
Abstract
Background:
Childhood mental disorders are a major global concern, particularly in India. Despite efforts to establish child psychiatry services, the treatment gap persists. This study investigates referral patterns, pathways to care, and diagnostic trends among children attending a child psychiatry unit (CPU).
Methods:
A retrospective chart review (2017–2022) was conducted at the CPU of Kasturba Medical College, Manipal. Two investigators analyzed 1,046 files, extracting data on demographics, pathways to care, reasons for referral, and diagnoses. Inter-rater reliability was confirmed, and associations between pathways to care, diagnosis, and demographics were examined.
Results:
This study included children with a mean age of 11.2 years, predominantly male (63.2%). Most children (97.5%) first sought care from a healthcare provider, with 29.3% consulting mental health professionals (MHPs) and 59.6% visiting medical specialists. Primary reasons for referral included behavioral disturbances, emotional disturbances, and academic decline. Common primary diagnoses were attention deficit hyperactivity disorder (16.5%), mental retardation (14.7%), and pervasive developmental disorder (12.6%). Significant associations were found between pathways to care and diagnosis (P = .001), as well as between gender and both referral reasons (P < .001) and diagnoses (P < .001).
Conclusions:
The study provides insights into the demographic and clinical characteristics of children with mental health problems in India. The medical model of care pathways is a positive shift, and these findings can guide gender- and culture-sensitive service planning, optimize resource allocation, and inform future research in child psychiatry.
Keywords
The majority (97%) of children and adolescents sought initial help from healthcare providers. Behavioral disturbances, emotional disturbances, and academic decline were the most common reasons for referral. Common primary diagnoses were ADHD, mental retardation, and PDD.Key Messages:
The World Health Organization (WHO) estimates that approximately 20% of children experience some psychiatric disorder. 1 In India, studies have found a prevalence of childhood mental illness of 6.5% in the community, rising significantly to 23.3% among school-going children. 2 At any given time, approximately 50 million Indian children are affected by mental health problems, with this number projected to increase. 3 Notably, half of all major psychiatric disorders begin during childhood and adolescence. 4 These findings highlight the need for effective mental health services for children and adolescents. The rising burden of childhood disorders, coupled with increased mental health service utilization by this age group, calls for the development of specialized mental health services. 5 Unfortunately, the unmet need for such services remains substantial, with at least half of affected children not receiving timely care. 5
Many countries have initiated the development of child and adolescent mental health policies, which are implemented by establishing dedicated psychiatry services for individuals below 18 years of age. 6 However, a recent survey across 44 countries revealed that many nations did not have separate child and adolescent psychiatry services or departments.7,8 To address the shortage of trained specialists in the field, several countries have introduced dedicated residency programs in child and adolescent psychiatry. Despite these efforts, the number of trained professionals remains insufficient to meet the growing demand.7–9 In India, efforts to provide mental health services for children date back to the 1940s. 10 The establishment and functioning of child psychiatry units (CPUs) in India have been well documented. Initially, these units primarily focused on providing clinical services. Over time, training mental health professionals (MHPs) in child and adolescent mental health also became a key objective.11,12 However, the treatment gap remains substantial. 10
A retrospective chart review (RCR) is a research design that uses pre-recorded, patient-centered data to address specific research questions. 13 In clinical practice, chart reviews are essential tools for evaluating current practices and improving services. 14 The advantages and methodological guidelines for conducting RCRs in child psychiatry have been well- documented. 15 Notable benefits include the relatively low cost of accessing existing data and the ability to study conditions with a long latency period between exposure and disease onset. 15
Several RCR studies have been conducted globally and in India, focusing on the sociodemographic characteristics, clinical presentations, and management of children attending tertiary care centers. For example, a study in Nigeria found seizure disorder (33.1%) to be the most common diagnosis, followed by schizophrenia (15.2%), mental retardation (12.6%), acute psychotic disorder (11.9%), and depression (7.3%). 16 A study from northeast India found that neurotic, stress-related, and somatoform disorders were the most prevalent (41.4%), followed by substance use disorders (21.3%), mood disorders, and psychotic disorders. 17
A retrospective study from a CPU in North India indicated that most children attending the unit were aged 10–15 years and came from rural backgrounds. 18 Intellectual developmental disorder was the most common diagnosis (21.2%), followed by attention deficit hyperactivity disorder (ADHD) (17.9%) and conduct disorder (2.3%). 18 Joseph et al. 19 studied care pathways and found that pediatrics departments, faith healers, and child guidance clinics were often the first point of contact for families seeking help for their children. It has been seen that children typically reach CPU at the fourth step in their care pathway, with referrals largely coming from other medical specialties. 20 Referral reasons have been explored in some studies, with academic decline or mood and behavioral symptoms emerging as primary concerns.20,21 These findings reveal significant heterogeneity in referral reasons, care pathways, and diagnoses of children attending CPUs, underscoring the need for regional studies to capture local variations and improve services.
Although a few RCRs from CPUs in India have primarily focused on the prevalence of various mental disorders, there is limited information about referral reasons and pathways to care. The current retrospective study aims to address this gap by examining the referral patterns, pathways to care, clinical concerns, and diagnoses of children attending a CPU at a tertiary hospital in South India.
Methods
Study Settings and Outcomes
A five-year retrospective chart review (2017–2022) was conducted in the Child Psychiatry Unit (CPU), Department of Psychiatry, at Kasturba Medical College, Manipal, a tertiary care hospital in southern India. The CPU is an integral part of the Department of Psychiatry, led by a multidisciplinary team consisting of a child psychiatrist, a senior resident, and a postgraduate resident. The CPU operates outpatient clinics twice a week. Patients can schedule appointments directly at the CPU or be referred by other units within Psychiatry or other specialties. The study received approval from the institutional ethics committee of Kasturba Medical College and Kasturba Hospital (IEC1: 30/2023). The hospital caters to patients from coastal and other parts of Karnataka, and from neighboring states of Goa, Tamil Nadu, and Kerala. All patients visiting CPU undergo a brief evaluation during their initial visit. A comprehensive workup is conducted for those requiring diagnostic clarification and inpatient care. In the current study, we reviewed all the children and adolescents (≤18 years) who underwent brief evaluations in the CPU between January 2017 and December 2022. The case records without consultant clinical notes, lacking follow-up appointments, incomplete, or being physically damaged were excluded. The outcome measures were the pathways to care, referral reasons, and clinical diagnoses. Additional outcomes included demographic and clinical profiles of the children and their relationships with other outcomes.
Data Collection
Two investigators (first and second author) screened the brief workup files and extracted relevant data from those meeting the inclusion criteria. A semi-structured data collection form was used to gather demographic and clinical details, including the point of first contact after symptom onset, referral patterns, major presenting symptoms, diagnoses, and psychiatric and physical comorbidities. Diagnoses were assigned based on the International Classification of Diseases,10th edition, or the Diagnostic and Statistical Manual of Mental Disorders, 5th edition guidelines. The first point of contact was categorized into the following groups to analyze pathways to care: MHPs, other medical specialties, paramedical professionals, general practitioners, Ayurveda, Yoga, Unani, Siddha, and Homeopathy (AYUSH) practitioners, or religious institutions. To ensure the reliability of data extraction, both investigators independently reviewed data from the first 50 files. Inter-rater reliability (IRR) was calculated for each question with categorical responses using Cohen’s Kappa to ensure consistency.
Data Analysis
Data were analyzed using the IBM SPSS Statistics, version 23. Continuous variables were summarized as means and standard deviations, while categorical variables were presented as frequencies and percentages. IRR was evaluated using Cohen’s Kappa (κ) to ensure consistency in observational ratings, following chart review guidelines. 15 Associations between pathways to care, diagnoses, presenting complaints, and demographic profiles were assessed using the chi-squared tests. Effect sizes were calculated as Cramer’s V, with values >0.1 considered moderate association, >0.15 as strong, and >0.25 as very strong association. 22 A P value of <.05 was considered statistically significant.
Results
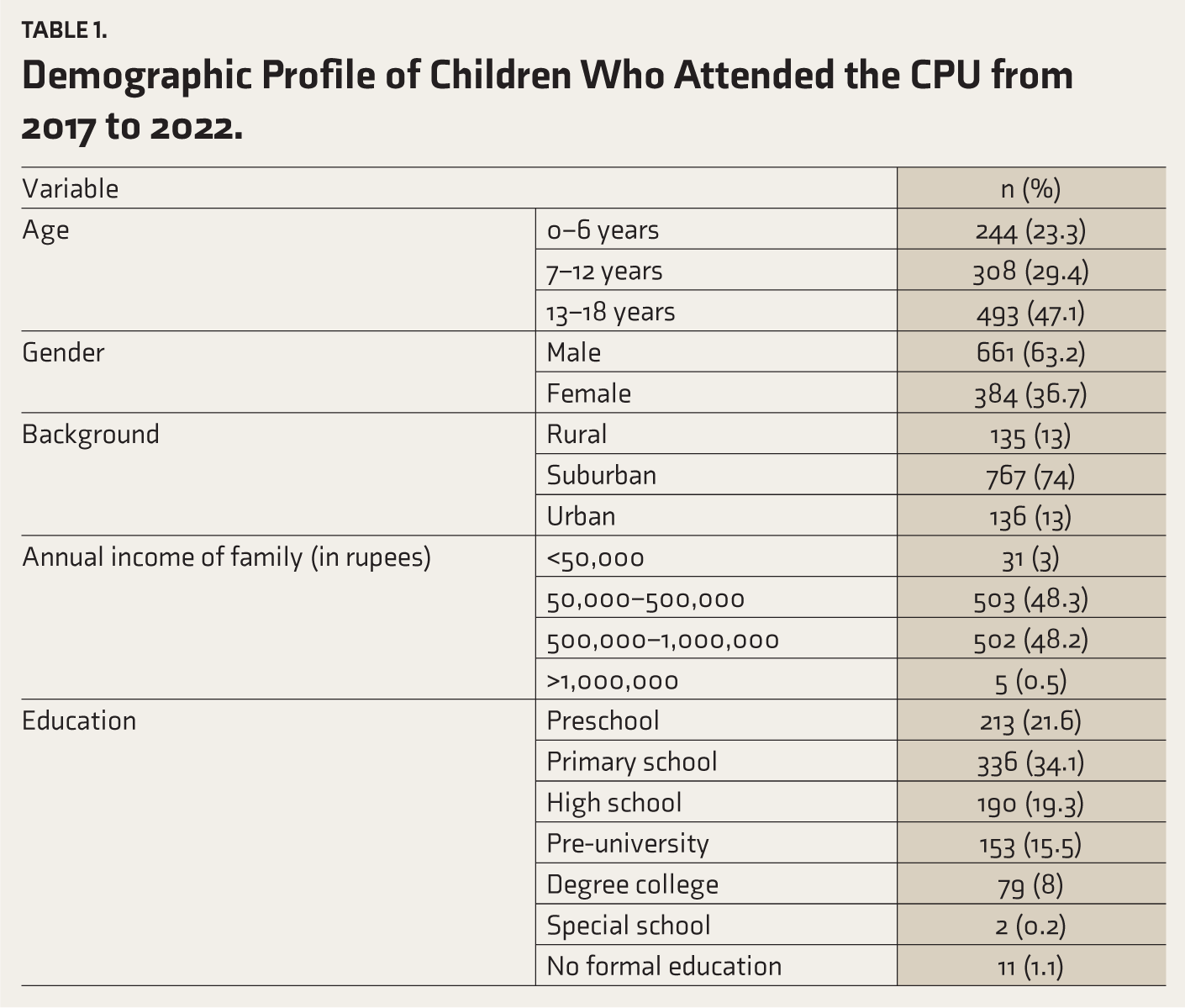
Of the 1,465 brief workup files in the CPU register, 1,046 were included in the study after excluding 419 files with missing data due to damage or unavailability during digitization. There was a near-perfect agreement between the two data extractors (first and second author) on categorical data extraction (κ = 0.91± 0.05, 95% CI 1.00–0.81), P < .001. IRR for individual items is presented in Supplementary Table 1. The mean age of the sample was 11.2 ± 4.9 years, with the majority of children in the adolescent age group (13–17 years). The demographic profile showed a male predominance (63.2%), with most children residing in suburban areas and attending primary school (34.1%) or high school and above (42.8%) (Table 1).
Demographic Profile of Children Who Attended the CPU from 2017 to 2022.
In the pathways to care, the first point of contact for children following the onset of symptoms is as follows. The majority of children (97.5%) initially contacted a healthcare provider, with MHPs (29.3%) and other medical specialties (59.6%) being the most common points of contact. Within the medical specialties, pediatrics was the most common first contact (49%). A small minority of children (2.5%) initially approached religious institutions (see Supplementary Table 2 for details).
Primary Referral Reasons for Children who Attended CPU.
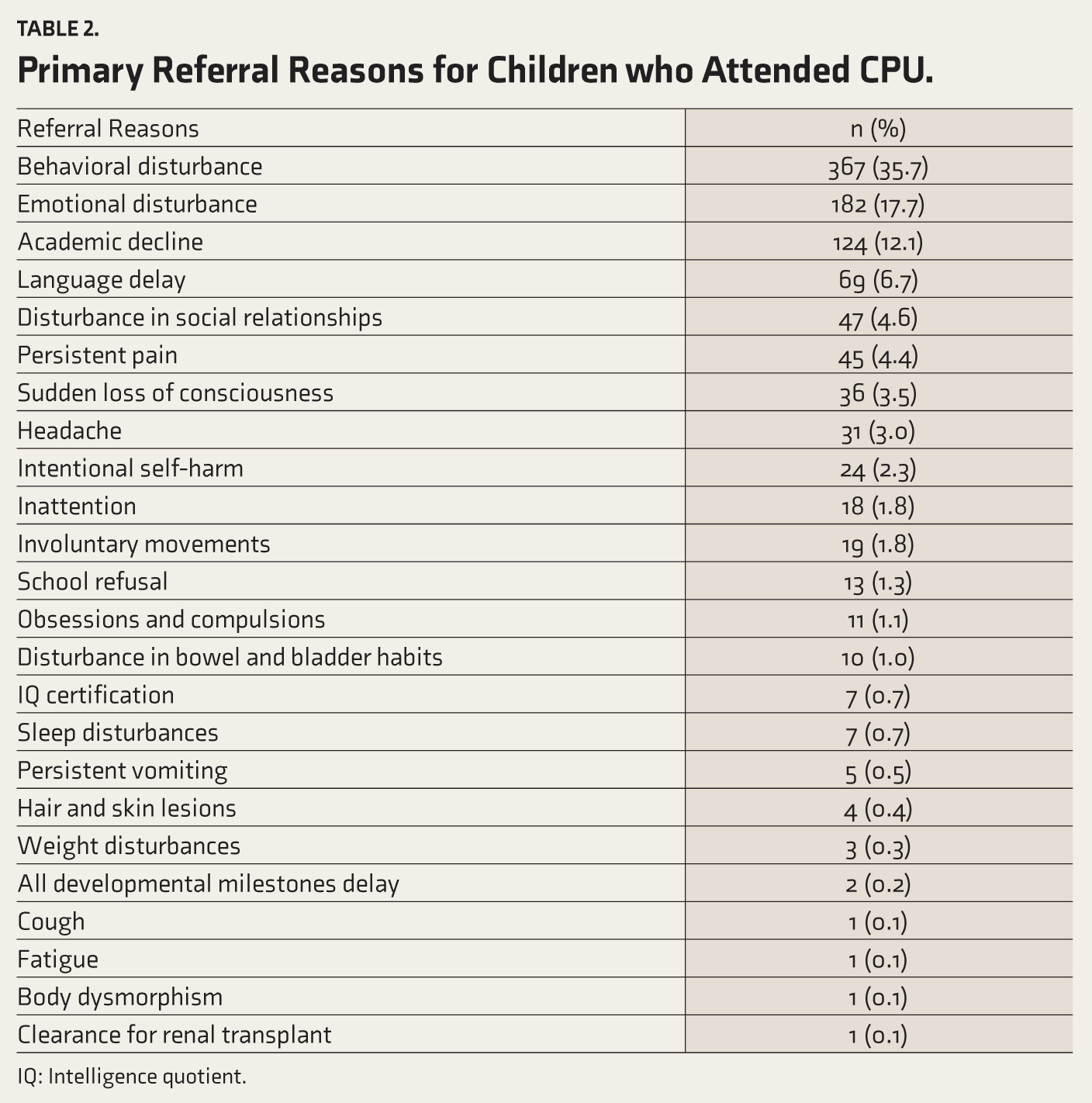
IQ: Intelligence quotient.
The primary reasons for referral to our CPU are presented in Table 2, with behavioral disturbance being the most common, followed by emotional disturbance. Common referral reasons also included academic decline and language development delays. Other notable reasons were problems with social relationships, persistent pain, intentional self-harm, headaches, and sudden loss of consciousness.
Table 3 summarizes the primary psychiatric diagnoses and comorbidities. The most prevalent primary diagnoses were attention deficit hyperactivity disorder (ADHD) (16.5%), intellectual developmental disorder (14.7%), and pervasive developmental disorder (PDD) (12.6%). Other common diagnoses included depressive disorders, dissociative disorders, anxiety disorders, and obsessive-compulsive and related disorders (OCRDs). Notably, 12.5% of cases lacked a formal diagnosis in the records, and 2.9% did not meet the criteria for any psychiatric diagnosis.
Primary Psychiatric Diagnosis and Major Psychiatric Comorbidities of the Children who Attended CPU.
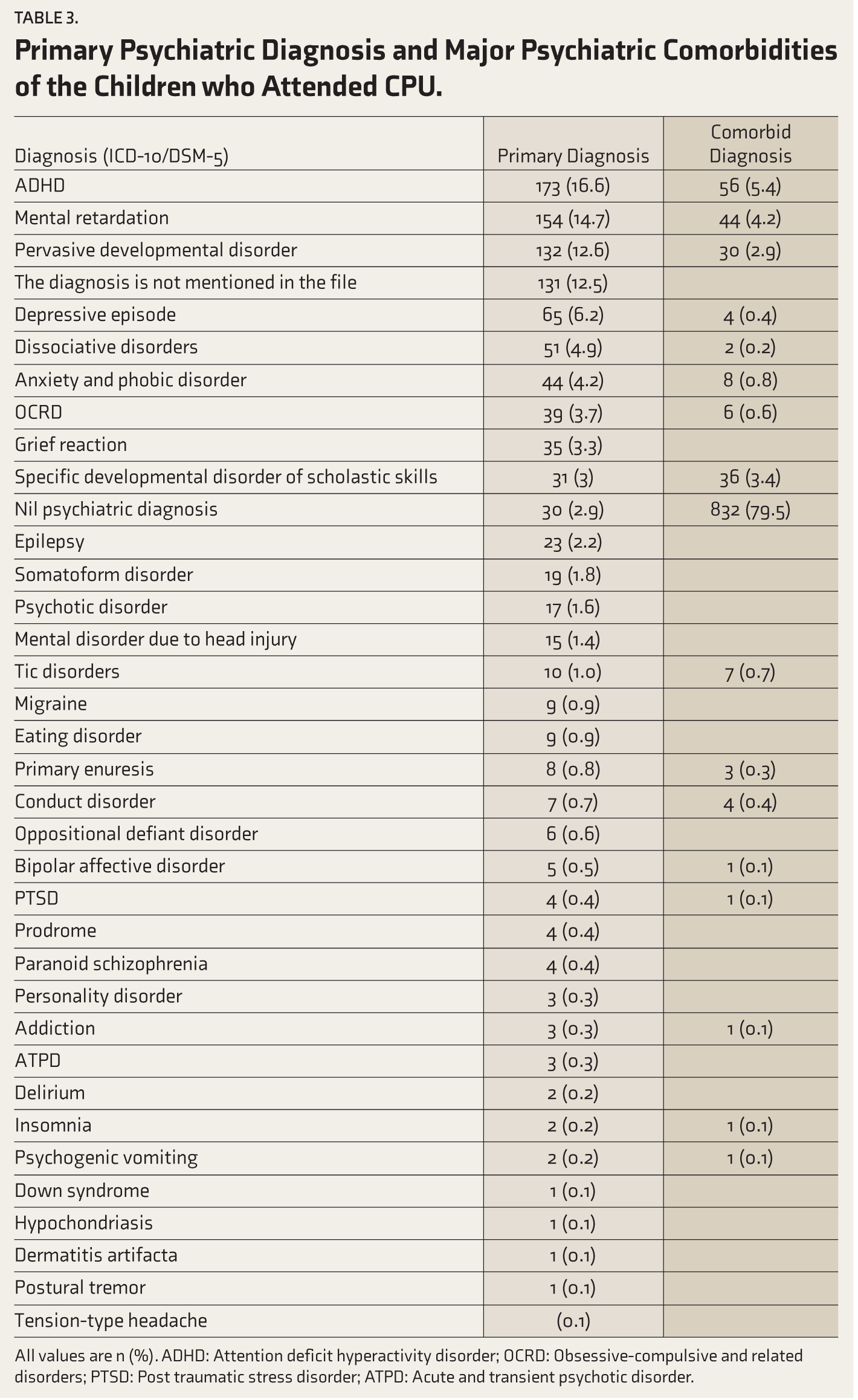
All values are n (%). ADHD: Attention deficit hyperactivity disorder; OCRD: Obsessive-compulsive and related disorders; PTSD: Post traumatic stress disorder; ATPD: Acute and transient psychotic disorder.
Comorbid psychiatric diagnoses were present in 19.7% of children, with ADHD (5.4%) being the most common comorbidity with any psychiatry diagnosis, followed by intellectual developmental disorder (4.2%) and specific learning disability (2.9%). Additionally, 22.6% of the sample had medical or physical comorbidities at presentation. Epilepsy was the most frequently reported comorbidity (11.1%), followed by iron deficiency anemia (1.2%), vitamin D deficiency (1%), hypothyroidism (0.8%), and Wilson disease (0.7%).
The relationship between pathways to care and referral reasons to the CPU was examined using a chi-squared test of independence (Figure 1). For most children, the initial point of contact for their healthcare needs was typically either a medical specialist or an MHP. Notably, children presenting with behavioral disturbances were the most likely to seek help from religious institutions. There was no significant association between pathways to care and referral reasons (χ2(115, N = 1015) = 132.9, P = .12), suggesting that these variables are independent in our sample.
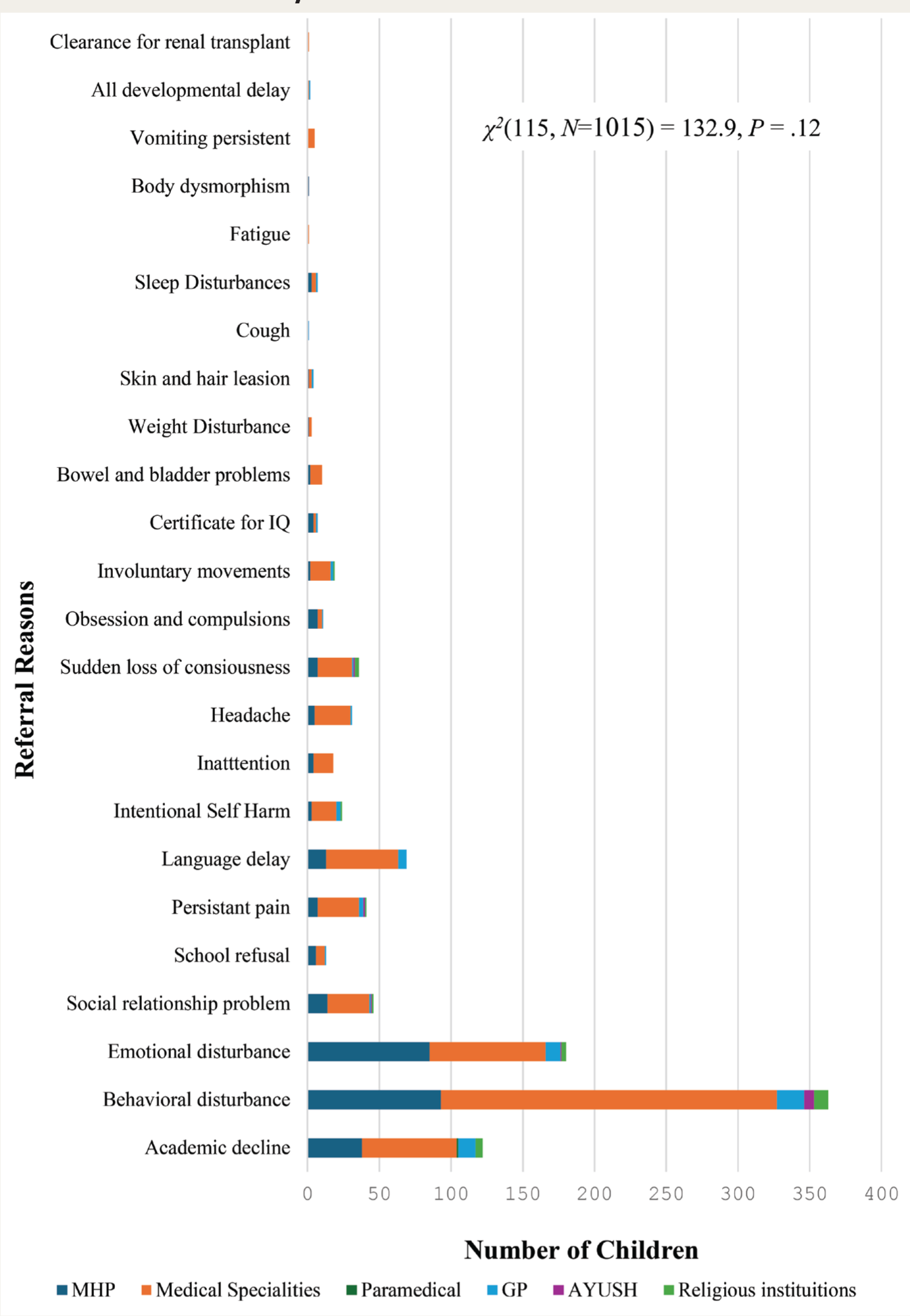
MHP: Mental Health Professional; GP: General Practitioner; AYUSH: Ayurveda, Yoga, Unani, Siddha, and Homeopathy.
The relationship between pathways to care and primary psychiatric diagnosis was examined using a chi-squared test of independence (Figure 2). Results showed that children with depressive disorders, anxiety disorders, and OCRDs were more likely to consult MHP first compared to other pathways. However, medical specialities remained the predominant first point of contact for most diagnoses. A significant association was found between pathways to care and primary psychiatric diagnosis (χ2(175, N = 1029) = 239.6, P = .001), with a medium effect size (Cramer’s V = 0.21). This indicates a strong relationship between the pathways to care and diagnosis.
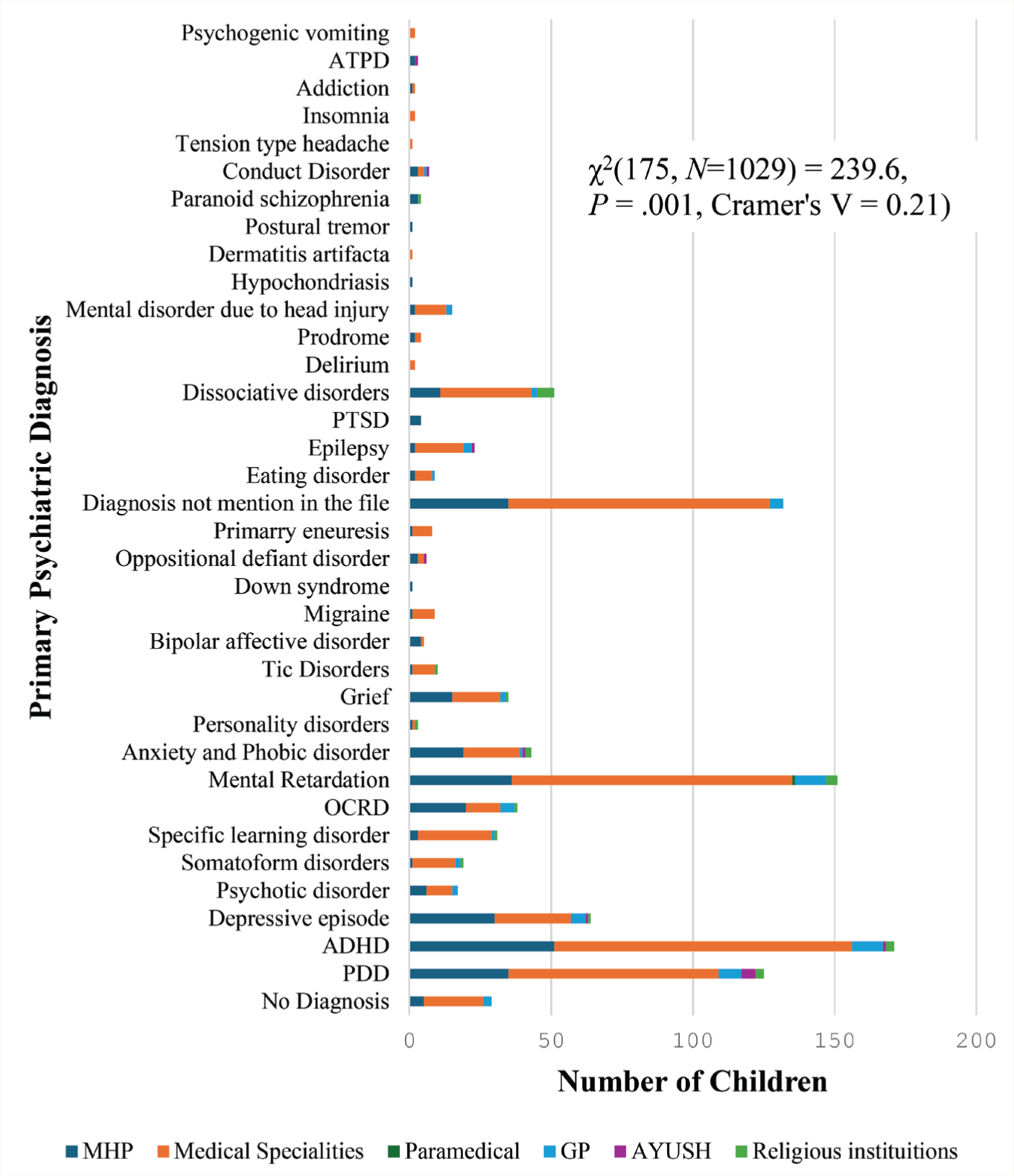
ADHD: Attention Deficit Hyperactivity Disorder; OCRD: Obsessive-Compulsive and Related Disorders; PTSD: Post-traumatic Stress Disorders; ATPD: Acute and Transient Psychotic Disorder; PDD: Pervasive Developmental Disorder; MHP: Mental Health Professional; GP: General Practitioner; AYUSH: Ayurveda, Yoga, Unani, Siddha, and Homeopathy.
We have examined the relationship between gender, referral reasons, and diagnosis, as gender has an association with specific diagnoses (Supplementary Figures 1 and 2). Chi-squared tests revealed significant associations between gender and referral reasons (χ2(23, N = 1027) = 95.3, P < .001, Cramer’s V = 0.31) as well as gender and diagnosis (χ2(35, N = 1045) = 142.6, P < .001, Cramer’s V = 0.37). Male children were more frequently referred for behavioral disturbances, academic decline, emotional disturbances, language delays, and disturbed social relationships. In contrast, girls were more frequently referred for emotional disturbances, somatic complaints (such as pain and headache), and dissociative symptoms. Boys were more frequently diagnosed with ADHD, PDD, mental retardation, and specific learning disability (SLD). In contrast, girls were more commonly diagnosed with depressive disorders, grief reactions, anxiety disorders, and dissociative disorders.
Discussion
Sociodemographic Characteristics
Our study’s findings align with large population-based cohort studies that report a higher cumulative incidence of child and adolescent-onset disorders among males. 23 Similarly, our chart review found that most children attending the CPU were male, aligning with retrospective studies conducted in Nigeria 16 and India. 21 The mean age of children in our sample was comparable to similar studies from India 19 and Nigeria. 16 A significant proportion of children in our study were from suburban areas, likely reflecting the hospital’s location. This contrasts with a previous study that reported a higher proportion of children from rural backgrounds. 18 Differences in socio-economic status were also observed, with most families in our study reporting an annual income between ₹50,000 and ₹10 lakh. This contrasts with other Indian studies, which found a higher proportion of families from lower socio-economic strata.24,25 These differences underscore the variations in patient demographics between private and government hospitals, as previously documented. 26 Furthermore, the majority of children in our study were attending primary school or preschool, reflecting the relatively younger age distribution of our sample.
Referral Reasons and Pathways to Care
Behavioral and emotional disturbances and academic decline were the most common referral reasons in our study, aligning with findings from other regions, including India.19,27,28 Previous Indian studies also highlighted academic decline and certification for mental retardation as prominent referral reasons.21,25 Male children were more frequently referred for behavioral symptoms, academic decline, and disturbed social relationships, reflecting the higher prevalence of ADHD, ASD, and other neurodevelopmental disorders among males. 29 In contrast, girls were more frequently referred for emotional disturbances, somatic symptoms, and dissociative symptoms, consistent with the higher prevalence of mood and dissociative disorders in females.23,29
Notably, most children in our study initially sought help from a medical or mental health professional, indicating growing awareness of the importance of medical evaluation for children’s symptoms. The pediatrics department was the most common first contact and referral source to the CPU. Although specific consultation reasons in pediatrics are unknown, research suggests that children often initially present physical symptoms, prompting early contact with general practitioners or medical specialists. 30 These findings underscore the need to train pediatricians, medical specialists, and general practitioners in recognizing neurobehavioral symptoms early to ensure timely diagnosis and intervention. Our findings on the first contact point align with a study from South India, which also identified psychiatry and pediatrics as the most common initial point of contact. 19
The Diagnoses of Children Attending the CPU
Our retrospective chart review identified ADHD as the most common diagnosis, followed by mental retardation and PDD. Other frequently diagnosed conditions included depressive disorders, dissociative disorders, OCRD, anxiety disorders, specific learning disorders, and somatoform disorders. These findings align with a nationwide cohort study involving 1.2 million children, which reported anxiety disorders as the most prevalent diagnosis, followed by ADHD, ASD, developmental disorders, and depressive disorders. 29 The diagnostic pattern in our study mirrors global trends. It is consistent with findings from other South Indian studies, which reported externalizing, mood, neurodevelopmental, anxiety, and intellectual developmental disorders as common diagnoses.21,24 However, a study from Nigeria reported a higher prevalence of epilepsy, schizophrenia, and mental retardation in the pediatric population, highlighting regional variations in diagnostic patterns. 16 Interestingly, our study revealed a higher incidence of dissociative and somatoform disorders compared to other Indian studies, suggesting a potential cultural predisposition among South Indian children.31,32 This observation is further supported by findings from a study conducted in Kerala. 24 Additionally, our study confirmed a significant association between gender and psychiatric diagnosis, consistent with large population-based research that underscores the bio-social influences of sex and gender on the development and presentation of psychiatric disorders.23,29
Comorbid psychiatric and physical conditions are frequently observed in children with a primary psychiatric diagnosis, with studies reporting their occurrence in nearly half of such cases. Accurate identification and timely management of these comorbidities are essential, as they significantly influence the progression and treatment outcomes of the primary disorder.33,34 While previous studies have reported high rates of comorbidities, our research found that approximately one-fifth of children had a comorbid psychiatric diagnosis. ADHD and mental retardation were the most common comorbid psychiatric conditions, consistent with existing evidence.33,34
Regarding physical comorbidities, seizure disorders and nutritional deficiencies were the most prevalent in our sample. This aligns with prior research identifying seizure disorders as the most common physical condition among children with psychiatric diagnoses. 35 Effective identification and management of such comorbidities remain critical to improving treatment outcomes and overall well-being.
Strengths and Limitations
Our retrospective chart review used a rigorous methodology to collect data from a large five-year sample, ensuring high IRR between data extractors prior to full data collection. The regional-specific nature of our study data provides valuable insights into childhood disorders within the local context. However, the study had certain limitations. Specifically, 416 case record files were excluded due to missing documentation during digitalization, and the retrospective design precluded detailed information on pathways to care, which would have offered a deeper understanding of referral patterns. Additionally, the absence of recorded diagnoses in many files limited the scope and completeness of our findings.
Conclusions
Our study revealed a positive trend, with most parents seeking early help from MHPs or medical professionals for their children. Behavioral and emotional symptoms were the primary reasons for referral, reflecting the high prevalence of externalizing disorders among children and adolescents. Common diagnoses included ADHD, PDD, mental retardation, and mood and anxiety disorders. Our study identified a gender-specific pattern in referral reasons and diagnoses, consistent with previous findings. These insights can inform regional presentation patterns and diagnoses, enabling the refinement of services tailored to the needs of children and adolescents.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors used Meta AI to edit language and correct grammar.
Ethics Approval
The study received approval from the institutional ethics committee of Kasturba Medical College and Kasturba Hospital (IEC1: 30/2023).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Prior Presentations
None.
Submission to Another Journal or Resource
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.