
Abstract
Psychiatric disorders were among the top 10 causes of disease-related burden worldwide in 2019, with no reduction compared to past years. 1 Psychopharmacology, the cornerstone of managing psychiatric disorders, has been in crisis with little new drug development in the past two to three decades, highlighting the need for new treatments. 2 Clinical neuroscience aims to understand psychiatric disorders at an individual level, from genes to neurocircuitry to brain function and seeks to find new treatments through translational research. 3 In psychiatry, the treatment gap is significant, with around 80% of cases in India and worldwide not receiving adequate care.4,5 Neuroscience-informed interventions can effectively bridge the treatment gap and complement the global mental health approach, which focuses on community-level impact and treatment availability. 3 Procedural treatments, rather than conventional medications and therapy, are increasingly being used in psychiatry. As “interventionism” is becoming common in other branches of medicine, the same approach is being adopted in psychiatry, thus giving birth to a new subspecialty called interventional psychiatry (IP).6,7 IP treatments, informed by advancements in neuroscience and technology, enhance our understanding of the brain-based etiology of psychiatric disorders. 8 This viewpoint discusses the current conceptualization of IP, its clinical scope, the need for specialized training, and its future evolution.
Defining Interventional Psychiatry
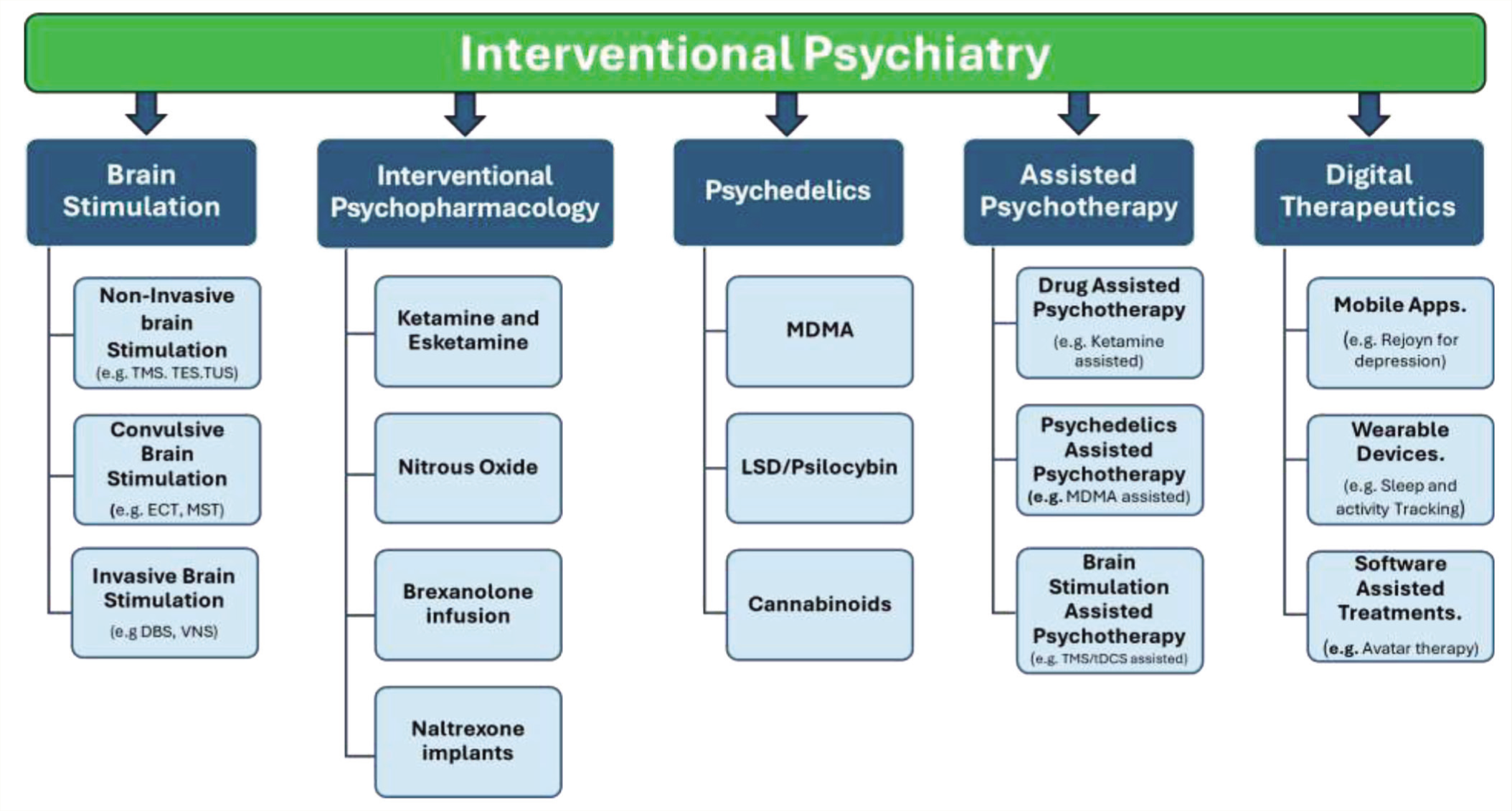
Williams et al. 9 introduced the concept of IP as an emerging subspecialty that uses neurotechnologies to identify and modulate dysfunctional brain circuitry underlying psychiatric disorders. They highlighted brain stimulation treatment as IP’s core component due to its promising results in treating neuropsychiatric disorders. However, IP extends beyond brain stimulation. Padberg et al. 10 suggested that newer psychopharmacological agents (e.g., ketamine and nitrous oxide), psychedelics, enhanced psychotherapies, and digital interventions also fall under IP, as these treatments are more procedural than conventional psychiatric methods. Therefore, we propose a broader definition of IP: Interventional psychiatry refers to procedural treatments in psychiatry using advancements in clinical neuroscience and technology, including brain stimulation, psychopharmacological interventions, psychedelics as therapeutics, assisted psychotherapies, and digital therapeutics. Due to the innovative nature of these interventions, standardized protocols, specialized training, and potential certification are necessary for practitioners (see Figure 1).
Interventionism in Psychiatry: A Historical Perspective
Procedural treatments in psychiatry have ancient roots, with evidence of crude psychosurgeries for treating psychiatric disorders dating back to the Neolithic era. In the 1800s, there was a resurgence of psychosurgeries, including controversial procedures such as prefrontal leucotomies and lobotomies. 11 Early procedural treatments also included malaria therapy, insulin coma therapy, and chemical convulsive therapy. However, electroconvulsive therapy (ECT), introduced in the early twentieth century, revolutionized psychiatric treatment and remains the most effective treatment for depression. The development of procedural treatments stagnated during the psychopharmacological revolution. In the 1980s, when pharmaco-resistance became a significant concern and understanding of neurobiology improved, new brain stimulation treatments such as transcranial magnetic stimulation (TMS) and transcranial electrical stimulation (tES) were introduced. These treatments proved effective for resistant psychiatric disorders and led to the development of IP as a subspecialty. 11
The Need for Interventional Psychiatry as a New Subspecialty
There have been no groundbreaking discoveries in psychopharmacology in the last two decades.12,13 Although effective in reducing symptoms, up to 75% of individuals may experience adverse effects from psychotropics, significantly affecting their quality of life.14,15 Treatment resistance is another major concern, with 30%–60% of people with common mental disorders responding poorly to conventional treatments. 16 Factors contributing to this resistance include the poor understanding of illness etiologies, the absence of personalized treatments, and a lack of precise interventions targeting circuit-level dysfunctions. Therefore, more effective, safe, and neurobiology-informed treatments are needed to address tolerability issues and treatment resistance in psychiatry.
Developing IP as a new subspecialty has academic significance. Williams et al. 9 highlighted the need for training psychiatry residents in circuit-based neuroscience and brain stimulation. Brunoni et al. 17 enlisted 13 reasons for developing IP as a subspeciality, including clinical implications, resident training, and research.
The Current Scope of Interventional Psychiatry Treatments in Clinical Practice
In Figure 1, we summarize the different treatments included under the broad umbrella of IP, which are briefly explained in the following sections. Some of these treatments have already been approved for various conditions, while others are still in the experimental stage. However, the scope of IP is expanding rapidly.
Different Interventions Under the Interventional Psychiatry Umbrella.
Brain Stimulation Treatments
Brain stimulation treatments form the backbone of IP, showing consistent efficacy in various disorders (Table 1) and gaining approval from agencies like the Food and Drug Administration (FDA). 18 Brain stimulation is classified based on invasiveness and type of stimulation. Noninvasive brain stimulation (NIBS) techniques are further classified as seizure (convulsive) or nonseizure (nonconvulsive).
Indications for Different Brain Stimulation Treatments.
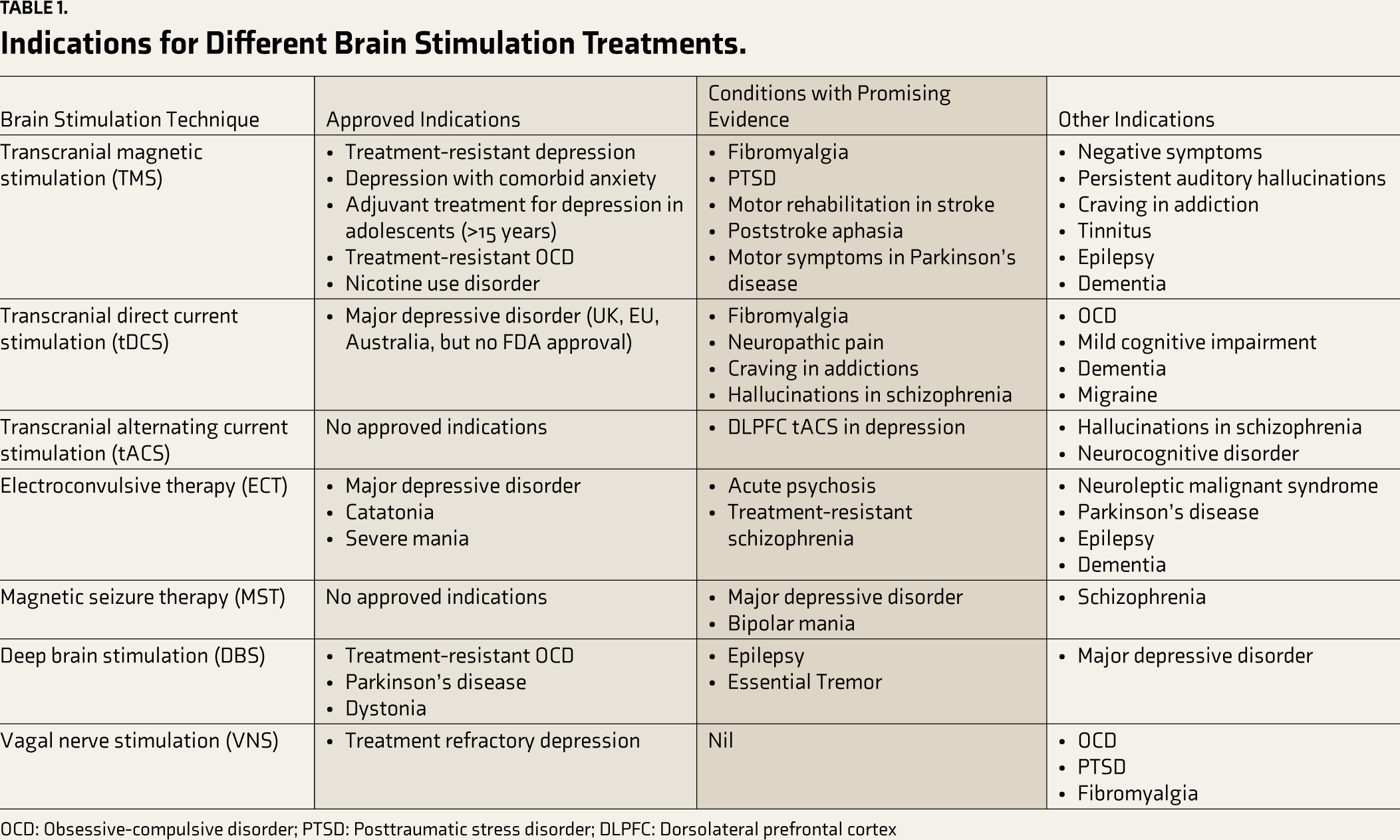
OCD: Obsessive-compulsive disorder; PTSD: Posttraumatic stress disorder; DLPFC: Dorsolateral prefrontal cortex
Noninvasive Brain Stimulation
NIBS treatments include TMS, tES, transcranial-focused ultrasound (TUS), and transcranial photobiomodulation (tPBM). TMS—FDA-approved for depression, obsessive–compulsive disorder (OCD), and nicotine use disorder—is a safe and promising treatment for neuropsychiatric disorders, showing consistent real-world effectiveness.19–22 Novel TMS protocols, such as accelerated TMS and personalized functional magnetic resonance imaging-guided Stanford neuromodulation treatment, demonstrate superior efficacy than ECT for depression without cognitive adverse effects. 23
Transcranial direct current stimulation (tDCS) is the most studied tES method, offering a safe and promising treatment for depression, auditory hallucinations in schizophrenia, craving in substance use disorders, and more.24,25 Though not FDA approved, its portability, ease of use, and potential for home-based treatments make it cost-effective. However, more robust evidence is needed for its routine clinical use. Innovations such as high-definition tDCS (HD-tDCS) provide more targeted stimulation and show promise, as indicated by early systematic reviews. 26 Dynamic tES treatments such as transcranial alternating current stimulation and transcranial random noise stimulation can modify abnormal neuronal oscillations and influence brain functions, suggesting their potential for personalized interventions.27,28 The clinical uses of tES are summarized in Table 1.
New forms of NIBS, such as tPBM, use red (620–700 nm) and near-infrared (780–1270 nm) light to induce changes in neuronal plasticity through mitochondrial-mediated mechanisms. Early evidence confirms its safety and suggests potential therapeutic applications in neurology and psychiatry. 29 Similarly, low-intensity (<100 W/cm2) focused ultrasound, called tFUS, allows for deeper brain targeting. Animal studies have confirmed its safety, and initial research on healthy controls indicates that tFUS can modulate both excitatory and inhibitory brain properties. 30 Preliminary findings show its potential therapeutic benefits in chronic pain and dementia. 30
Convulsive Brain Stimulations
Despite being noninvasive, ECT and magnetic seizure therapy (MST) induce seizures and require general anesthesia. Thus, they are classified separately. Introduced in 1938 in Italy, ECT is one of the oldest biological treatments in psychiatry and the earliest form of interventional treatment. 31 Today, even nearly a century later, ECT remains the most effective treatment for depression and is also recommended for acute mania, suicidality, and catatonia, often providing rapid improvement and sometimes lifesaving. Innovations like ultra-brief pulse width (<0.5 ms) and unilateral electrode placement reduce ECT’s cognitive adverse effects. 32 Ongoing research focuses on improving ECT tolerability with newer modifications such as focal electrically applied seizure therapy, low amplitude ECT, fronto-medial ECT, and individualized low amplitude seizure therapy. 33
MST is a novel convulsive therapy using high-intensity magnetic pulses (100 Hz) applied over the cortex with an especially designed TMS coil, avoiding direct electrical stimulation and the cognitive adverse effects associated with ECT. Studies indicate that MST has comparable efficacy to ECT in treating major depressive disorder (MDD) with significantly lower cognitive risks. 34
Invasive Brain Stimulations
New invasive brain stimulation methods, such as deep brain stimulation (DBS) and vagal nerve stimulation (VNS), offer hope for treating refractory neuropsychiatric disorders. DBS targeting the ventral capsule was approved by the FDA in 2009 for refractory OCD and has shown promise in treating refractory depression. 35 VNS is approved by the FDA for treatment-resistant epilepsy and depression and has also shown efficacy in OCD, anxiety disorders, and dementia. Additionally, a newer noninvasive form of VNS, called auricular VNS, stimulates the auricular branch of the vagus nerve externally and shows promising results. 36
Interventional Psychopharmacology
Procedural treatments requiring specialized training are emerging in psychopharmacology and fall under the IP umbrella. Ketamine, a leading medication in this group, originally an anesthetic, has shown therapeutic potential in depression and beyond. It can be administered via intravenous infusion, intranasal spray, oral, and subcutaneous routes. Intranasal esketamine was approved by the FDA in 2019 as an augmentation treatment for treatment-resistant depression and is used off-label for acute suicidality, bipolar depression, OCD, posttraumatic stress disorder (PTSD), and borderline personality disorder. 37 Another promising medication is inhalational nitrous oxide that has shown initial efficacy in depression trials, sustaining mood improvement for up to a month. 38 Brexanolone infusion, a synthetic neurosteroid, is the first FDA-approved drug for postpartum depression. It is administered as a slow infusion over 60 hours with rapid antidepressant effects. Most patients achieve a response within 24–36 hours, making it an ideal antidepressant for conditions with significant health risks for the mother and baby. 39 Naltrexone, an opioid receptor antagonist, is available as a subcutaneous implant for opioid use disorder, offering improved long-term outcomes compared to oral forms. 40
Psychedelics as Therapeutics
Once considered drugs of abuse, psychedelics now offer new hope for treating various psychiatric disorders. 3,4-Methylenedioxymethamphetamine (MDMA) is leading psychedelic research and has shown efficacy in reducing PTSD symptoms in initial clinical trials. 41 Drugs such as psilocybin and lysergic acid diethylamide are also being researched for their potential therapeutic roles in depression, anxiety disorders, and substance use disorders, with early promising evidence. 42 A better understanding of the human endocannabinoid system has also opened up potential uses for cannabinoids in psychiatry. Thus, psychedelics represent significant promise in the field of psychiatric treatments, although they may require special arrangements and monitoring, falling under IP.
Assisted Psychotherapies
Evidence-based psychotherapies can be combined with psychopharmacological agents or NIBS interventions, either sequentially or concurrently, to improve treatment outcomes—a practice known as assisted psychotherapies.43,44 Psychedelic-assisted psychotherapy using MDMA has shown promising evidence in treating PTSD and is currently seeking FDA approval. 45 Similarly, agents such as psilocybin and ketamine have been integrated with structured psychotherapies for depression and anxiety disorders, showing early promising results.43,46 TMS and tES can also be effectively combined with psychotherapy, creating a bidirectional interaction that enhances outcomes in depression, OCD, and PTSD treatments. 44
Digital Therapeutics
Digital therapeutics (DTx) leverages advances in digital and information technology to innovate treatments for psychiatric disorders. In the last decade, research related to DTx in healthcare has surged, with over 32 trials registered on ClinicalTrials.gov. 47 DTx includes text message services, smartphone applications, online tools, wearable devices, and software. Recently, the FDA approved Rejoyn™ as the first prescription DTx for adjunctive treatment of MDD in the United States, following a clinical trial that demonstrated superiority over control treatments using a digital cognitive-emotional training regimen. 48
Virtual reality (VR) technologies are increasingly used to treat psychiatric disorders, especially for exposure therapy in anxiety disorders, PTSD, and addiction, which strongly support their efficacy. 49 VR also aids cognitive training in dementia and social skill training in autism spectrum disorder. 49 Avatar therapy, using VR, has shown efficacy in treating persistent hallucinations in schizophrenia. 50 Wearable devices such as smartwatches, rings, and wearable ECG and EEG can monitor stress, anxiety, sleep quality, and treatment response, with potential for broader applications. 51 The growing interest in artificial intelligence and machine learning in healthcare is also evident in mental health, aiding in early detection and diagnosis and predicting treatment responses or relapses. 52 Given that many of these interventions require specific training and supervision, they are classified under the umbrella of IP.
The Need for Residency Training and Competency in Interventional Psychiatry
As a new subspeciality, IP requires specialized training programs to equip psychiatry residents and practicing psychiatrists with the skills to administer these new treatments. Recent surveys found that only a small percentage of psychiatry residents felt competent to administer ECT (24.3%) and rTMS (3.1%). 53 Similarly, surveys in China revealed inadequate knowledge and negative attitudes toward TMS among psychiatrists, but those who received formal training had more positive attitudes and higher knowledge levels, underscoring the need for formal training. 54
Many residency programs in the United States have implemented IP tracks to train residents in core competencies through planned clinical rotations and monthly lectures. 55 In Brazil, IP fellows receive three months each in ECT, TMS, tES, and ketamine treatments, alongside other academic activities. 17 Structured training during psychiatry residency is thus feasible and essential for equipping the residents with the necessary skills in IP.
Interventional Psychiatry in the Indian Context
ECT services have been available in India since the 1960s, primarily concentrated in apex institutes and research centers. 56 However, comprehensive data on the number of hospitals offering ECT or the annual procedures performed are lacking, and psychiatrists’ knowledge and attitudes toward ECT remain inadequate. In contrast, institutes such as the National Institute of Mental Health and Neuro Sciences (NIMHANS) and the Central Institute of Psychiatry (CIP) have used TMS for over 20 years, with more institutes now adopting TMS and tES. 7 Recently, NIMHANS initiated multicentre clinical trials through the clinical research center (CRC) for neuromodulation in psychiatry, focusing on brain stimulation treatments for resistant psychiatric disorders. 57 The CRC has also established the Clinical Research Training Program fellowship, a unique formal training initiative for psychiatrists in brain stimulation. 57 Additionally, the Psychiatry Department of Kasturba Medical College, Manipal, offers an exclusive one-month brain stimulation program for psychiatry postgraduate residents.
Data on the clinical use of ketamine in India are limited, despite their use by many institutes and practitioners for depression and other indications, as well as for research purposes. 58 Psychedelic research and clinical use are restricted due to legal limitations under the NDPS Act, which bans these substances. Digital interventions show significant potential in India, particularly in telepsychiatry, following the introduction of a National Tele-Mental Health Program. 59 NIMHANS launched the Tele-Mental Health Assistance and Nationally Actionable Plan through States program to provide free mental health services across India, particularly targeting remote areas. However, psychiatry residents currently lack adequate and uniform training in these interventions due to their limited availability. 7 Thus, research, clinical use, and training in IP are still developing, and challenges are facing India.
Future Prospects of Interventional Psychiatry
The scope of interventions under IP is likely to expand significantly in the coming years, becoming a pivotal treatment option for both psychiatric and neurological conditions. Brain stimulation treatments are advancing toward personalized and closed-loop neuromodulation, ensuring precision, safety, and efficacy. Emerging treatments such as tFUS and tPBM may gain prominence due to their distinct mechanisms of action. MST shows promise as a primary treatment for convulsive brain stimulation, potentially replacing ECT in some cases. Precision psychopharmacology and psychedelics are expected to broaden their therapeutic applications. The field of psychotherapy will evolve with the introduction of assisted techniques. Digital interventions are set for exponential growth, offering cost-effective and accessible options pending regulatory approvals. Staying informed about these developments and acquiring the necessary knowledge and skills to deliver these interventions effectively will be crucial. Developing standardized treatment protocols, formal training programs for residents and practitioners, and establishing certifications and accreditations for IP courses will be essential steps toward achieving these goals and advancing the field.
Conclusion
There are substantial treatment gaps in psychiatry, especially in addressing treatment-resistant conditions. IP offers a new and expanding array of treatments that can significantly impact the understanding and management of these disorders. Brain stimulation treatments have emerged as safe, effective options approved for depression, OCD, and addictions. Other promising interventions within IP include interventional psychopharmacology, assisted psychotherapies, and DTx. It is essential to ensure psychiatry residents, and practitioners are competent in these core IP interventions for effective treatment delivery. IP-focused residency training and fellowships are pivotal in achieving this competency. In India, IP is still emerging, with a primary focus on brain stimulation therapies. There is a critical need to bridge the gap between research and clinical practice and to broaden the scope of IP skills within the country.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the support of the Clinical/Public Health Centre Research Grant from the DBT Wellcome Trust India Alliance (IA/CRC/19/1/610005).