
Abstract
Background:
The National Mental Health Survey of India 2015–2016 identified a substantial treatment gap in mental healthcare, emphasizing the urgent need for improved training of primary care doctors (PCDs) in managing psychiatric disorders. This study aimed to evaluate the effectiveness of three digitally delivered primary care psychiatry courses offered by the department of psychiatry in a tertiary neuropsychiatric center: the Certificate Course in Primary Mental Healthcare (CCPMH), the Diploma in Community Mental Health (DCMH), and the Diploma in Primary Care Psychiatry (DPCP).
Methods:
Based on the board of studies documents, including curriculum, delivery methods, accreditation criteria, and outcomes, a comparative and thematic analysis of the courses was conducted.
Results:
The digital courses differed in duration, depth, and delivery methods. The DPCP, the most intensive and personalized program, was highly effective in translating knowledge into clinical practice. The CCPMH provided a foundational, short-term course for PCDs, while the DCMH covered a broader range of topics relevant to primary care psychiatry, supplemented with self-learning modules. All courses significantly contributed to reducing the mental health treatment gap by training a substantial number of PCDs.
Conclusions:
Digitally delivered courses are essential in addressing the mental health treatment gap in India. The DPCP, with its emphasis on practical training and personalized learning, demonstrates high effectiveness in equipping PCDs with the necessary skills to manage psychiatric disorders. However, further research is needed to evaluate long-term outcomes and to address the scalability and accessibility challenges of these.
Key Messages:
The National Mental Health Survey of India reported a prevalence of psychiatric disorders at 10.6%, coupled with an 83% treatment gap. 1 In recent years, the critical role of primary care doctors (PCDs) in addressing mental health issues, particularly in resource-constrained settings where specialized psychiatric services are limited, has gained increasing recognition. To bridge this gap and equip PCDs with the necessary skills and knowledge to identify and manage psychiatric disorders effectively, several educational initiatives have emerged.
The Telemedicine Centre, established in 2007, provides remote psychiatric consultations and services through telecommunications technology. The Virtual Knowledge Network (VKN), in collaboration with Extension for Community Healthcare Outcomes (ECHO), utilizes a Hub and Spoke model to facilitate tele-mentoring for mental health professionals. 2 Tele-mentoring via tele-ECHO clinics has proven feasible and effective in training remote PCDs in drug addiction management (including diagnosis and treatment), significantly enhancing their knowledge, confidence, and engagement through both synchronous and asynchronous learning components.
Section 31 of the Mental Healthcare Act 2017 mandates that the appropriate government address human resource needs for mental health services by developing and implementing educational and training programs in collaboration with higher educational institutions. This initiative aims to increase the number of mental health professionals and improve their skills. Additionally, the government is required to train all medical officers in public healthcare and prisons to provide basic and emergency mental healthcare. 3 The government must also strive to meet internationally accepted guidelines for the number of mental health professionals within 10 years from the act’s commencement. In 2018, our center was established to focus on digital education and training in mental health. The courses offered by our center are designed to empower PCDs with evidence-based practices in primary care psychiatry. These courses are accredited by the statutory bodies and are recognized by the National Medical Commission (NMC) of India for MBBS-qualified doctors as per National Institute of Mental Health and Neurosciences (NIMHANS) Act 2012. 4
Our center offers one short- and two intermediate-term digitally driven primary care psychiatry courses: the Certificate Course in Primary Mental Healthcare (CCPMH—2 months), the Diploma in Community Mental Health (DCMH—6 months), and the Diploma in Primary Care Psychiatry (DPCP—1 year). The vision of these courses is to empower MBBS doctors (trainees) to provide first-line treatment for highly prevalent psychiatric disorders in primary care settings using digital technology without requiring deputation to tertiary medical educational institutes and with minimal disruption to their clinical workflow while pursuing the course.
In the 1960s, India launched postgraduate psychiatric courses, but psychiatric care accessibility persisted as a challenge. Short-term training for PCDs was initially contentious but later proved to be effective. 5 Digital innovations, such as our center’s tele-training, bridged gaps in undergraduate education, empowering primary care providers. These initiatives enhanced mental healthcare accessibility and community awareness. Despite recent revisions to the MBBS curriculum, additional training for existing PCDs remains crucial. Our center’s tele-training exemplifies leveraging technology to provide adequate distance education and address this need. These efforts signify progress in integrating mental healthcare into primary care, reducing stigma, and enhancing treatment accessibility. 6
These primary care psychiatry courses for MBBS doctors offered by our center’s digital academy use the “Clinical Schedule for Primary Care Psychiatry” (CSP). This is an adopted and validated point-of-care all-in-one manual specifically tailored for PCDs to provide a structured framework for screening, diagnosing, follow-ups, taxonomy, referral points, and managing (including diagnosis and treatment) six high-prevalent psychiatric disorders in primary care settings. 7 Developed by experts in the field, the CSP ensures that PCDs are equipped with the necessary tools to address tobacco addiction, alcohol-related disorders, psychotic disorders, somatization disorders, anxiety disorders, and depressive disorders (abbreviated as TAP SAD) effectively. It is periodically updated and revised to meet the needs of PCDs, with CSP 2.4 (September 2023) being the latest version.
Furthermore, integrating a learning management system (LMS) facilitates online remote e-learning, making the courses accessible to a broader audience across geographical locations. Through a blend of didactic lectures, case discussions, interactive sessions, and self-assessment quizzes, participants engage in a dynamic learning experience that combines theoretical knowledge with practical application. Clinical hands-on training is a key component in the courses, which includes instant-collaborative video consultation (i-CVC) and tele-psychiatric on-consultation training (tele-OCT). The course employs adult learning principles to ensure adequate comprehension and application by primary care providers. By shedding light on the strengths and areas for the improvement in these educational initiatives, we hope to contribute to the ongoing efforts to enhance primary care psychiatry education and ultimately improve mental healthcare delivery at the grassroots level. 8 The significant advantage of these digitally driven courses is that there is no deputation to medical colleges for courses, and training occurs while they regularly work in their hospitals (employer-friendly courses). The CCPMH, DCMH, and DPCP courses are flexible and can be done part-time, modular-based, and need-based. Additionally, personalized modules are offered in DCMH and DPCP.
This study aims to provide comprehensive information about three digitally driven primary care psychiatry courses offered by our center’s digital academy. This will enable prospective candidates to make informed decisions and select the most suitable course using a cafeteria approach. The objectives are to conduct a theme-based analysis of the three courses and report on their performance audit.
Methods
The need for three distinct courses in primary mental healthcare offered by our center’s digital academy arose from several factors: catering to the diverse requirements of PCDs, the needs of the State government, offering flexible learning options, implementation of DMHP, addressing diverse community needs, and strategically scaling mental healthcare capabilities and the overarching goal of bridging the mental health treatment gap in India.
After five years of offering three primary care psychiatry courses, this comparative study aims to analyze the CCPMH, the DCMH, and the DPCP course provided by our center’s digital academy. The study employed an organized methodology to evaluate these courses through a comprehensive review of the board of studies documents for each course, focusing on various themes, delivery methods, curriculum, and accreditation criteria to identify their respective strengths and weaknesses. Additionally, a performance audit was carried out using data from file reviews and registers, analyzing enrollment and completion rates. The performance audit involved collecting and analyzing data (till December 2023) on enrollment and completion rates. This provided insights into the popularity and success of the courses in terms of participation and the ability of enrolled doctors to complete the training. The audit also helped identify trends and patterns in enrollment, which could indicate the courses’ accessibility and appeal to PCDs across different regions and settings. Overall, this comprehensive and organized analysis aimed to provide a clear understanding of how each course contributed to addressing the mental health treatment gap in India by enhancing the capabilities of PCDs.
Further, Pahuja et al. introduced two novel methods of evaluating the effectiveness of a training method called the translational quotient (TQ) and primary care psychiatry quotient (PCPQ) to assess skill acquisition. TQ measures the acquisition of practicing psychiatric clinical skills among PCDs in real-world primary care settings in their clinic after the particular training method. It evaluates a training program’s effectiveness in translating taught knowledge into practical clinical skills essential for early diagnosis and first-line treatment by PCDs. For the DPCP course, the TQ was assessed through evaluation live tele-OCT sessions conducted by a tele-psychiatrist (trainer) six and nine months after the course began. 9 In other words, the tele-psychiatrists observed live video consultations of five consecutive general patients, or two patients were diagnosed with psychiatric disorders. Further details of TQ assessment are described elsewhere.9,10 These sessions involved live video streaming of real-time outpatient consultations. PCPQ is defined as the proportion of psychiatric cases among total general patients of PCDs. It may be equated with a prevalence of psychiatric disorders in primary care. 9
This is a medical audit-based study of the training curriculum and is exempted from the ethical review as per the Indian Council of Medical Research’s (ICMR) National ethical guidelines for Biomedical and Health Research involving human participants (2017, p. 36). Our institute follows the ICMR guidelines for ethical review. 11
Results
The three courses, CC-PMH, D-CMH, and DPCP, employ varied delivery methods to enhance the clinical skills of PCDs in managing patients with mental illnesses. Each course incorporates both onsite and online/digital training components to cater to different learning preferences and schedules. Online training includes live virtual classroom (VCR) sessions, recorded videos, and interactive case discussions. Live clinical point-of-care / hands-on training methods, such as i-CVC (where a PCD can consult a psychiatrist at any time for a collaborative approach to treating patients) and tele-OCT (where PCDs and Psychiatrists collaboratively screen general patients for mental health issues) are integral to the training process.
While the CCPMH and DPCP courses include both online and onsite training, the DCMH course is entirely online. The DCMH course also incorporates self-paced learning via LMS, providing participants with the flexibility to access course materials at their convenience. This component spans 12 hours and includes tailored manuals for PCDs and expert-led videos covering clinically relevant subjects. Clinical hands-on training is a key component of both the DPCP and CCPMH courses. Additionally, the CCPMH includes a virtual case conference component with actual patients (with their consent). Among the three courses, the DPCP is the most intensive and personalized. Table 1 highlights the unique delivery methods utilized in each course.
Delivery Methods in the Three Digitally Driven Primary Care Psychiatry Courses.
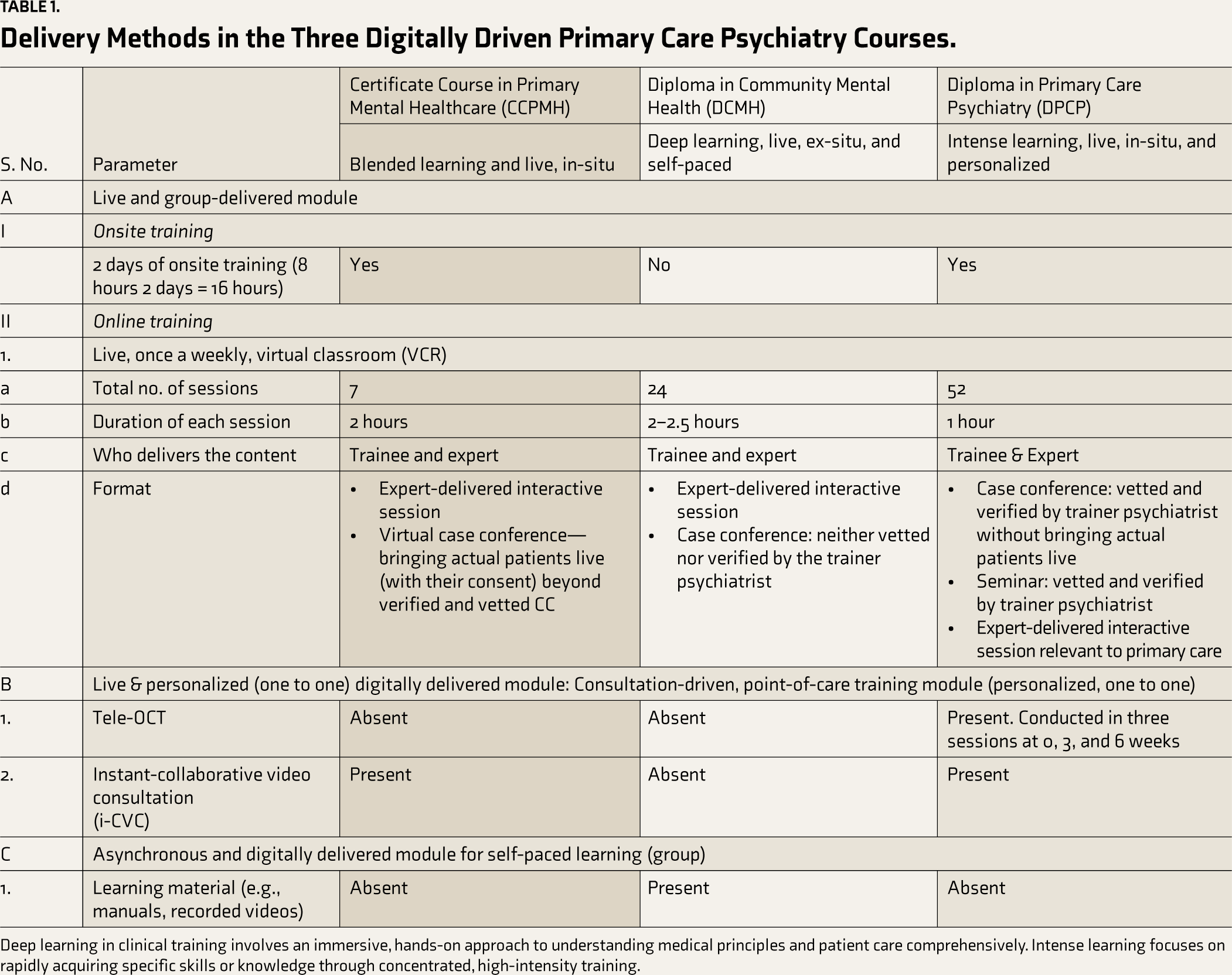
Deep learning in clinical training involves an immersive, hands-on approach to understanding medical principles and patient care comprehensively. Intense learning focuses on rapidly acquiring specific skills or knowledge through concentrated, high-intensity training.
All three courses cover modules on the identification (including screening and diagnosis) and first-line management (including diagnosis and treatment) of TAP SAD; however, there are variations in the topics covered. The DCMH course has a broader curriculum, including dedicated modules on the basics of psychiatric evaluation (such as history taking and mental status examination) and brief non-pharmacological interventions, which are not included in the other courses. Modules addressing mental illness in special populations, including children and the elderly, are covered in both the DCMH and DPCP courses. Optional modules are available in the DCMH and DPCP courses, such as those on cannabis use disorders and opioid use disorders, allowing for a personalized learning experience. These additional modules are tailored to the specific needs of participating doctors who regularly encounter relevant patients in their day-to-day practice. All three courses are primarily delivered in group settings, although the DPCP also offers the option of individual (one-on-one) instruction based on demand.
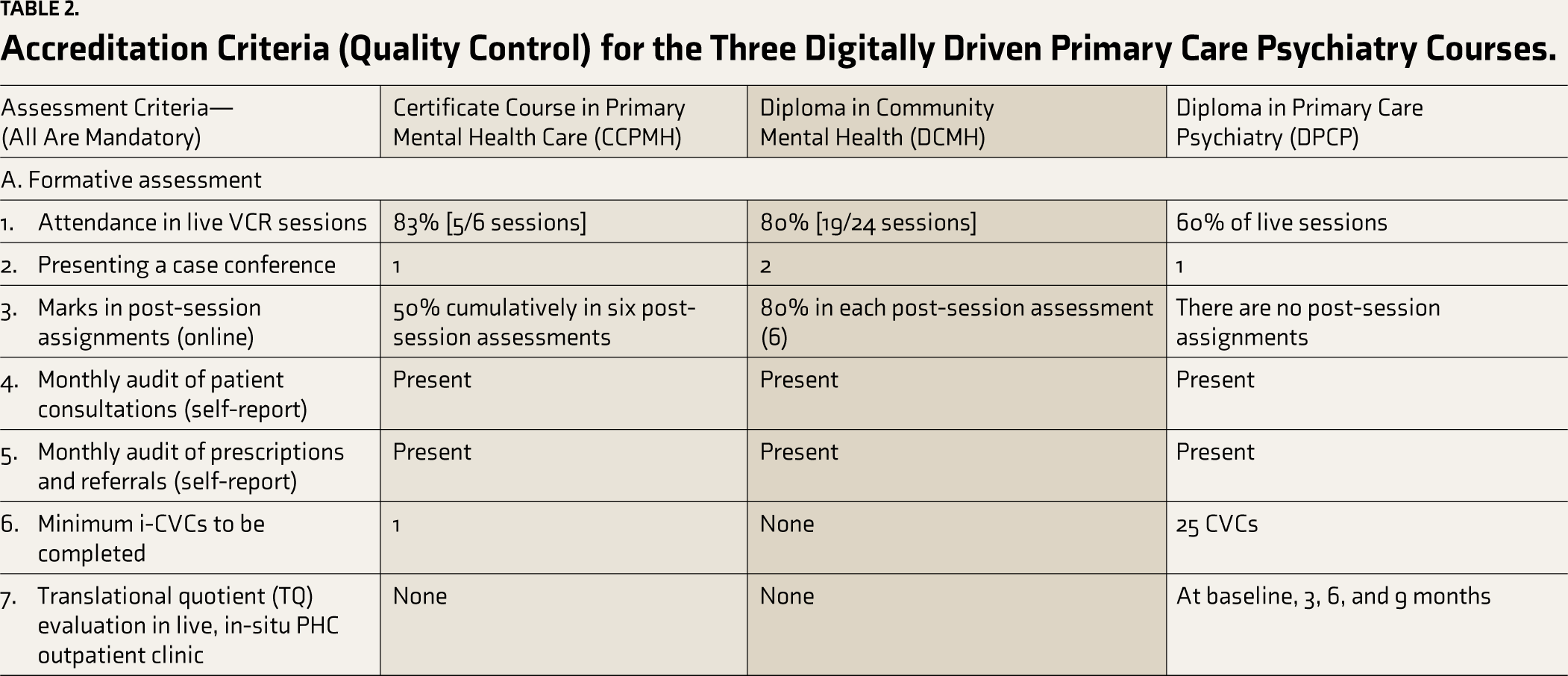
Accreditation criteria play a crucial role in ensuring standardized education. Formative and summative assessments are used for accreditation in DPCP and CCPMH courses, while the DCMH course only uses formative assessments. Table 2 highlights the accreditation criteria for the three courses.
Accreditation Criteria (Quality Control) for the Three Digitally Driven Primary Care Psychiatry Courses.
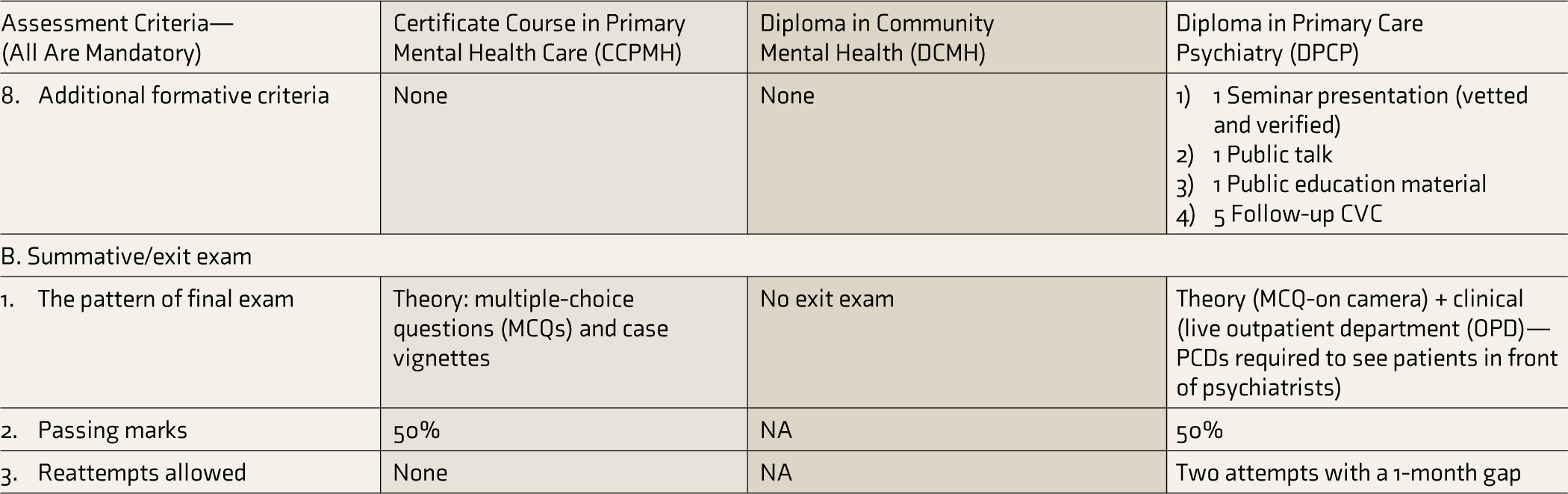
We assessed the number of doctors enrolled and accredited, CVCs conducted, and monthly audits of patient interactions, prescriptions, and referrals made during the course. All three courses have trained a substantial number of PCDs.
Pahuja et al., in their assessment of the DPCP-trained doctors, opined that a PCPQ of around 30% may be considered adequate for a primary care psychiatry training program. 9 The diagnostic concurrence with tele-psychiatrists was notably high in the DPCP course, indicating robust diagnostic accuracy and agreement. However, it is essential to note that some parameters, such as PCPQ and diagnostic concurrence, were not assessed in other courses. Table 3 outlines the achievements of the three courses till December 2023.
Performance Audit/Achievements Till December 2023 for the Three Digitally Driven Primary Care Psychiatry Courses.
aThis is based on the preliminary assessment of self-reported data by trained doctors and is indicative.
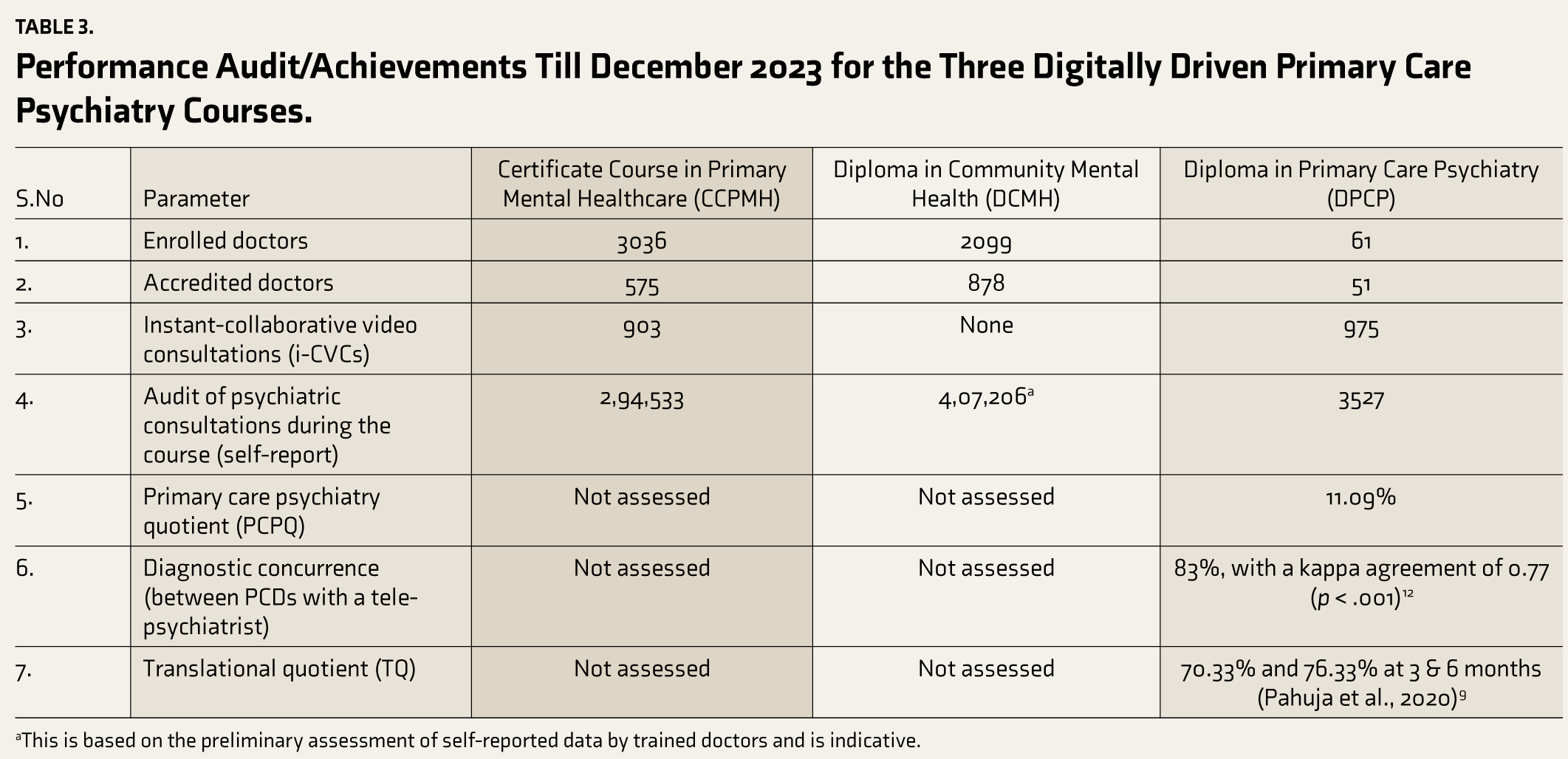
The CCPMH offers a two-month foundational course with 30 hours of training that combines both onsite and online training. The DCMH provides an in-depth course extending over six months, with 60 hours of training that is entirely online with an element of self-learning through LMS. The DPCP course offers the most comprehensive, intense, and personalized training, lasting one year and spanning 125 hours, featuring a blend of online and onsite training. The DPCP course offers extensive practical training and hand-holding from experts throughout the training period and accommodates both group and individualized learning styles. While the CCPMH and DPCP cater primarily to government doctors, the DCMH cater to doctors from both the government and private sectors. PCDs can utilize this information to guide their choices through a cafeteria approach. Table 4 presents a comparative overview of three primary care psychiatry courses.
Highlights of the Three Digitally Driven Primary Care Psychiatry Courses.
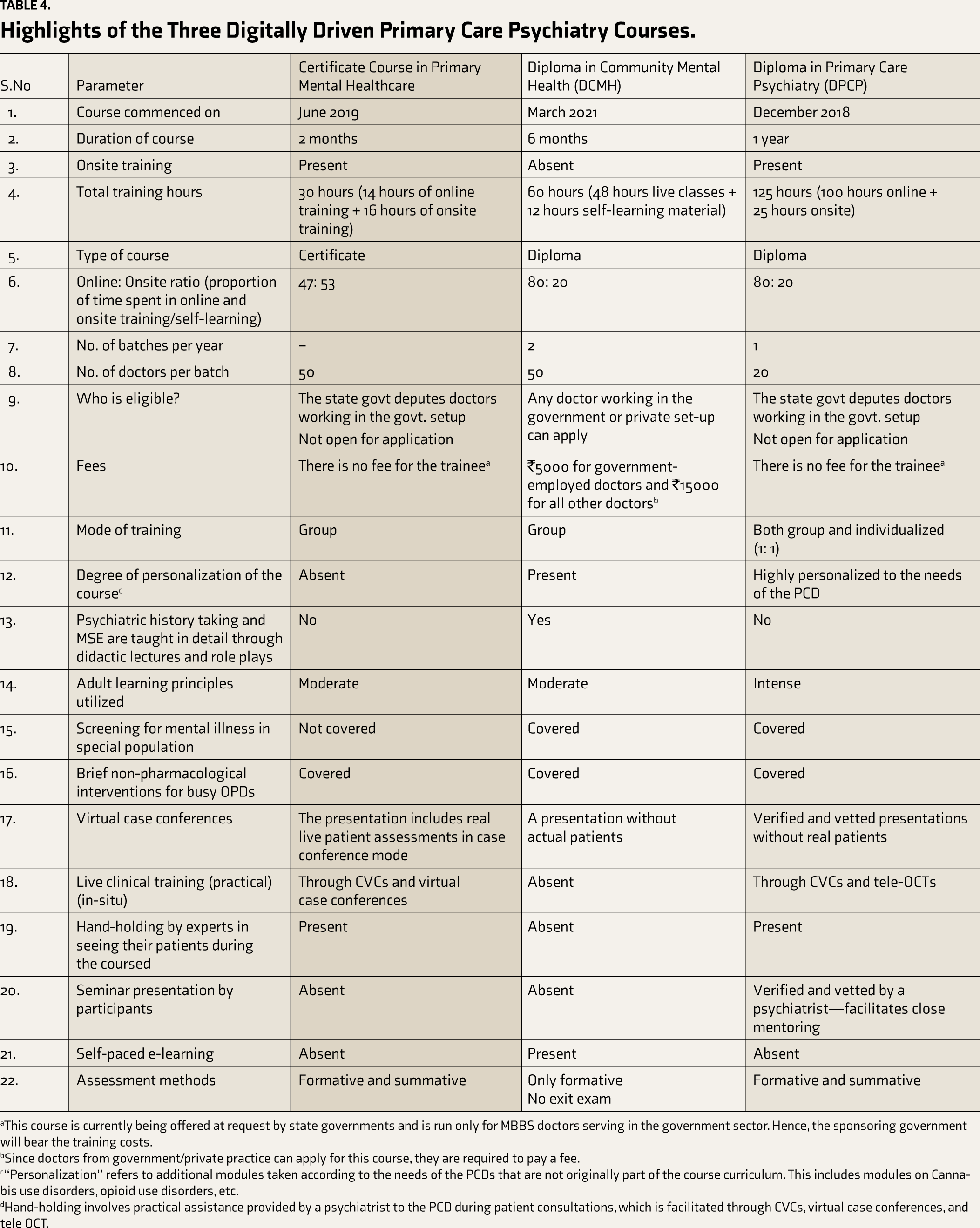
aThis course is currently being offered at request by state governments and is run only for MBBS doctors serving in the government sector. Hence, the sponsoring government will bear the training costs.
bSince doctors from government/private practice can apply for this course, they are required to pay a fee.
c“Personalization” refers to additional modules taken according to the needs of the PCDs that are not originally part of the course curriculum. This includes modules on Cannabis use disorders, opioid use disorders, etc.
dHand-holding involves practical assistance provided by a psychiatrist to the PCD during patient consultations, which is facilitated through CVCs, virtual case conferences, and tele OCT.
Discussion
The three courses offered by our center’s digital academy, CCPMH, DCMH, and DPCP, demonstrate considerable variation in structure, duration, and depth, effectively catering to the diverse training needs of PCDs. The CCPMH, focusing on foundational knowledge, combines onsite and online training over two months, benefiting government doctors by blending theoretical and practical learning without disrupting clinical duties. The DCMH provides a comprehensive six-month online training, addressing broader mental health needs with an in-depth syllabus that includes psychiatric evaluations and non-pharmacological interventions. The DPCP, with its intense and personalized approach, spans one year and includes extensive hands-on clinical training through methods like CVC and tele-OCT.
Blended learning approaches, which combine online and face-to-face instruction, are effective in medical education. A meta-analysis by Cook et al. found that blended learning is associated with higher knowledge acquisition and learner satisfaction than traditional learning methods, supporting the design of our center’s courses, particularly the CCPMH and DPCP. 12
Integrating various delivery methods, including live VCR sessions, recorded videos, and hands-on clinical training, highlights the effectiveness of blended learning in enhancing the training of primary care providers. CVC and tele-OCT in the DPCP course provide a robust framework for real-time skill application and feedback, ensuring that PCDs can translate theoretical knowledge into practical skills. This aligns with the findings by Jayasankar et al., who emphasized the importance of live clinical training in enhancing practical skills among PCDs. Additionally, the CCPMH’s inclusion of virtual case conferences with actual patients and the DPCP’s seminar presentations vetted by trainer psychiatrists underscore the significance of experiential learning, which is critical for skill acquisition and retention. 13
The value of practical training in medical education is well-documented. For instance, Kneebone et al. highlighted that simulation-based training enhances the procedural skills of medical students and professionals, leading to improved patient outcomes. This supports the hands-on approach of the DPCP, which incorporates simulation and real-time consultation components. 14 Furthermore, the Chhattisgarh Community Mental Healthcare tele-mentoring program (CHaMP) demonstrated that digitally driven initiatives can effectively reach and train remote healthcare providers, enhancing their ability to manage mental health conditions in underserved areas. 15
e-learning courses in medical education, particularly those with interactive elements, have been found to enhance knowledge retention and application. This supports the effectiveness of our center’s use of blended learning and interactive training modules. The DPCP’s high TQ scores at six and nine months indicate its effectiveness in translating taught knowledge into practical clinical skills essential for early diagnosis and first-line treatment by PCDs. Based on the success of the DPCP, a new course, the Diploma in Prison and Correctional Psychiatry for Practicing Medical Officers, has been introduced recently. This course has successfully trained two batches of medical officers in the Bihar prisons.
The adaptability of these courses to diverse groups of doctors, including those from government and private sectors, is crucial for addressing the mental health treatment gap in India. The DPCP course specifically targets state government doctors with sponsorship, ensuring that those serving in rural and resource-constrained settings receive adequate training. This is vital for enhancing mental healthcare accessibility across diverse geographical locations, as evidenced by significant enrollment numbers across all courses. The flexibility of these digitally driven courses allows PCDs to integrate training with their clinical duties, thereby minimizing disruptions and enhancing learning outcomes. 16
The importance of adaptable and scalable training programs in healthcare has been emphasized in various studies. For instance, Frenk et al. argued for transformative educational approaches that are flexible and context-specific to meet the evolving needs of healthcare systems globally, supporting the design and implementation of these courses tailored to the needs of Indian PCDs. 17
Continuous feedback mechanisms between trainers and participants are integral to the success of these courses, ensuring that the courses remain relevant and responsive to participants’ needs. High enrollment numbers and positive participant feedback reflect a critical demand for specialized training in primary care psychiatry, corroborating the findings of Gangadhar, who emphasized the growing need for mental health training programs for PCDs. 6 Continuous feedback in medical education has been shown to improve learning outcomes and professional development. A study by Veloski et al. demonstrated that formative feedback enhances clinical performance and competencies, highlighting the importance of feedback mechanisms in these courses. 18
Despite the success of these courses, several limitations need to be addressed. The reliance on self-reported data and potential bias from the authors’ affiliation with the center may affect the validity of the findings. Additionally, there is a lack of data on long-term skill retention, application in general practice, how many patients really benefited, decrease in disability, increase in ability, and cost-effective analysis. Future research should incorporate tele-OCT and TQ assessments into the CCPMH and DCMH, standardize accreditation criteria across courses, and explore hybrid learning models. Conducting cost-effectiveness analyses, developing a condensed version of the DPCP, establishing mentorship and support systems, and incentivizing course completion for government medical officers could enhance the scalability and accessibility of these programs. Additionally, reliability can also be an issue; an outside audit may be recommended. Additionally, the integration of artificial intelligence in psychiatry education could catalyze further advancements in this field. 19
Conclusion
Our center’s digitally driven courses effectively address India’s mental health treatment gap by equipping primary care providers with essential skills. These courses demonstrate the importance of blended and practical learning approaches in medical education. Evaluating the long-term impact of these courses on patient outcomes and the sustainability of acquired skills through longitudinal studies and standardized patient assessments is crucial. Addressing these limitations and implementing the proposed recommendations can further optimize these training programs, ensuring their effectiveness in equipping PCDs with the necessary competencies to manage mental health conditions in their communities.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
Thanks to staff at NIMHANS Digital Academy and doctors who have been trained in these three courses.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
Generative artificial intelligence (AI) has been used to enhance language, and the authors take full responsibility for the text generated in the manuscript.
Ethical approval
The Institutional Ethics Committee provided exemption from the ethical review as per the Indian Council of Medical Research’s (ICMR) National ethical guidelines for Biomedical and Health Research involving human participants (2017, p. 36).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.