
Abstract
Background
Specific learning disorder (SLD) is a neurodevelopmental disorder where an individual experiences persistent difficulty in learning and using academic skills for at least six months despite interventions targeted at addressing these challenges. 1 The prevalence of SLD ranges from 2% to 10%, with dyslexia being the most common type. 2 A meta-analysis of Indian studies showed the pooled prevalence of SLD in India to be 8%. 3 Significant gender differences are noted to exist, with boys being more frequently affected by the condition than girls. 4 Essential features of SLD include ongoing struggles with fundamental academic skills, such as impairments in reading, written expression, and mathematics. Diagnosis involves standardized achievement measures and comprehensive clinical assessment. While the learning difficulties may emerge during school-age years, they may become fully apparent only when academic demands surpass the individual’s capabilities. 1
The Government of India recognized SLD as a disability in 2016 through the gazette notification released on December 28, 2016. 5 The implementation of the Rights of Persons with Disabilities (RPWD) Act, 2016, introduced legal obligations to adhere to specific assessment and certification guidelines outlined in the act. 5 This has led to some practical difficulties in routine clinical practice. This article focuses on the challenges and opportunities in the SLD assessment and certification process in India.
Discussion
There are issues inherent to the construct of SLD described in the diagnostic manuals and the current certification processes under the RPWD Act (2016, amended in 2024). 6 The authors discuss ten challenges that arise with SLD in the current Indian context and our recommendations for overcoming these challenges.
Challenges
Diagnosis: While diagnostic manuals discuss learning disorders, the RPWD Act, 2016 specifically addresses learning disability and their assessment. Conceptual differences (disorder vs. disability) with regard to SLD exist among various diagnostic guidelines and the RPWD Act. 7 Many definitions of SLD, whether exclusionary or inclusionary, often mention terms such as adequate intelligence, appropriate instruction, and sociocultural factors. However, standardizing these criteria proves challenging in a pluralistic society like India, where diverse cultural, linguistic, and socioeconomic factors can significantly influence educational outcomes and the assessment of learning difficulties. 8
Standardization of assessment tools: The tools approved for SLD assessment under the recent notification of the RPWD Act include the NIMHANS (National Institute of Mental Health and Neurosciences) Battery and the Grade Level Assessment Device (GLAD).9–10 The NIMHANS Battery was initially standardized for the 7th grade/standard (approximately up to 14 years of age), but the updated version includes test items up to the 10th grade. It is available in English, Kannada, and Hindi but is copyrighted. 11 The GLAD can be used from the age of six years for grades I to IV and is available in English and Hindi, covering mathematics as well. 8
However, according to the RPWD Act, SLD assessment and certification should be conducted for children aged eight years and above, with repeat certifications during class X and class XII. 6 The recent guideline also mentions that these tools will be used across all ages, and a certificate issued at 18 years or more will be valid for a lifetime. Currently, there is a lack of assessment tools for SLD beyond grade X. 12 This poses a challenge for older children and adults as we do not have a scale that is currently standardized for them. Another challenge that arises is that the tools such as the NIMHANS battery and various intelligence quotient (IQ) tests currently approved to use as per the recent gazette notification are copyrighted. There should also be clarity regarding how these tools will be purchased and who will provide the funding till new assessment tools are developed.
Language issues: The multilingual social context of India presents a special challenge, as there is a scarcity of assessment tools available in different languages that adequately address the unique characteristics of each language. 13 Additionally, in the Indian context, children may have difficulties in one language, which usually would be the second or third language, but might not have difficulties in the first language. This is because, in general, all subjects are mainly taught in the first language (medium of instruction), and hence, a child would have received maximum training in that language. Sometimes, children who are trained in their vernacular languages in smaller classes face difficulties when they are introduced to English later during their higher education. 11 For example, a child who has Hindi as his/her mother tongue and who studied in a Hindi medium school might have SLD in English. Similarly, a child who has done his schooling in an English medium school might have difficulties in their vernacular languages. This aspect has not been taken into consideration in the law and places huge challenges.
Human resources: The RPWD disability assessment includes screening for children, with a screening committee headed by the school principal and a screening questionnaire administered by teachers in both public and private schools when children reach eight years of age or class III, whichever comes earlier. Diagnosing SLD post-screening necessitates initial evaluation by a pediatrician, followed by assessment by a psychiatrist to rule out comorbidities, and later specific psychometric tests, including IQ assessments, conducted by a psychologist. 6 In a country where there is already a shortage of psychiatrists and psychologists, the availability of qualified human resources presents a significant challenge. 14 However, the provision to include private medical practitioners as a board member is a welcome step.
The shortage of special educators in India is another significant challenge. While the Central Board of Secondary Education (CBSE) mandated the appointment of special educators in affiliated schools to support children with learning disabilities, many schools struggled to find qualified professionals in this field. School authorities have noted that while special educators may have experience in teaching physically challenged students, they often lack the theoretical and practical skills required to support students with learning disabilities effectively. 15
Remedial measures: The diagnosis of SLD under the RPWD Act necessitates ensuring that the child has had adequate opportunities for learning and that proper motivation is provided to them. Only if the child remains unable to perform despite these provisions, a diagnosis of SLD can be made. This poses problems in the Indian context. First, assessing whether adequate opportunities and remedial measures were indeed provided to the child is difficult. Second, there are concerns about the competence of the current education system in delivering such remedial measures effectively. 16
Lack of awareness: Parents and school teachers not being aware of the condition remain to be a problem. The presence of multiple curriculums, varying standards, and multilingualism further complicates matters, making it difficult to implement a unified, standardized approach. Certificates become significant primarily when exemptions and concessions in schooling are necessary. Each educational board offers various supports, including exemptions from second and third languages, additional time, scribe support for writing, provision of calculators, and more. However, there is a lack of uniformity in the assessment and certification processes across different boards, let alone alignment with the RPWD guidelines. 17 The new gazette notification also mentions that if a child screens positive for SLD, the teachers shall interview the parents to assess their motivation. If motivated, the child will be referred for further assessment. 6 What if the child comes from a family background where his parents lack understanding and motivation? We also should consider whether the stigma and discrimination associated with labeling the child with a “mental illness” would lead to refusal to take consultation.
Children with borderline intelligence: As per the recent gazette notification under the RPWD Act, SLD can be diagnosed only if the IQ score is more than 85. The benefit of intellectual disability (ID) is received for individuals with IQ scores less than 70. What about the individuals who fall between the two? Despite having difficulties in learning, they are not eligible for benefits under either SLD or ID. Another challenge is that standard IQ scales consider an IQ score of 90–110 to be average, 80–89 to be low average, and 70–79 to be borderline. So, why a cutoff score of 85 is kept is also unclear. The current guideline also fails to address benchmark disability and the percentage of disability assessment in SLD.
Research and funds: There is a scarcity of high-quality, methodologically sound, population-based epidemiological studies in this area in India. There is a pressing need for large-scale population-based surveys in India that utilize appropriate screening and diagnostic tools. 3
Misuse: Some authors have also noted that the demand for SLD certificates has surged disproportionately in urban areas. Both parents and teachers seek to access the benefits of SLD certificates, regardless of the actual level of disability experienced by the child. Many professionals have started capitalizing on this surge by charging hefty amounts for assessments that impose a significant financial burden on parents. 18
Reservation versus accommodation: There is evidence that intensive remediation over an extended period can significantly reduce symptoms of SLD. One of the key characteristics of children with SLD is that many of them, with additional time and support, can eventually improve their reading, spelling, or mathematical abilities. 11 This may lead to situations where it becomes challenging to determine whether the child still qualifies for having a disability. This raises the question of whether it is appropriate to continue providing benefits associated with disability status to these children or if the focus should shift more towards accommodating their needs. Additionally, given that up to 15% of children will have learning disorders, considering it as a benchmark disability can lead to many challenges in the future once more people start availing of such benefits, and it would even lead to a possibility of people with other benchmark disabilities being undermined.
Recommendations
Consensus guidelines in India recommend a basic intervention approach to manage SLD. It focuses on the interpretation of evaluation reports, the description of specific skills that may be delayed, and the identification of comorbidities. Intervention should then be interdisciplinary and individualized for each child. Remedial education stands as the cornerstone for the treatment of SLD. 19 The current RPWD assessment guidelines fail to address the diversity present within SLD adequately. There is a need to recognize that all children with learning issues and low average performance do not have SLD. Every child is different, and similarly, every child’s performance in terms of reading, spelling, and writing can be different. One should consider the uniqueness of the child and perform a holistic assessment to diagnose learning disability. There is a crucial need to develop individualized, tailor-made teaching strategies, and materials for each child. 17
We have proposed ten recommendations that should be considered without delay:
A task force to be formed that includes psychiatrists, psychologists, pediatricians, members from various nongovernmental organizations actively involved in the field, and members from the legal fraternity who can act as a policy guide to the government. It is crucial to bring these challenges associated with diagnosis, assessment, certification, and management of SLD to the attention of policymakers. There is a need for a standard definition removing all ambiguities, and the diagnosis should be more longitudinal, based on school records rather than cross-sectional. There is an urgent requirement to upgrade existing assessment tools to cater to the needs of children in secondary classes and beyond. The development of new, easily adaptable tools, preferably digital, must be initiated without delay. Assessment methods should not be limited to diagnosis and certification but should also provide valuable information for planning support measures, including remediation and rehabilitation.
20
Such tools should be made freely available for the assessment process. Remedial tools should also be made available in all languages and based on difficulty level. There is a need for good-quality epidemiological studies, both cross- sectional and longitudinal, using standardized definitions and assessment tools. Studies should also investigate the remedial measures currently provided in our country, as well as their effectiveness and practicality.
12
There is also a need to develop tools that are validated in all regional languages. Individuals should be assessed in languages in which they are having difficulties and not necessarily the mother tongue or medium of instruction. There is a need to increase the workforce to include qualified and specially trained professionals to assess and diagnose SLD and provide remedial measures within the school. The nonavailability of trained professionals should not be used as an excuse to allow other nonprofessionals to take over such responsibility. Rather, the focus should be solely on increasing the number of qualified professionals. Standardizing diagnostic procedures and establishing consistent systems of practice across India are crucial for maintaining uniformity across the country. This standardization ensures that children receive consistent and equitable assessments regardless of their location. Additionally, uniform provisions across all educational boards and entrance examinations would facilitate a seamless transition for children with SLD across different boards and institutes, ensuring they receive appropriate accommodations and support wherever they go.15–16 Addressing the challenges related to remedial measures requires careful evaluation of educational practices and interventions, as well as collaboration between educators, parents, and healthcare professionals to ensure the best possible support for children with learning difficulties. Additionally, the introduction of the new National Education Policy with its holistic approach, encouragement for regional languages, vocational push, and digital integration on outcomes for students with SLD remains to be seen. Incorporation of technology with assistive devices like voice recognition programs, recording devices, word processors, and various educational apps is helpful. Many forms of technology can help individuals with learning disabilities capitalize on their strengths and bypass or compensate for their disabilities. Increasing awareness about SLD among parents, teachers, and schools is crucial as it encourages early identification of the condition. This proactive approach can help save children from the academic struggles they face before their SLD is diagnosed, and it enables them to access early interventions. By fostering a better understanding of SLD and its signs, caregivers, and educators can provide timely support, leading to improved academic outcomes and overall well-being for children with SLD.
16
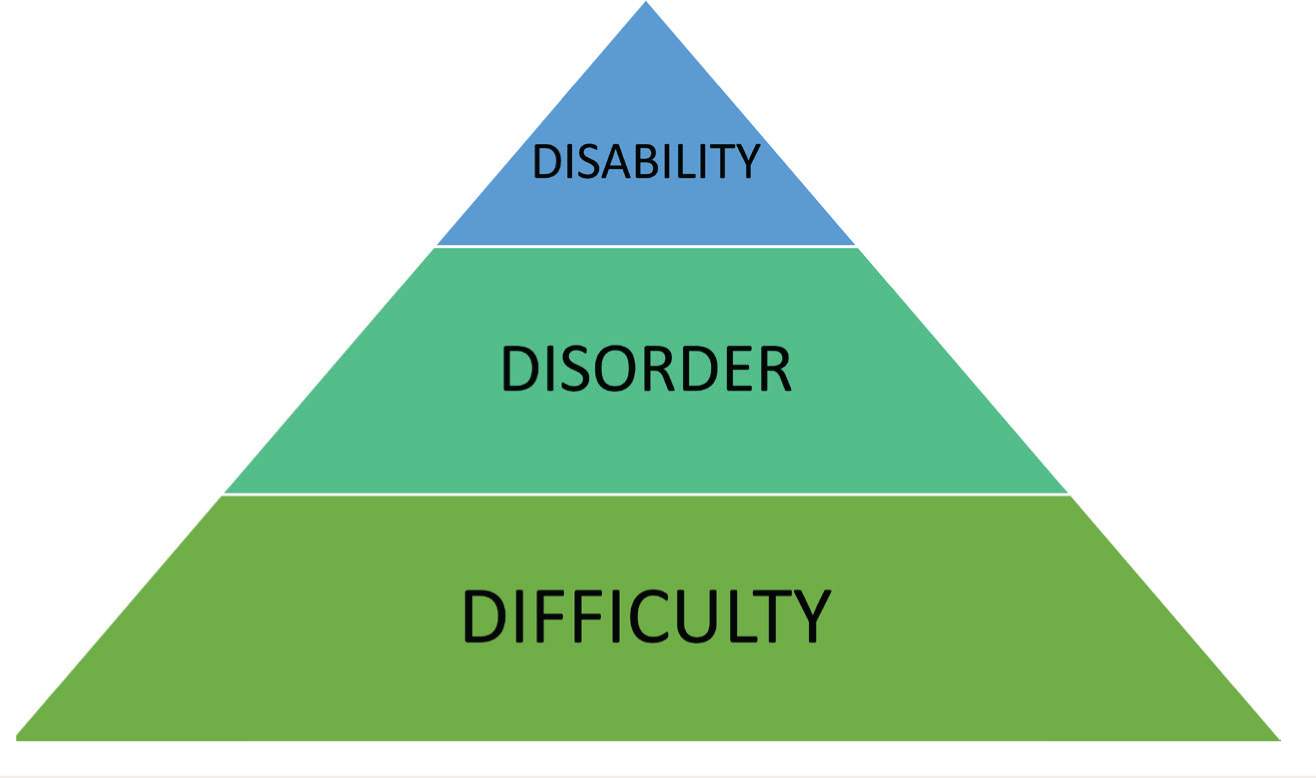
There is also a need for early symptom recognition and remedial intervention. This should ideally start earlier than eight years, preferably from the first standard in schools. Programs must be implemented where at least one teacher is identified and trained for early recognition of symptoms as well as to enforce adequate remedial measures. Individuals with borderline IQ are a group who are being left alone without any assistance despite having significant learning difficulties. Whether they should be included in SLD if they are having learning difficulties must be decided. The IQ cutoff score, if being used, should be 90, or specific cutoff scores based on each scale should be mentioned. The task force should also address the group with IQ scores of 70–90, and a separate care plan must be prepared for them. The option for the detailed assessment of SLD after the screening only if the parents are motivated should be removed. It should be made imperative for the parents to take the child for detailed, if necessary, repeated assessments and remedial measures. Rehabilitation institutes should be tasked with coming up with guidelines for the support needs of children with dull normal and borderline intelligence in academics, semi-skilled jobs training, and support needs. To address the debate between disorder and disability, the authors suggest a new perspective on SLD. We propose categorizing individuals with SLD into three groups: a larger group with general learning difficulties, a subset with a diagnosable learning disorder, and an even smaller subset with a learning disability (Figure 1). Individuals with learning difficulties should be identified as early as possible in school and be provided with remedial intervention at the school level. The children who, despite remedial measures from school, persist in having difficulties should be referred to specialists for the evaluation for learning disorders. Those diagnosed with a learning disorder should then receive tailored professional interventions. Finally, the small subset of individuals who, despite all professional interventions, still struggle significantly should be assessed for a learning disability. Additionally, the recent gazette notification has not mentioned the benchmark disability in SLD or how to assess the percentage of disability under SLD. However, an earlier notification dated December 09, 2020, stated that “any person having tested positive on NIMHANS Battery shall be considered as a person with benchmark disability, that is, disability of more than 40%”. Whether the same can be applied has to be clarified at the earliest.
The decision regarding benefits and accommodations for children with SLD should be based on a comprehensive understanding of their individual needs and capabilities. It may be beneficial to reassess their situation periodically and adjust support measures accordingly. Additionally, focusing on providing appropriate accommodations, such as additional time or specialized instruction, can help these children succeed in academic and social settings while minimizing the stigma associated with disability status. Ultimately, the goal should be to ensure that all children, regardless of their learning challenges, have access to the support and resources they need to thrive.
Categorization of Individuals with Specific Learning Disorder.
Conclusion
SLD is a neurodevelopmental disorder characterized by significant challenges in academic performance. Recognized as a disability under the RPWD Act in India, addressing issues related to its definition, assessment, and certification remains a critical concern. There is an urgent need to decentralize the assessment process and develop adaptable, culturally, and linguistically inclusive tools, preferably digital, for improved accessibility. There is also a pressing need to raise awareness, train skilled professionals, and ensure the availability of adequate remedial measures. Until such measures are implemented, the emphasis should shift from focusing solely on disability and reservations to fostering an enabling environment and providing adequate accommodations for individuals. Additionally, raising awareness among policymakers and other key stakeholders about these challenges is of paramount importance.
Footnotes
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
Grammatical corrections were made using the generative artificial intelligence (AI) tool (ChatGPT). We assume full responsibility for the manuscript’s content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.