
Abstract
Suicide is a significant adverse outcome of schizophrenia and other severe mental illness. The pioneer psychiatrist Bleuler described that suicidal drive is one of the most severe symptoms of schizophrenia. 1 Suicide is one of the principal causes of loss of life in patients with schizophrenia, and the lifetime risk of death by committing suicide can range from 4.9% 2 to 5.6%. 3 It is also observed that the suicide rate attempts among people with psychosis vary from 10% to 50%. 4 Suicide is noted to be the highest specific cause of mortality in patients with schizophrenia.
Non-suicidal self-injurious (NSSI) behavior infers intentional self-harm 5 and self-imposed damage of body tissue without the intention of dying. 6 In the Indian sample, the lifetime prevalence of NSSI was found to be about 21.4%, with a greater prevalence in women. 7 NSSI in schizophrenia patients is estimated to occur at a higher rate than in the general population. Common methods include cutting, burning, head banging, pricking, scratching, and self-hitting, resulting in injuries that extend from superficial scratches to extreme mutilation of body parts. It also includes behaviors associated with psychotic symptoms, such as hitting oneself due to command hallucinations. 8
Young people are reported to be more likely to carry out NSSI. 9 The research, however, is insufficient to determine whether NSSI varies with age. Additionally, there is conflicting information about whether there is a gender difference in NSSI, with some research suggesting a higher frequency among females 10 and others concluding there is no gender difference. 11 The presence of NSSI in schizophrenia patients has been associated with various factors, including younger age, female gender, comorbid substance use disorders, greater severity of depressive symptoms, and a history of childhood trauma or abuse. 12 There are multiple overlying features between self-injurious behavior and suicidal behavior. There is growing recognition that they are two distinct terminologies with notable differences in causation, impairment, socio-occupational function, course, and the outcome between the two. 13 NSSI behavior is associated with nerve damage, tissue scarring, infections, accidental deaths, emotional distress, and an increased risk of suicide. 14
The existing literature on NSSI in schizophrenia is sparse, with most studies focusing on suicidal behavior rather than non-suicidal self-injury. This case series underscores the need for heightened awareness and targeted interventions for NSSI in schizophrenia. Clinicians should consider comprehensive treatment approaches that address both the psychotic symptoms and the underlying causes of self-injury. By thoroughly exploring these aspects, this case series will contribute valuable insights into the complex interplay between schizophrenia and NSSI. The patients gave written informed consent for the publication of this manuscript and the images.
Case 1
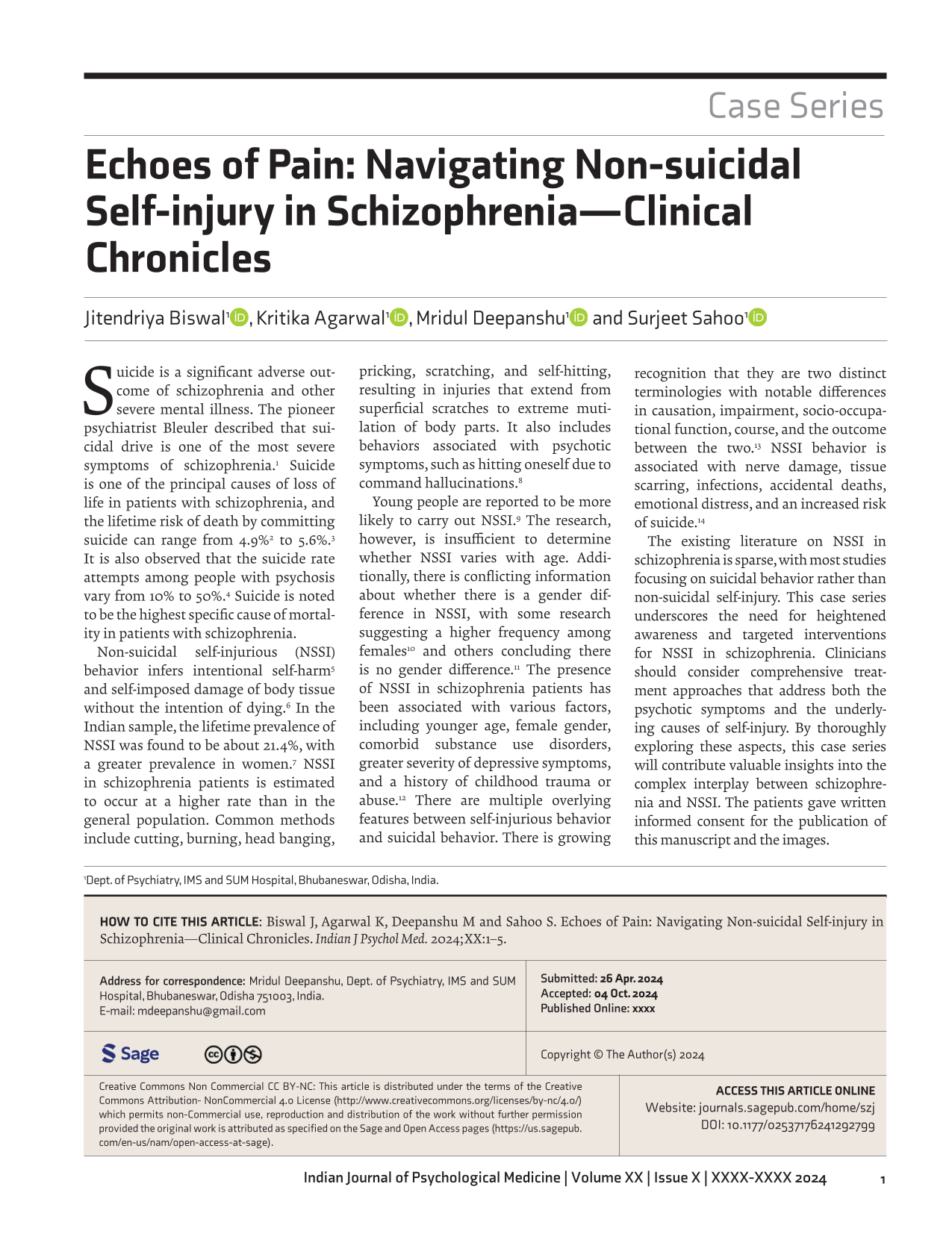
A 37-year-old man from West Bengal educated up to 12th standard and from a middle socio-economic background, presented to the psychiatry outpatient department (OPD) with his wife, referred by the ENT department for mental status evaluation due to recurrent nose bleeds. The patient had been under ENT treatment for three months and underwent multiple tests without finding any physical cause for his complaints. Initially, he believed maggots were inside his nose, leading him to prick his nose, causing injuries repeatedly (Figures 1(A) and 1(B)). Despite ENT interventions, including antibiotics, analgesics, and nasal packing, his symptoms persisted. Rhinoscopy revealed no maggots or internal injury, but the patient remained convinced maggots were present, especially active at night.
The Patient’s Bleeding from the Right Nostril is due to Repetitive Nose Pricking.
During the psychiatric evaluation, it was noted that the patient had been experiencing symptoms for over a year, including suspiciousness, muttering to himself, fearfulness, and auditory hallucinations. He believed that three men were trying to harm him and his family, prompting him to avoid leaving his house and quitting his job. He also occasionally consumed alcohol, cannabis, and nicotine but had been abstinent for nine months. During the interview, it was observed that the patient demonstrated poor insight regarding their self-harm behavior. Despite a thorough examination by the medical team, which found no evidence of maggots and instead identified the presence of self-inflicted injuries, the patient did not accept these findings. The injuries are believed to be part of his delusional beliefs.
Clinically, the patient was cooperative, with normal psychomotor activity and speech. His mood was reported as irritable and congruent with his situation. His thought content revealed a delusional belief about the maggots and a delusion that a neighbor was responsible for his condition due to a past conflict. He also experienced commanding auditory hallucinations, instructing him about the maggots and causing significant distress.
Routine investigations were normal except for a slightly elevated total leukocyte count. Given his psychiatric symptoms, he was diagnosed with Paranoid Schizophrenia (F20.0), as per International Classification of Diseases – 10 (ICD-10) guidelines, 15 and managed on an outpatient basis, as he and his family declined inpatient admission. Treatment included starting Olanzapine, gradually increasing it to 15 mg per day over two weeks, along with a combination of Amoxicillin 1000 mg and clavulanic acid 250 mg per day for five days, and continuing ENT care.
A psychoeducation session was held, and following medication adjustments and follow-ups, his pricking behavior decreased, allowing the nasal injury to heal. After four weeks, notable improvements were observed, although he still felt unmotivated. Escitalopram 10 mg/day was added. Six weeks later, he showed substantial improvement, with reduced delusional beliefs and normalized daily activities. Following psychoeducation and pharmacological intervention, the patient developed insight into his self-harm behavior. Consequently, there was a significant reduction in his nose-picking behavior. The treatment plan and psychoeducation proved effective in managing his condition.
Case 2
A 26-year-old male with no prior psychiatric history presented to the emergency department after an apparent suicide attempt two days earlier. Examination revealed multiple lacerations on his neck and abdomen. Although alert and oriented, he was uncooperative and refused to discuss his injuries. The neck wounds had no active bleeding and showed granulation tissue, while the abdominal incisions were superficial with no active bleeding (Figures 2(A) and 2(B)). His mother reported that he had been behaving abnormally for the past three months after quitting his job at a diamond company in Mumbai due to increasing paranoia and aggression toward his co-workers, whom he believed were conspiring against him. After returning to his village, his condition worsened; he became socially withdrawn, suspicious, irritable, and muttered to himself.
Self-inflicted Multiple Incised Wounds on the Neck and Abdomen, Respectively, of the Patient.

The patient was admitted to the psychiatry ward for further evaluation. Initially uncooperative, he later disclosed hearing voices of men constantly criticizing him and commanding him to harm himself. These voices intensified on the day of the self-inflicted injuries, compelling him to cut himself in an attempt to silence them.
Clinically, the patient appeared thin but with average grooming and hygiene. He maintained a downward gaze during the interview but was cooperative. His vitals were stable. Psychomotor activity and speech were normal, though establishing rapport was challenging. He described his mood as “fine,” but his affect was irritable, congruent with his mood and situation.
The patient harbored delusions that his neighbors and former co-workers were plotting against him and his family. He believed they intended to destroy his home and murder him. These delusions led him to isolate himself at home. He experienced persistent auditory hallucinations, with voices commenting on his actions and urging him to kill himself. These voices, perceived as coming from outside himself, were distressing and beyond his control. No insight into the self-harm behavior was observed during the interview. He was eventually diagnosed as a case of Paranoid Schizophrenia (F20.0) as per ICD-10. 15
Routine biochemical tests showed normal results. The treatment was initiated with daily injections of Haloperidol 20 mg and Promethazine 50 mg, which were subsequently tapered. Olanzapine was introduced at a dose of 10 mg per day and progressively increased to 15 mg per day. The patient demonstrated a good response to treatment over two weeks, with a reduction in delusional and hallucinatory symptoms. Cognitive behavioral therapy (CBT) and insight facilitation sessions focused on self-harm behavior were initiated with the assistance of a clinical psychologist. The patient showed significant improvement and was subsequently discharged in a stable condition.
Case 3
A 65-year-old male presented to the emergency department with a self-inflicted amputation of the penis and multiple neck lacerations sustained two days prior (Figures 3 and 4). First aid and surgical consultations were provided. Examination revealed a complete transection of the penis at the penoscrotal junction, controlled bleeding with ligatures, and a 25 cm neck laceration. The amputated penis, with a six to seven-hour warm ischemia time, underwent unsuccessful replantation due to gangrenous changes.
Mutilated Penis of the Patient.

Lacerated Injury Marks on the Neck of the Patient.

Postoperative View of the Base of the Penis with a Catheter in Situ.

The patient had a 20-year history of psychiatric illness but had been non-compliant with medications for the past two years. His brother accompanied him during the psychiatric evaluation. The patient, a separated farmer from a low socio-economic background, exhibited irritability, suspiciousness, muttering, wandering, and disturbed sleep. He experienced auditory hallucinations of derogatory voices commanding him to harm himself and was suspicious of family and neighbors plotting against him. These symptoms worsened over the past two years, leading to isolation and refusal of food due to paranoia. One night, voices commanded him to mutilate his genitals to prevent spirits from entering his body, prompting the self-inflicted injury with a sickle knife.
Routine investigations were within normal range. Clinically, the patient appeared thin, poorly groomed, and wearing untidy clothes. He was cooperative but had difficulty establishing rapport, with reduced psychomotor activity and stereotyped hand movements. His speech was slow and sometimes irrelevant. He reported feeling upset, with an objectively irritable affect incongruent with his mood. He maintained delusions of persecution and heard derogatory, commanding voices causing distress, indicative of Paranoid Schizophrenia (F20.0), as per ICD-10. 15 During inpatient care, the patient was interviewed multiple times, and serial Mental Status Examinations (MSE) were conducted to understand the psychopathology underlying the self-mutilation. It was observed that the patient’s poor insight into self-mutilation was associated with delusions and command hallucinations.
The patient was managed in the plastic surgery ward and diagnosed with schizophrenia by the psychiatry team. Treatment began with Olanzapine, titrated to 20 mg per day over three weeks, and later switched to long-acting injectables due to poor compliance. Psychoeducation sessions were provided to the patient and family to address compliance issues. The patient was discharged after two weeks and scheduled for regular follow-up visits in the psychiatry OPD.
During follow-up, significant improvements in delusions, hallucinations, and self-care were noted. Despite ongoing reluctance to take medications, long-acting injectables were continued alongside oral medications. Six sessions of psychoeducation and insight facilitation were completed during the follow-up period. Over two months, periodic mental status evaluations indicated a substantial reduction in psychotic symptoms.
Discussion
Schizophrenia is a severe chronic mental disorder with a disabling nature and course, which imposes a significant burden on patients’ families, friends, and society. Schizophrenic patients are known to have self-harm behavior due to active psychotic symptoms such as hallucinations, delusions, catatonic excitement, and sometimes due to associated affective symptoms. 16 In these cases, the delusion of persecution and commanding hallucinations were the leading causes of self-harm behavior. Patients with schizophrenia have a higher magnitude of self-harm and suicidal behavior than the general population. During the acute phase of illness, the risk of self-harm behavior is significantly higher. Therefore, drug-naive psychotic patients carry the maximum chance of suicidal self-harm behavior. 17
It was seen that patients with the schizophrenia-related disorder had a younger mean age at the time of self-injurious behavior. It was also seen that patients with schizophrenia used more lethal methods to harm themselves than patients with mood disorders. 18 Patients of schizophrenia who suffer from persistent psychotic symptoms with poor insight and deteriorating socio-occupational functioning have a higher risk of suicide and self-harming behavior. 19 Self-harm and suicidal behavior were seen to be very common in young patients, especially with first-episode psychosis. 20 We also noticed that with treatment in a short span (two weeks), symptoms started improving, and most of the patients were off medications or presented for the first time.
Managing NSSI behavior and suicidal behavior in patients with schizophrenia requires a comprehensive approach addressing the underlying psychopathology and providing appropriate interventions. Manual-assisted cognitive therapy, dialectical behavior therapy, emotion regulation group therapy, second-generation antipsychotics such as aripiprazole, SSRI and CBT, and naltrexone are some interventions that seem to show promise for reducing NSSI. 21
Conclusion
NSSI behavior is common in schizophrenia, serving as a coping mechanism and expression of distress. This case series highlights NSSI’s significance, unique characteristics, and motivations in this population. Comprehensive assessment and intervention strategies are essential, considering psychiatric symptoms, emotional dysregulation, cognitive deficits, and comorbid conditions. Identifying factors like childhood trauma, negative symptoms, and poor insight underscores a holistic approach to managing NSSI. Linked to emotional distress, increased suicide risk, and severe health consequences, NSSI must be managed immediately. Distinguishing NSSI from suicidal behavior is crucial for effective clinical intervention.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. The manuscript, to the best of the author’s knowledge, does not infringe upon any copyright or property right of any third party.
Declaration Regarding the use of Generative AI
The article was ideated and drafted in a text editor and was refined with the aid of artificial intelligence tools like ChatGPT and Grammarly, and was revised to reflect our intended message.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
All patients included in this case series provided informed consent for the use of their medical information and images for publication purposes. Consent was obtained in accordance with ethical guidelines, ensuring patient confidentiality and privacy throughout the publication process.
Prior Presentation
No prior presentations done. The case series being submitted has not been published, simultaneously submitted, or already accepted for publication elsewhere.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.