
Abstract
To the Editor,
The Jefferson Scale for Physician Empathy-Health Professionals (JSPE-HP) is widely used to measure self-rated empathy. 1 The JSPE is a 20-item instrument with each item rated on a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree). Half the items are reverse scored. Higher scores indicate higher levels of empathy. 2 Separate versions have been developed for health professionals and students. Despite being widely used, the factor structure of the JSPE has not been studied by Indian health professionals. It is unclear whether the theoretical concept of “physician empathy” has latent factors similar to the populations where the instrument was developed.
We did an exploratory factor analysis of JSPE scores in a sample of Indian health professionals to address this lacuna. Several methods have been described to decide the number of retained factors in factor analysis.3,4 We developed models using three different approaches (Kaiser’s criteria, scree plot, and parallel analysis) and compared them. We analyzed data from a cross-sectional observational study carried out between December 2015 and July 2016 in faculty in a medical college in South India. 5 The Institutional Ethics Committee approved the study. All faculty members of designations Assistant Professor and above who were not on extended leave were invited to participate. Informed consent was taken from all participants. Details of the sample and significant associations are available in the literature. 5 We used SPSS version 16 for statistical analysis 6 and checked the suitability of data using the Kaiser–Meyer–Olkin (KMO) test and the Bartlett test for sphericity. An exploratory factor analysis was done using principal component analysis with an orthogonal rotation on the 20 items of the JSPE-HP. We used a web-based engine to do parallel analysis. 7 Factor loadings with a value of more than 0.4 were interpreted. We calculated Cronbach’s alpha for each factor.
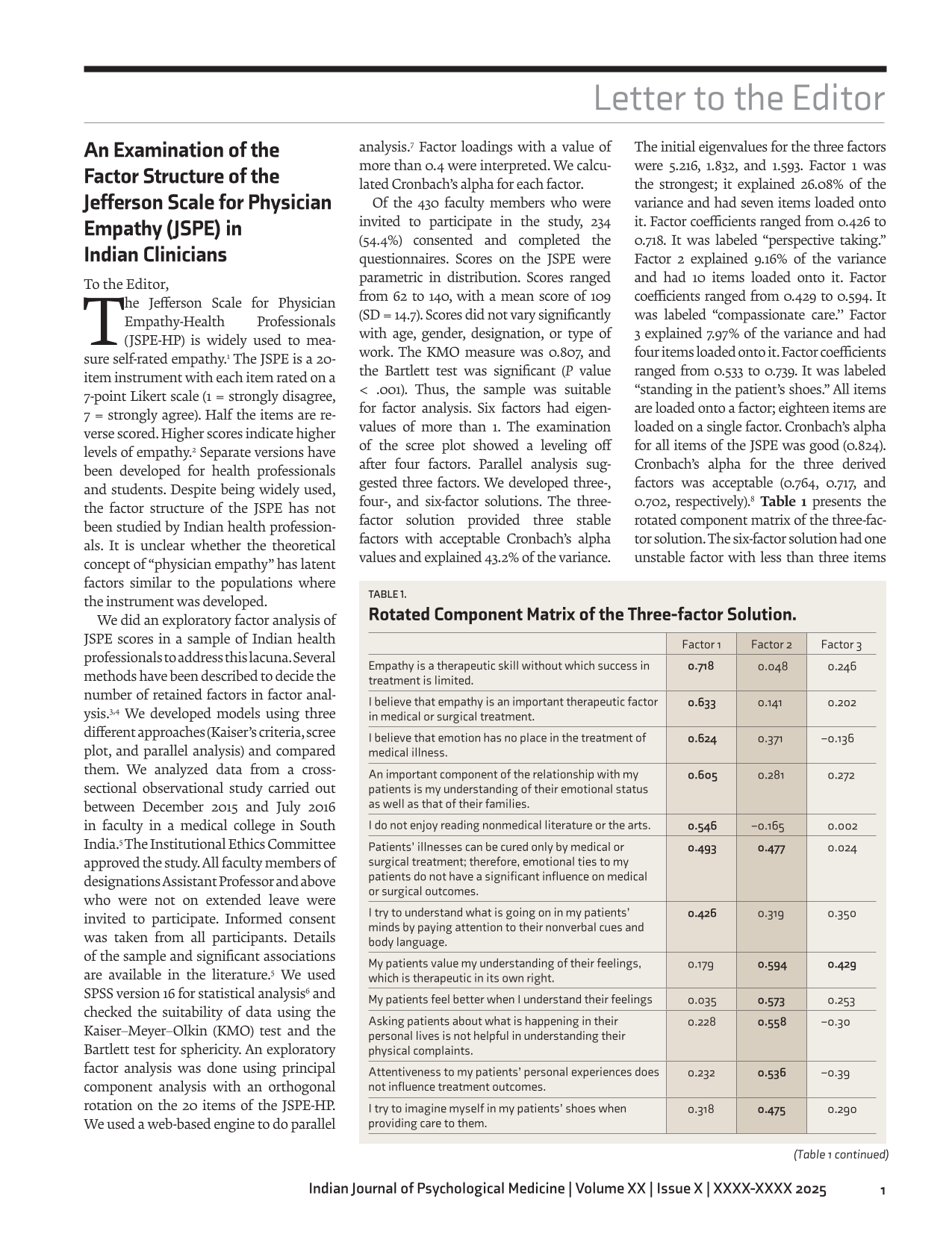
Of the 430 faculty members who were invited to participate in the study, 234 (54.4%) consented and completed the questionnaires. Scores on the JSPE were parametric in distribution. Scores ranged from 62 to 140, with a mean score of 109 (SD = 14.7). Scores did not vary significantly with age, gender, designation, or type of work. The KMO measure was 0.807, and the Bartlett test was significant (P value < .001). Thus, the sample was suitable for factor analysis. Six factors had eigenvalues of more than 1. The examination of the scree plot showed a leveling off after four factors. Parallel analysis suggested three factors. We developed three-, four-, and six-factor solutions. The three-factor solution provided three stable factors with acceptable Cronbach’s alpha values and explained 43.2% of the variance. The initial eigenvalues for the three factors were 5.216, 1.832, and 1.593. Factor 1 was the strongest; it explained 26.08% of the variance and had seven items loaded onto it. Factor coefficients ranged from 0.426 to 0.718. It was labeled “perspective taking.” Factor 2 explained 9.16% of the variance and had 10 items loaded onto it. Factor coefficients ranged from 0.429 to 0.594. It was labeled “compassionate care.’’ Factor 3 explained 7.97% of the variance and had four items loaded onto it. Factor coefficients ranged from 0.533 to 0.739. It was labeled “standing in the patient’s shoes.” All items are loaded onto a factor; eighteen items are loaded on a single factor. Cronbach’s alpha for all items of the JSPE was good (0.824). Cronbach’s alpha for the three derived factors was acceptable (0.764, 0.717, and 0.702, respectively). 8 Table 1 presents the rotated component matrix of the three-factor solution. The six-factor solution had one unstable factor with less than three items loading onto it and one item not loading strongly onto any factor. The four-factor solution was stable, but only three factors had acceptable values for Cronbach’s alpha. Thus, we found a three-factor solution to best fit the JSPE scores in this sample of Indian clinicians. A three-factor structure for the JSPE is the most consistently reported in the literature across cultures. 9 The factor structure was similar to that previously reported by Hojat et al. 2 Thus, we used the same labels they suggested.
Rotated Component Matrix of the Three-factor Solution.
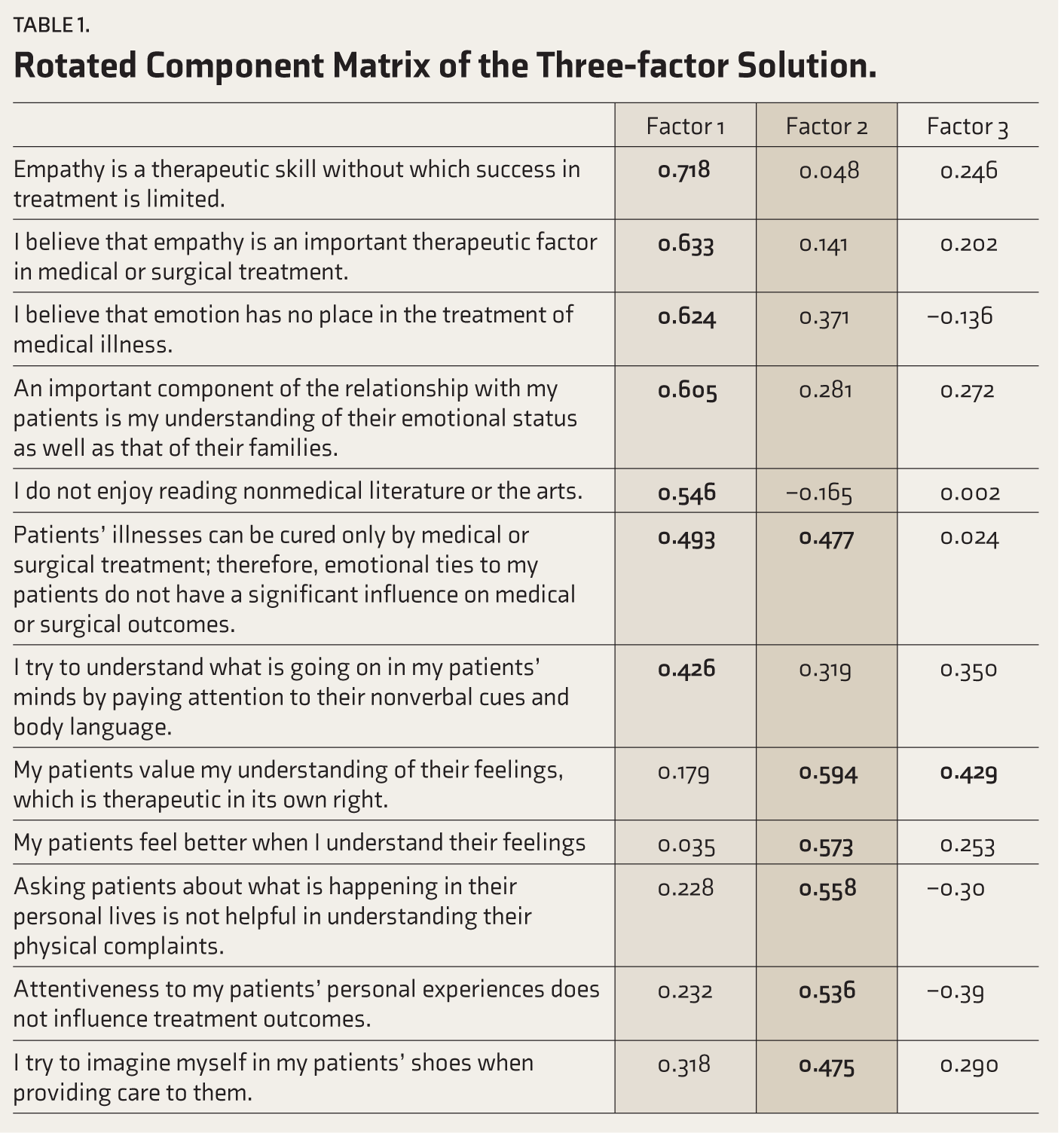
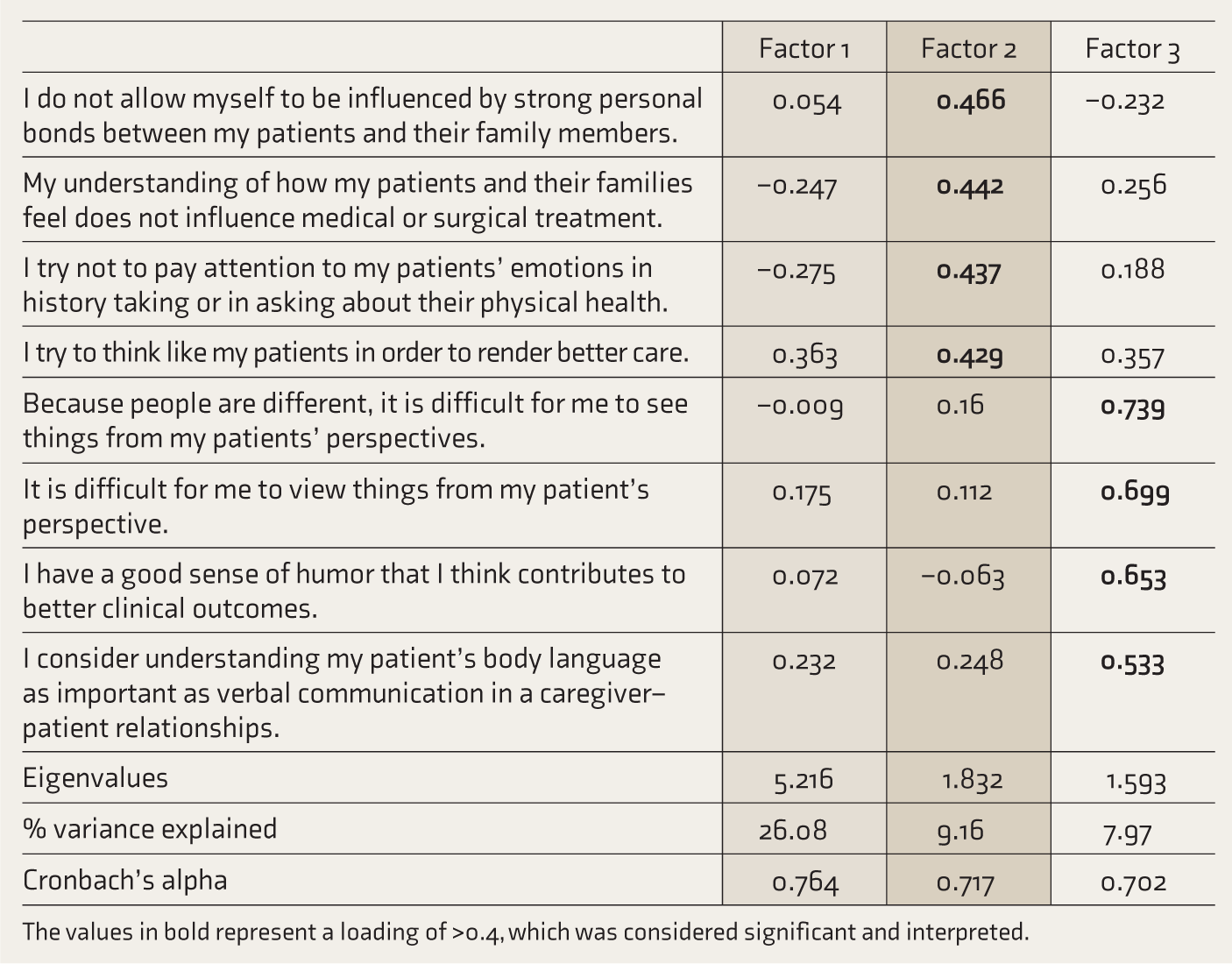
The values in bold represent a loading of >0.4, which was considered significant and interpreted.
This study is a secondary analysis of data collected in 2015–2016. However, the point of collection of data would not impact the validity of the presented psychometric analysis. We did not collect data on the cultural or linguistic backgrounds of the participants or how they impacted the scores. A modest response rate limits this study. It adds to the growing consensus that parallel analysis is a superior method of deciding the number of factors in factor analysis. 10 It supports the cross-cultural validity of the JSPE and substantiates a stable three-factor structure for the JSPE in Indian clinicians.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Data Availability
The data used in this study are not available in a public data repository.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The study was cleared by an Institutional Ethics Committee (Minute No. 9724) dated November 10, 2015.
Informed Consent
All participants gave a written informed consent before being included in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded through an internal FLUID grant (minute num. 9724).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.