be encouraged to make broader domain-wise diagnoses (namely, severe mental disorders, common mental disorders, etc.) rather than striving for specific diagnoses, which generally require teasing out of symptoms and other information. Additionally, the focus can be on the first-line management of presenting symptoms and prompt referral to tertiary care for further management.
Time and Duration Specificity, Continuity of Care
Time specificity describes primary mental healthcare as provided at presentation time, irrespective of the setting. This is akin to the first aid provided. Another aspect of mental healthcare delivery is longitudinal care compared to cross-sectional interventions in other specialities. Hence, “when” and “how long” care are relevant in this context. Hence, longitudinal care in primary mental health care delivery becomes pertinent with regular follow-ups of patients.
Setting Specificity
A pragmatic approach in primary mental health care delivery is defining the setting. The care delivered at the level of Aayushman Aarogya Mandirs (earlier named Health and Wellness Centers/Sub-Centers) and Primary Health Centers is considered primary care. However, the word setting is most often used interchangeably in the context of service availability (e.g., primary care setting). This describes the “where” in primary mental health care. A debatable angle to setting specificity includes the care received at Taluk Hospital/block-level hospital settings, where specialist care is available. This also overlays the cadre specificity angle to the setting.
Management Specificity
This domain describes the “what” in primary care. In the realm of primary care, the focus lies on understanding the diverse treatment modalities tailored to address various mental illnesses. Such treatment approaches encompass pharmacological and non-pharmacological interventions, each uniquely suited to different conditions and individual needs, and can be administered by different healthcare professionals. The realm of pharmacological interventions presents a complex landscape where the benefits and potential side effects of psychotropic medications necessitate careful consideration and a nuanced evaluation of risk versus benefit. Meanwhile, non-pharmacological interventions offer a spectrum of options ranging from educating to brief counseling and supportive therapy, providing patients with mental illnesses avenues to navigate and overcome their distress.
In this regard, primary care could be considered a specific mono-therapeutic pharmacological and low-intensity psychosocial intervention that alleviates distress and symptom severity. Guidelines on which drugs could be prescribed in primary care management for what conditions, how long, and which non-pharmacological interventions can be used constitute the management specificity.
Process Specificity
Unlike Management Specificity, which deals with “what,” this domain describes the “how” in primary care. Process specificity refers to how the care is delivered, that is, in-person v/s tele mode of delivery, home visits, proxy consultations, collaborative consultations with specialists, cultural integration through liaison with faith healing, and alternative care approaches. This also deals with accountability, legal liability, policy, and administration-level decisions for primary mental healthcare delivery. In primary care settings, all the above can be easily construed as part of primary mental healthcare, particularly teleconsultations, proxy consultations, collaborative care, and home visits.
Describing Primary Mental Health Care: What Constitutes “Care?”
Kates et al. (2018), 18 define primary mental health care as the one which encompasses mental health services provided by primary care providers, eliminating the need for direct involvement of mental health professionals.
The provision of primary mental health care transcends NOT merely treating mental illnesses and instead encompasses a broad array of approaches aimed at effectively addressing patients’ distress. Collaboration among professionals from diverse fields, including alternative medicine practitioners, religious healers, and various personnel within Primary Health Centers (PHCs), plays a crucial role in this holistic approach.
Within this context, “care” entails culturally appropriate interventions tailored to promote mental well-being, prevent mental disorders, and offer accessible treatment alternatives. Primary mental health care is delivered at individual, family, and community levels, employing low-intensity psychosocial interventions19–21 and mindfulness techniques in conjunction with largely mono-therapeutic pharmacological interventions to support individuals with mental illnesses. Following up, stable cases can also happen under primary mental health care.
Sequential Versus Parallel Care
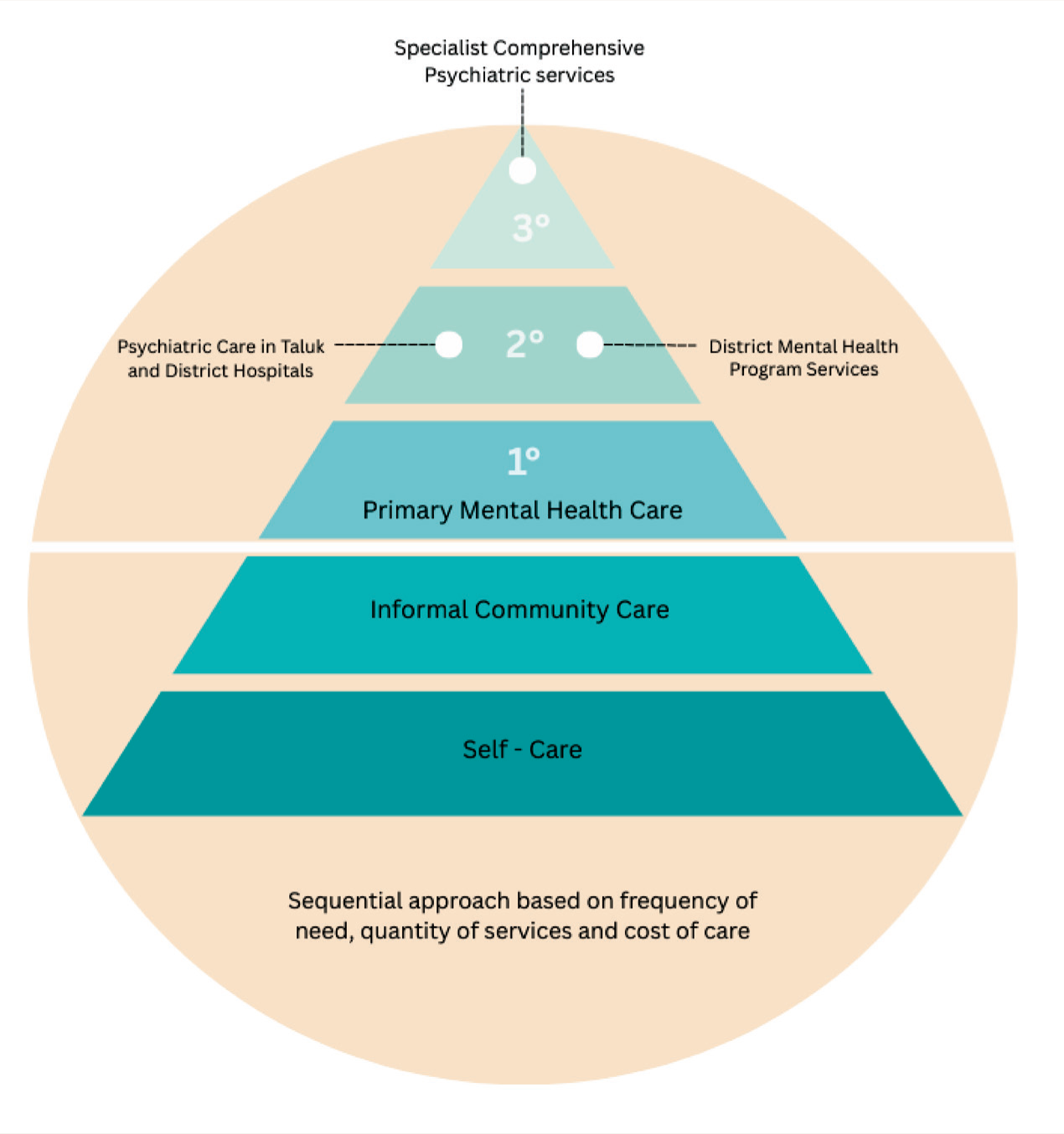
Scientific literature mentions help-seeking pathways, 22 especially in people seeking mental health services. In the World Health Organization pyramid, primary care comes third after informal services as shown in Figure 2.
Care Pyramid (Reference: Figure 4.1: WHO Service Organization Pyramid for an Optimal Mix of Services for Mental Health, Source: Mental Health in Transition: Assessment and Guidance for Strengthening Integration of Mental Health into Primary Health Care and Community-Based Service Platforms in Ukraine, World Bank, 2017). 23
However, in mental health, integrating alternative approaches through a parallel model of care, rather than a purely sequential one, has become increasingly necessary. 24 While sequential care involves patients moving from one service to another linearly, parallel care allows for the simultaneous engagement of multiple treatment modalities, including medical, psychological, social, and alternative approaches such as yoga and mindfulness therapies.25, 26 This model is particularly effective in mental health, where complex conditions often require a multifaceted approach. Parallel care facilitates family and community involvement, recognizing their crucial roles in providing support, Continuity, and a sense of belonging, which are essential for recovery. It also allows concurrently addressing different aspects of a patient’s well-being, leading to more comprehensive and sustained outcomes. 27 By engaging family members and community resources in parallel with professional treatment, this model helps to create a more resilient support system, ultimately enhancing the effectiveness of primary care in mental health settings. 28
Integrating Alternative Approaches, the Role of Family and Community in Primary Care
Specifically, in LaMIC countries, integrating alternative approaches to care plays a major role in the acceptability of mental health service delivery. Similarly, care is also facilitated by the family and community through filial piety in a socio-cultural context. 29 Hence, approaches like Dava-Dua (integration of faith healing and pharmacological approaches) 30 and caregiver-inclusive care approaches 31 are needed to define “care” in primary mental health care.
Operationalizing the Definition of Primary Mental Health Care
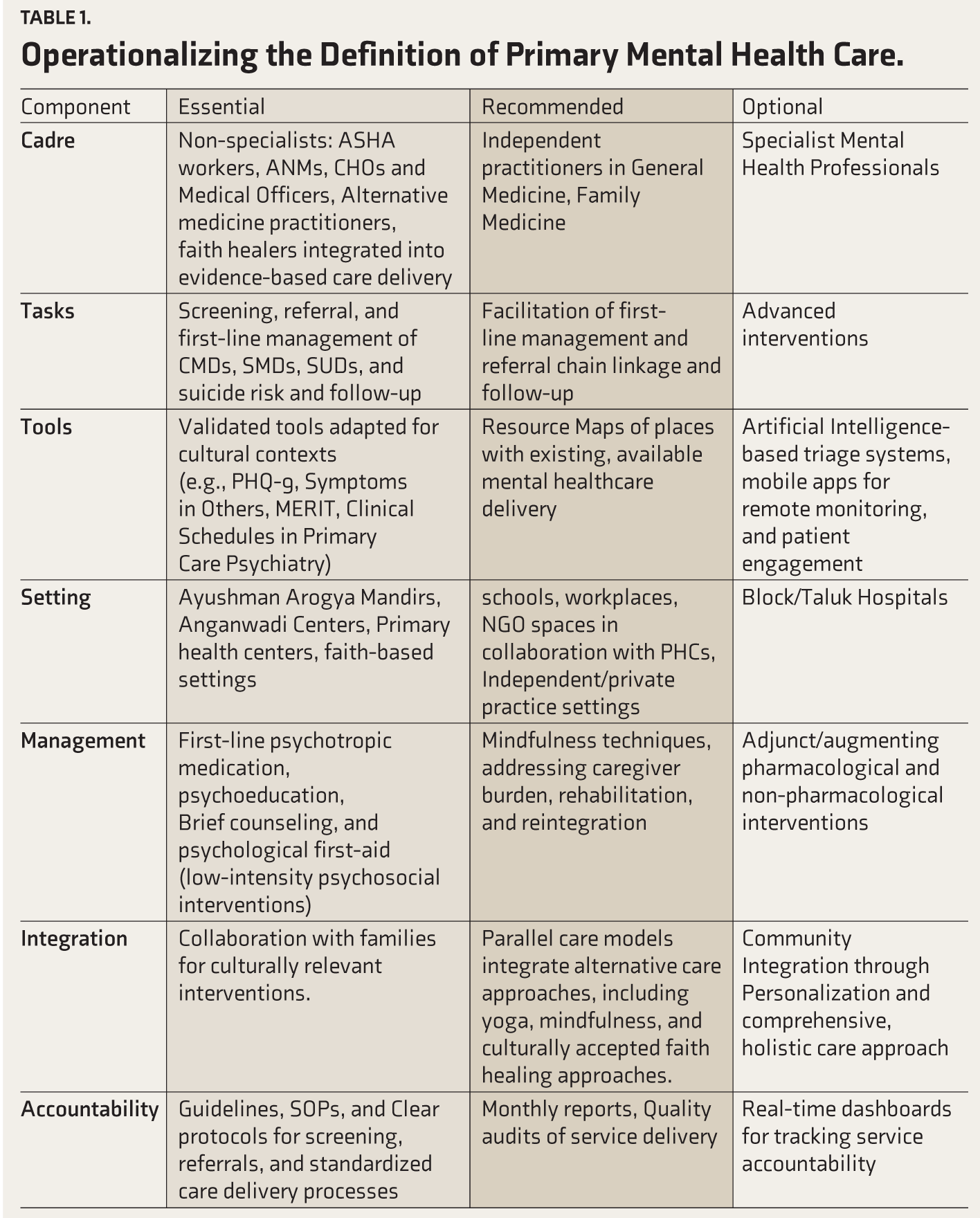
To operationalize the definition of primary mental health care, mental health needs to be viewed from the angle of primary care, and primary care has to be viewed from the point of mental health. Considering the need for operationalizing the definition, concept, boundaries, and expectations of primary mental health care, flexibility and modularity in defining primary mental health care are suggested. An attempt at operationalizing this is described in detail in Table 1.
Operationalizing the Definition of Primary Mental Health Care.
Limitations
Though this article attempts to operationalize the definition of primary mental health care, the authors acknowledge that these are viewpoints of mental health professionals. Although thoughts from people involved in primary care delivery have been duly considered, the authors are open to the possibility of a different viewpoint from people involved in primary care delivery.
Conclusions
Defining and operationalizing the concept of “primary mental health care” is a nuanced and evolving process that must balance public health priorities, contextual relevance, and system capacity. In this regard, developing an operational framework shall provide insights for policymakers, program designers, and health system stakeholders aiming to strengthen mental health integration within primary care. A consensus-driven, context-specific, and modular definition, which is dynamic, flexible, and culturally appropriate, has been attempted. This facilitates standardization where feasible and encourages innovation and customization to address diverse population needs across varied service delivery settings.
Footnotes
Acknowledgements
Same as the “Introduction ” article of this issue (Indian J Psychol Med. 2026;48(1 suppl)).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Channaveerachari Naveen Kumar is the Principal Investigator of this project and supplemental issue. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Declaration Regarding the Use of Generative AI
In the preparation of this work, the author(s) utilized ChatGPT for only table generation assistance. After employing this tool, the author(s) carefully reviewed and edited the content as necessary and take(s) full responsibility for the final publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This viewpoint is a result of funding under the research project “Multistate digitally driven capacity building program for primary mental healthcare” funded by the CSR initiative of a multinational company.