
Abstract

Dear Editor,
Obsessive-compulsive disorder (OCD) is a chronic debilitating mental illness with waxing and waning courses. 1 The H7 coil used for deep repetitive transcranial magnetic stimulation (dTMS) is designed to produce deeper and broader neuronal stimulation in the dorsomedial prefrontal cortex and anterior cingulate cortex, which is known to alleviate the symptoms of OCD.2,3 A real-world observational study also emphasized the efficacy of the H7 coil in OCD. 4 This report discusses the application of protocol customization in a non-responder 54-year-old female leading to remission. Informed consent was obtained from the patient for publication of this report.
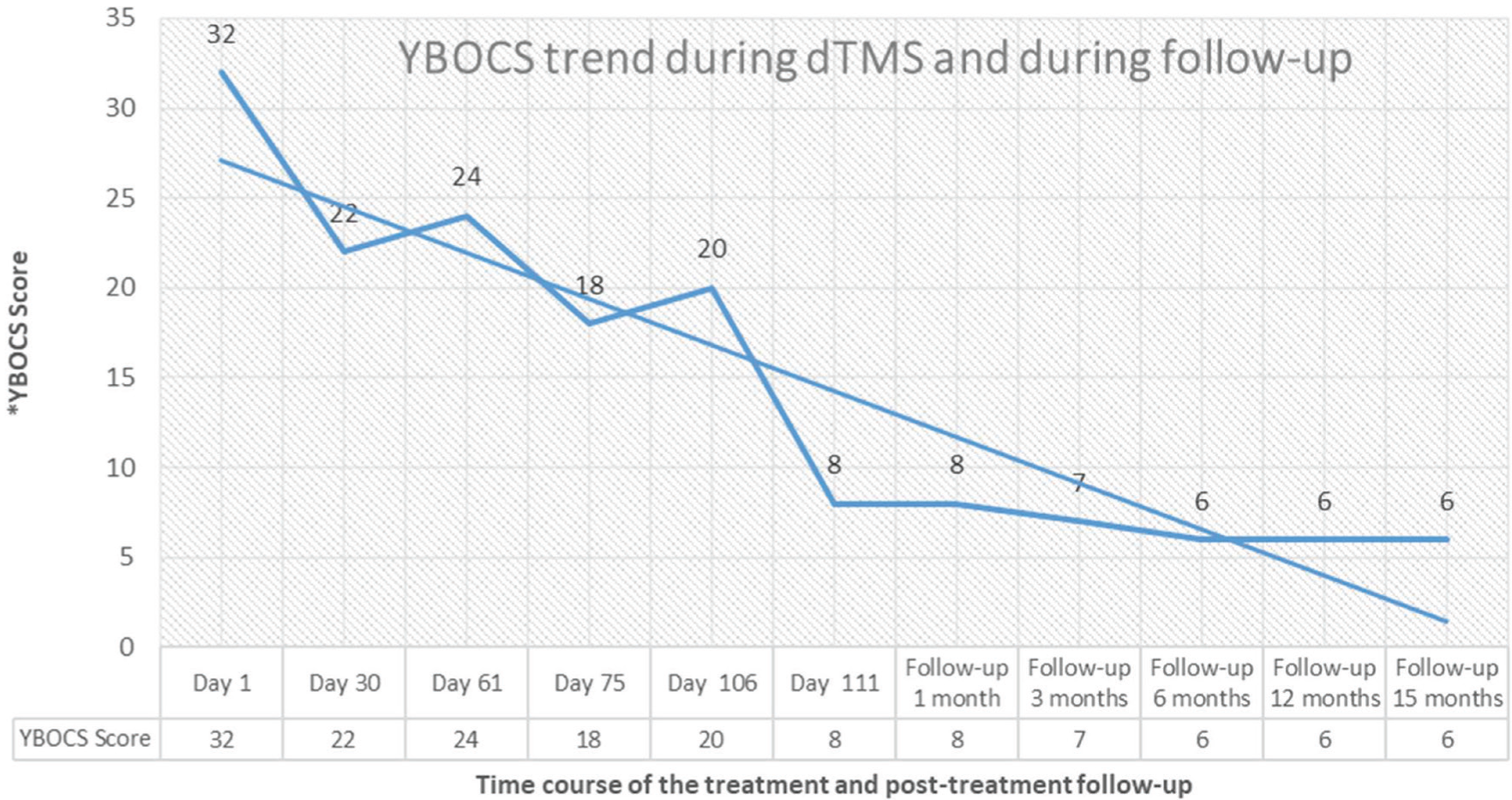
A 54-year-old female patient was having miscellaneous obsessions, somatic obsessions (concern with illness, salivation), inferiority complex, feelings of guilt, lack of self-worth, doubt, and anxiety. She was diagnosed as having OCD. 4 She was on regular treatment with fluvoxamine 100 mg/d and venlafaxine 37.5 mg/d for about 22 years. After a recent spike in symptoms, she was advised to take dTMS with an H7 coil using a BrainsWay deep TMS 104 device. Treatment began after obtaining informed written consent from the patient and a detailed screening for electromagnetic field compatibility and safety. An approved treatment protocol was decided to be given to the patient. Forty-five dTMS sessions were given in total, 30 first and 15 as maintenance after about a month. As shown in Figure 1, the target area was located according to the standard BrainsWay manual, keeping the helmet 4 cm below the level of finding the foot twitch. Each session consisted of 50 20Hz 2s 100% Resting Motor Threshold trains with an interval of 20s, delivering 2,000 pulses. 5 The Yale-Brown Obsessive-Compulsive Scale (YBOCS) reduced to 22 from an initial score of 32, but the patient reported minimal subjective improvement. She relapsed within a month. Eventually, we did a literature search to find an innovative and suitable treatment for her. We then arrived at the idea of adjusting the train frequency in order to stimulate the target neurons with more certainty. EEG studies in OCD explain frontal theta or delta predominance in some patients. In the same line, we planned to record resting EEG and customize the intermittent theta burst stimulation (iTBS) according to peak frequency in the bilateral prefrontal areas. Fast Fourier Transform (FFT) graphs depicted 3Hz activity in line with previous studies. 6 The protocol was customized, replacing the standard 5Hz train frequency with 3Hz. Burst frequency remained at 50Hz. After a gap of 15 days, the patient was called again and explained about the possibility of new treatment. After obtaining the consent, six customized EEG-iTBS sessions were given prior to the regular high-frequency stimulation as priming sessions. From the third session onwards, the patient reported a 50% fall in the severity of obsessions. By the sixth session, she reported great symptom relief and happiness. Her emotional pain score on the Visual Analog Scale dropped to two from the previous score of eight. YBOCS reduced from 20 to 8. Figure 2 depicts follow-up YBOCS scores during 1, 3, 6, 12, and 15 months. Currently, she is on fluvoxamine 100 mg/day and venlafaxine 37.5 mg/day.
Site of Stimulation Using H7 Coil in OCD. (a) The final position of the H7 helmet is shown, measured as 4 cm anterior to the location of the foot twitch (motor cortex). (b) The areas stimulated in the brain by the H7 coil. The pink-shaded area is the dorsomedial prefrontal cortex (dmPFC), and the blue-shaded area is the anterior cingulate cortex (ACC).

The Trend in Yale-Brown Obsessive-Compulsive Scale (YBOCS) Scores Observed During Deep Transcranial Magnetic Stimulation (dTMS) and the Follow-up Period Up to 15 Months.
To conclude, the new customized protocol delivering 540 pulses per session, each session consisting of 20 trains of 3Hz, 3s duration, and nine triplet bursts with an interval of 8s at an intensity of 80%, has helped our patient achieve remission. The good response shown by the patient in just six sessions was maintained thereafter for 15 months. Adjusting train frequency in this patient must have led to better stimulation of neurons in the target area falling in phase with the resting state neuronal firing. Further research is required in this direction. The authors also wish to repeat the same customization method in a bigger sample of non-responding patients in the future.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Nil.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from the participant.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.