
Abstract

Sutar R, et al., 1 have done a commendable job in conceptualizing the need for developing a Hospital Mental Health Screen (HMHS) for medically ill patients in India. It is appreciable that various psychiatric morbidities and relevant psychological conditions have been considered. However, we have identified some methodological and statistical gaps, elaborated below, that require further reflection.
The authors stated in the methodology section that “the exploratory factor analysis (EFA) was conducted to understand the latent constructs.” However, in the Statistical Analysis section, they mentioned that they conducted Principal Component Analysis (PCA).
Although manuscripts often erroneously report PCA as a factor analysis, they are mathematically and conceptually distinct. 2 PCA provides a concise summary of item scores, indicative of a formative measurement model, whereas EFA assumes common factors underlying the observed item scores, reflecting a reflective measurement model. This distinction is critical because it affects the interpretation of psychological assessment outcomes. 3 The PCA, while often used as an initial solution, is not ideal for identifying latent constructs in psychological assessments due to its focus on variance rather than on underlying factors. The article could have clearly differentiated the use of PCA as a preliminary step and ensured that the final factor structure is derived through methods like EFA or Principal Axis Factoring (PAF), which better align with the theoretical underpinnings of the constructs being measured.
The authors 1 have also recommended the use of confirmatory factor analysis (CFA). CFA, like EFA, is rooted in the common factor model, positing that observed variable relationships stem from shared underlying constructs represented by latent factors. 4 Given their shared theoretical foundation, CFA and EFA exhibit greater similarity compared to CFA and PCA, suggesting that findings from EFAs are more likely to translate to the CFA framework than those from PCAs.
Though Eigenvalue (≥1) and scree plot analysis are widely used methods for determining a number of factors to retain, scree plots often present ambiguity, leading researchers to rely less on them, 5 which seems the case for the current scree plot presented for HMHS. For a definitive conclusion, alternative approaches are available, such as parallel analysis (PA) based on Horn’s criterion 6 and the minimum average partial (MAP) method introduced by Velicer. 7 Additionally, Bandalos (2018) offered valuable insight, emphasizing that interpretability and theoretical relevance should be the primary criteria for selecting the number of factors, as a factor solution is only beneficial if it can be meaningfully interpreted. 8 The 27 items of the HMHS can be categorized into six diagnostic categories (Table 1). Two items represent disease burden, and four items are not disorder-specific. After PCA, the 27 items were categorized into six factors, and they did not retain homogeneous symptoms; symptoms of depression, for example, were spread across three different factors (F1, F3, and F6). Diagnosing based on these factors presents challenges. Moreover, the identified factors directly challenge DSM/ICD diagnostic criteria. The authors should have discussed these issues.
Categorization of Hospital Mental Health Screen Items.
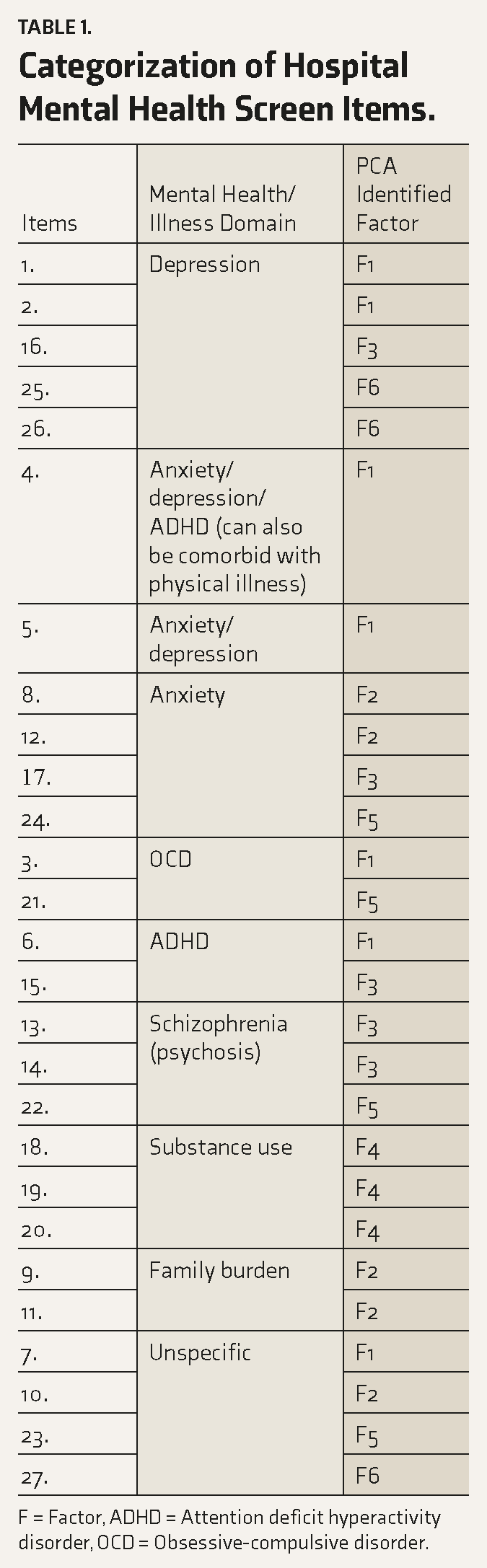
F = Factor, ADHD = Attention deficit hyperactivity disorder, OCD = Obsessive-compulsive disorder.
There might be various reasons that affected the extraction; one important contributor is the sample heterogeneity with a high weightage of medicine and surgery patients. Severity, duration, and disability related to the medical conditions are potential factors, and there should have been some data on those. By considering such sample selection criteria, EFA may become meaningful, 9 as it has appeared in the article.
Some items need to be clarified. Item 5 (“I have trouble sleeping”) can be directly attributed to pain or discomfort caused by physical illnesses, 10 not necessarily psychiatric illness. Similarly, item 4 (“I am unable to concentrate on my work”) can result from several physical illnesses; thus, it is not a specific feature representing a specific illness.
It is mentioned that two psychiatrists dichotomously categorized the presence or absence of psychiatric morbidity. What was the process of categorizing a structured interview, a semi-structured interview, or a questionnaire? It is important, as the reliability of the diagnosis may be inferred from this. Moreover, whether both the psychiatrists made their diagnosis independently and then the corroboration was assessed is also not mentioned. There is also a need to understand how many of the patients were screened (by the psychiatrists) as having psychiatric morbidity for this study. It is helpful to provide a clear methodology for establishing concurrent validity, particularly in terms of using a recognized gold standard and reporting the relevant statistics. The article should have included detailed information on how the diagnoses were made, the tools used, and the reliability of the diagnostic process, as also whether independent corroboration was assessed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.