
Abstract

Dear Editor,
Pica is described as eating non-nutritive, non-food items for at least one month, sufficiently severe to necessitate clinical attention, which is inappropriate for the developmental level of the individual and is not part of a culturally supported practice. 1 The non-eatables that are most commonly discussed about pica include ingestion of soil, sand, clay (geophagia), ice (pagophagia), starch (amylophagia), hairs (trichophagia), glass (hyalophagia), etc.2,3 Another rarely described pica is “acuphagia,” which is used to describe a type of abnormal eating behavior characterized by eating sharp metal objects. In acuphagia, the presence of a foreign body in the gastrointestinal tract, especially in high volumes, can cause bleeding, obstruction, and rupture of intestines and subsequently lead to peritonitis, shock, and death. 4 Usually, pica is reported as an independent/isolated disorder. However, during the early years of life, it has been reported to be associated with developmental disorders such as intellectual disability and autism. However, among adults, it has been commonly reported to be associated with other comorbid conditions like obsessive-compulsive disorder and schizophrenia.5,6
The published literature provides limited data on acuphagia. In their case report, Rezazadeh et al., 7 reviewed 28 cases of metallic foreign body ingestion, with all included cases not conforming to the definition of acuphagia, which is characterized by eating sharp metal objects. Out of these 28 cases, 24 were considered as acuphagia, and the age of these cases ranged from 20 to 67 years, and the majority (n = 15) of them were males. Out of the 24 cases of acuphagia, 11 were diagnosed with schizophrenia or schizophrenia spectrum disorders, four were diagnosed with affective disorder, and one patient was found to have an intellectual disability. In one case, the psychiatric disorder was not specified. Instead, it was mentioned that it was a mental abnormality. 7 However, none of the included cases had information about recurrent acuphagia requiring surgical intervention. There is no clear understanding of the association between acuphagia and schizophrenia. However, some of the reports that have focused on pica in schizophrenia patients suggest that this could be influenced by delusional beliefs related to nutrition, part of disorganized behavior, hyperorality due to cognitive impairments and lesions in the temporal lobes, psychotropic-induced compulsive eating of inedible things, prolonged malnutrition and deficiencies of micronutrients, comorbid obsessive-compulsive disorder, and inhibition of the hematopoietic system by the long term use of psychotropic medications. 6 However, it is important to note that various associations are noted in different case reports.
In the current case report, we describe a young male with treatment-resistant schizophrenia who presented to the emergency department with pain in the abdomen and, on evaluation, was found to have acuphagia, requiring recurrent evacuation of foreign bodies. Written consent was obtained from the patient to report the anonymized clinical presentation.
Case Report
A 26-year-old single male presented to the emergency with pain in the abdomen. Exploration of history revealed that the patient has had a mental illness for 13 years. Delusions of reference, persecution and grandiosity, auditory hallucinations, disorganized speech, dis-organized behavior, and negative symptoms characterized the illness. The onset of psychotic symptoms was preceded by the use of cannabis in a dependence pattern, and the psychotic symptoms would persist despite intermittent stoppage of cannabis use for periods of months at a stretch. He also had a history of ingestion of multiple metallic sharp objects for the last four to five years, leading to medical emergencies in the form of acute abdomen. He had undergone numerous endoscopic interventions for the removal of ingested foreign bodies. For his psychotic symptoms, the patient was admitted to multiple hospitals in the past for his mental illness and had received multiple adequate antipsychotic trials (risperidone 6 mg/day, trifluoperazine15 mg/day, and clozapine 500 mg/day). He had also received three cycles ofECT.
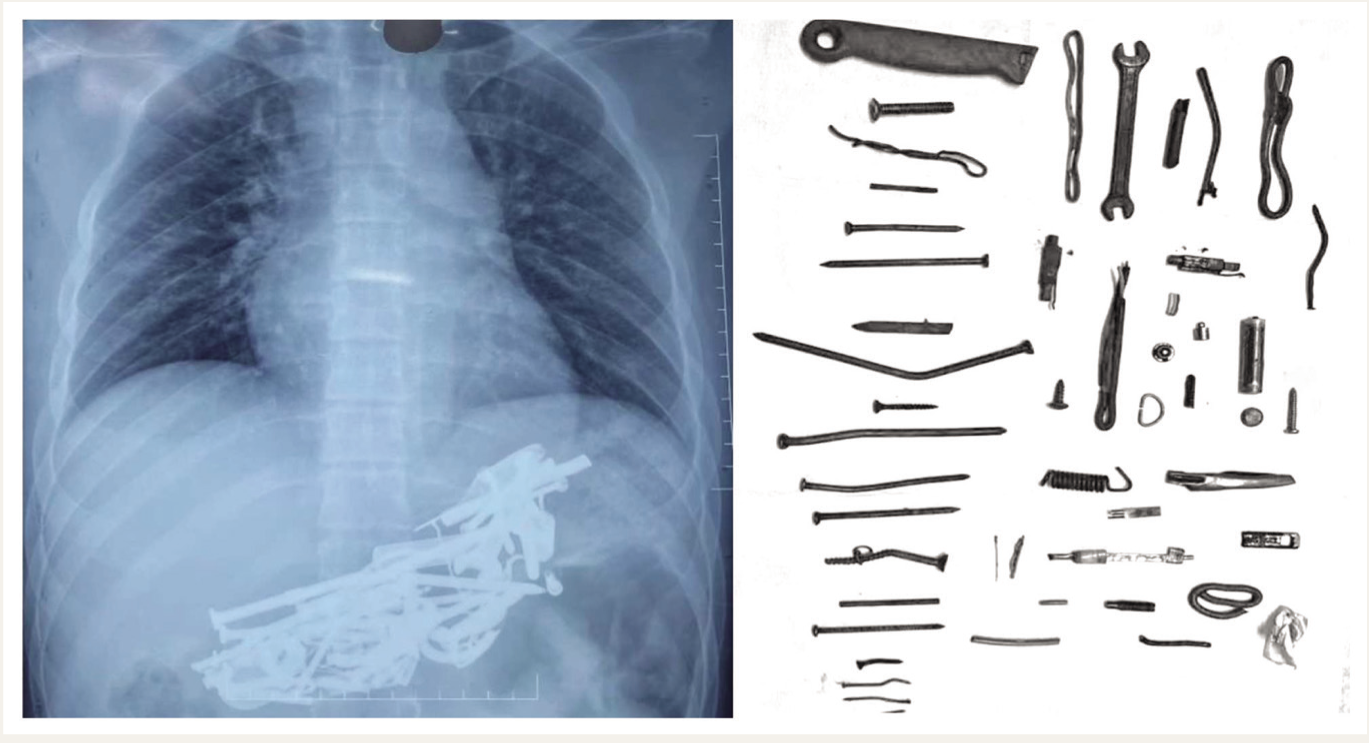
Upon arrival in the emergency department, an X-ray of the abdomen revealed multiple radiopaque shadows. A liaison with gastroenterology was done, and emergency endoscopic removal of 190 foreign bodies (including nails, screwdrivers, batteries, knives, etc.) was performed under general anesthesia (Figure 1). He was admitted to the psychiatry ward for further management. His routine investigation, including his complete blood count, iron profile, and contrast-enhanced magnetic resonance imaging (CE-MRI) of the brain, did not reveal any abnormality. His treatment history revealed that he had maximum improvement with clozapine; however, he had developed an episode of seizure at a clozapine dose of 500 mg/day, for which he was administered sodium valproate 1000 mg/day.
An X-ray of the Abdomen Showing the Ingested Material and Some of the Items Removed by the Endoscopy.
After a detailed evaluation, in terms of psychiatric issues, as per the International Classification of Diseases, Eleventh Revision (ICD-11) criteria, 8 diagnoses of schizophrenia, multiple episodes, currently symptomatic, tobacco dependence, currently using and cannabis dependence, currently abstinent, were kept. The patient was restarted on clozapine and was also administered bilateral ECT. Nicotine replacement therapy was started for tobacco dependence. He received an acute course of 12 ECT sessions, followed by continuation ECT. Additionally, behavioral measures, such as 24-hour round-the-clock monitoring, distraction techniques, and contingency management, were done for the patient to keep him away from ingestion of non-nutritive materials. His family members were psycho-educated about the illness.
Over three months, the dose of clozapine was increased to 500 mg/day, and tab lamotrigine 200 mg/day was started as an augmenting agent that is also an anti-epileptic agent. He was continued on twice-weekly continuation ECT. After the third month, he would no longer search for inedible substances and continued to have minimal positive symptoms, with overall about 60% improvement (Positive and Negative Syndrome Scale 9 score reduced from 134 to 54; Clinical Global Impression scale 10 severity rating reduced from 7 [among the most extremely ill patients] to 4 [moderately ill]). Imaging was also repeated twice to ensure that there were no residual or new foreign bodies that the patient might have consumed during the ward stay and that they were normal. The patient’s relatives, however, continued to remain critical of him, and they were psycho-educated about the same. After three months, he was shifted to another hospital for further stabilization and was thereafter lost to follow-up.
Discussion
There is limited literature on acuphagia. In a case report published in 2023, 7 on the ingestion of metallic foreign bodies, the authors reviewed 28 cases, including one of their cases. In our search, we found one more case of acuphagia in a 16-year-old male with obsessive-compulsive disorder. 8 Our index case was a young male suffering from schizophrenia. The majority of these patients presented with abdominal pain, followed by symptoms of nausea, vomiting, and fever. 7 Our index case also presented with abdominal pain. In terms of the number of metallic items removed, one of the reports documented the removal of 648 items; however, these were not sharp metallic items and were instead metallic coins. 11 In our index case, 190 items were removed, most of which were sharp nails and screws. Additional items included a spanner, battery, and metallic spring. Different hypotheses have been suggested for the association of pica and schizophrenia. In our case, the acuphagia was most likely related to the patient’s delusional belief about the nutrient value of the non-edible materials. However, he never explicitly gave any explanation.
Although the majority of cases of acuphagia are reported in patients with schizophrenia, there is limited data on inappropriate feeding behaviors in patients with schizophrenia. A study that evaluated feeding behaviors among 206 schizophrenia patients in a psychiatric hospital reported the prevalence of pica to be 14.3%. 10 Little is known about the course of acuphagia. The index case had undergone endoscopic removal of metallic items in the past. Accordingly, our case highlights the fact that acuphagia in schizophrenia patients could be a long-lasting condition. Many of the hypotheses given for pica in schizophrenia could have played a role in the persistence of acuphagia in the indexcase.
Our case highlights the fact that when a patient with schizophrenia presents with a history of pain in the abdomen, a possibility of acuphagia should be considered as a differential diagnosis. The patient’s eating habits should be carefully reviewed, and if required, appropriate investigations in the form of an X-ray of the abdomen and pelvis and ultrasound of the abdomen should be considered. A close liaison with other specialists needs to be considered in a patient with a history of eating sharp metallic objects to prevent complications.
Conclusion
As acuphagia is part of the broader rubric of pica, the phenomenon of pica in patients with schizophrenia needs to be evaluated in more detail in terms of prevalence, patients’ understanding and attribution of such behavior, and treatment strategies that work for pica in schizophrenia patients.
Supplemental Material
Supplemental material for this article is available upon request to the corresponding author.
Footnotes
Declaration Regarding the Use of Generative AI
We declare that we have not used AI tool for writing this manuscript.
Funding
The author received no financial support for thisresearch, authorship, and/or publication of this article.
Simultaneous Submission to Another Journal or Resource
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.