
Abstract
Background:
Facial emotion recognition (FER) deficits are being considered as core features of social cognitive deficits in schizophrenia, associated with socio-occupational dysfunction. Social cognition intervention programs have been shown to improve these deficits; however, there are no such intervention strategies in India. In this study, we aim to examine the efficacy of Training of Affect Recognition – Indian Version (TAR-IV) to enhance the FER abilities of people with schizophrenia.
Methods:
In an open-label experimental design, 36 participants with schizophrenia underwent 12 sessions of TAR-IV as an add-on to treatment as usual (TAU), while 29 participants with schizophrenia continued TAU (pharmacological treatment with or without occupational therapy and vocational rehabilitation services). Clinical and functional assessments were done using the positive and negative syndrome scale (PANSS) and socio-occupational functioning scale. Emotion recognition abilities were assessed on the tool for recognition of emotions in neuropsychiatric disorders at baseline, post-intervention, and follow-up (two to three months post-intervention).
Results:
The intervention group showed significant improvements in FER (P = .001) and socio-occupational functioning (P = .008) after receiving the TAR-IV, which remained significant at two months follow-up. A lower age of onset and poorer neurocognitive function at baseline predicted greater changes in emotion recognition ability following the intervention.
Conclusions:
This study demonstrated the efficacy of TAR-IV, the Indian adaptation of social cognition intervention, in improving emotion recognition abilities and socio-occupational functioning in patients with schizophrenia. These findings need to be replicated in randomized controlled trials.
Keywords
TAR-IV was feasible for training affect recognition in schizophrenia patients in Indian setting. TAR-IV enhanced facial emotion recognition abilities in patients with schizophrenia.Key Messages:
Social cognition refers to the cognitive processes involved in identifying facial emotions, understanding the mental state of others, interpreting cues from socio-environmental situations, and producing an appropriate response. 1 This social cognitive ability is a highly evolved function, and Homo sapiens demonstrate a much higher ability in this domain as compared to other primate species. 2
Deficits in social cognitive abilities have been observed in individuals with schizophrenia as well as in those with autism. 3 In schizophrenia, these deficits have been described as trait deficits that persist throughout the disorder and are associated with socio-occupational dysfunction. Hence, understanding these deficits and the strategies to improve social cognition and socio-occupational functioning is of important clinical significance.1,4
The conventional treatment for schizophrenia includes pharmacological and non-pharmacological intervention programs (family intervention, vocational rehabilitation, social skills training, cognitive remediation), primarily focusing on treating positive symptoms and socio-occupational dysfunction.5,6 These non-pharmacological interventions have shown their effectiveness in preventing relapse and improving cognitive abilities and work-related performance of persons with schizophrenia.7,8 However, they may explain only 20%–40% of the variance in functional outcomes. 9 Studies where subjects underwent a cognitive remediation program achieved improvements in their basic cognitive abilities (learning and memory tasks) but failed to show improvements in social cognition tasks (emotion recognition). 10 A meta-analysis of 42 studies of social cognition intervention in schizophrenia showed moderate effects on improving social cognitive abilities and only a weak effect on improving executive functions. 11 Integrated cognitive remediation and social cognition may achieve synergistic effects in improving functional outcomes in persons with schizophrenia. 12 This highlights the need for valid social cognition intervention programs in the treatment of schizophrenia.
Social cognition intervention modules have been developed and evaluated in Western settings.13,14 Meta-analytical studies11,15 have reported various social cognition training programs (such as Social Cognition Interaction Training [SCIT], Training of Affect Recognition [TAR], Social Cognition Enhancement Training [SCET], Attentional Shaping, Social Cognition Training Program [SCTP], Emotion Management Therapy [EMT], Social Cognition Skill Training [SCST], Emotion and TOM Imitation Training [ETIT], Micro Expression Training Tool [METT]) and reported moderate effect sizes in improving social cognitive abilities.11,15,16,17 These interventions utilize social contexts and situations that may not be applicable to the Indian cultural setting and, hence, may need adaptation. The TAR is a standardized social cognition intervention program. The authors have previously reported the adaptation of this program to the Indian cultural setting (TAR-IV) and the feasibility of administering this intervention program in our patient population. 18
The current study sought to examine the efficacy of the adapted TAR-IV program in improving emotion recognition abilities in Indian persons with schizophrenia in comparison to treatment as usual (TAU). We also examined the effects of the training program on social functioning. We hypothesized that the TAR-IV program would improve facial emotion recognition (FER) and socio-occupational functioning in persons with schizophrenia compared to TAU.
Methods
Participants
Individuals with a clinical diagnosis of schizophrenia according to the ICD-10 criteria were recruited from the outpatient and inpatient services and extension clinics of the Department of Psychiatry, Kasturba Medical College, Manipal, Dr A. V. Baliga Memorial Hospital, Udupi, and Kiran Rehabilitation Centre, Mangalore, three centers in coastal areas of south India.
The inclusion criteria were: (a) age range from 18 to 55 years; (b) education at least up to the seventh standard and ability to read the local language, Kannada, which is the native language spoken in the geographical region where the study was conducted; (c) score equal to or below 70 on the Positive and Negative Syndrome Scale (PANSS) 19 ; (d) score three or less on the Clinical Global Impression Severity (CGI-S) 20 ; (e) score greater than 24 on the Hindi Mental Status Examination (HMSE) 21 ; and (f) stable dose of antipsychotic medication for the last four weeks The exclusion criteria were as follows: (a) comorbid neurological disorders such as seizure disorder, stroke, head injury, or intellectual disabilities; (b) comorbid psychiatric disorders; and (c) substance dependence other than nicotine in the last six weeks. In order to have a homogeneous group of persons with schizophrenia in the present study, we excluded patients with comorbid psychiatric disorders and substance dependence other than nicotine in the last six weeks. Nicotine dependence was not an exclusion as it is widely prevalent in persons with schizophrenia. 22
Sample Size Estimation
At 80% power of the study, the probability of alpha error at 0.01 with an effect size of 0.8 (as reported in earlier studies using the TAR), the sample size was estimated to be 60 (30 each in the study and comparison group). Accounting for attrition (estimated at 25% as reported in earlier studies),10,23 we aimed to recruit 80 subjects (40 each in the study and comparison group).
Procedure
The study was approved by the institutional ethics committee of Kasturba Medical College and Kasturba Hospital (Approval No. IEC 211/2013 dated 14-05-2013) and registered in the Clinical Trials Registry – India CTRI (CTRI/2017/04/ 008351). The Institutional Human Ethics Committee approved the protocol, and all study participants provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki. The experimental design of the study was a non-randomized open-label trial, with persons with schizophrenia receiving either training in the TAR-Indian version or TAU. The study was conducted between 2015 and 2017. Individuals with schizophrenia were approached for participation in the study and explained about the TAR program. Participants who were willing to attend training sessions regularly were recruited to the intervention group, and those who were unwilling to participate in the TAR program or, due to logistic reasons, expressed an inability to travel to the hospital for regular sessions were recruited into the comparison group and advised to continue TAU. Participants in both groups received a stable dose of antipsychotic medication throughout the study period. Both groups continued to receive other psychosocial interventions, as determined by the treating psychiatrist. The participants in the intervention group underwent a 12-session TAR program. Assessments were performed in the intervention group at baseline (T0), post-intervention (T1) (4–6 weeks after completion of the TAR program), and follow-up (T2) two to three months after the T1 assessment. In the TAU group, assessments were similarly performed at baseline (T0), after 4–6 weeks (T1), and after 2–3 months (T2).
Intervention-emotion Recognition Training on the TAR-Indian Version
The details of adaptation and feasibility of using TAR-IV have been described earlier. 18 Briefly, the cultural adaptations included (a) translation of all instructions, emotional words, and worksheets to the vernacular language Kannada, (b) adaptation of social contexts and situations to the Indian cultural and regional context, (c) Modifications of methods in the administration of the session tasks to accommodate unfamiliarity with computer use in our population (supplementary Table 1). We refer the reader to our earlier publication for the detailed description of the cultural adaptation made in the TAR-IV. 18 It comprises 12 training sessions of 45 minutes to one-hour duration administered twice a week. Participants completed the training either in pairs when two consenting participants were available to undertake the training during one training period or individually when only one consenting participant was available. TAR is based on the principles of errorless learning, feature abstraction, self-instruction, and positive reinforcement. It has three blocks. During the first one to four sessions’ facial expressions of the six basic emotions (happiness, sadness, fear, anger, surprise, disgust) and neutral are learned with the appropriate prototypical facial components. The second aim is to learn appropriate alternative verbal strategies to avoid impaired automatic processing. In the second block, the fifth and sixth session focuses on increasing judgment confidence while recognizing facial emotions. In the seventh and eighth sessions, the participants are taught to recognize less intense emotional expressions correctly. With matching tasks in the eighth session, nonverbal processing is trained, and in doing so, a more holistic recognition and increased automatic processing is facilitated. In the third block, the ninth and tenth sessions’ situative-cognitive anchors or cues are practiced. By using ambivalent facial expressions, participants were taught to use situational cues in these situations. The 11th and 12th sessions teach expressive behavior in social interactions. Patients are taught that the inspection or survey of unity of a situation, cognition, and emotion as a strategy of verification or falsification plays a central role in interpreting social scenes (supplementary Table 2).
Adherence to the training program was ensured because all 12 sessions of the TAR_IV were conducted under therapist supervision. The therapist also supervised and evaluated the homework tasks.
Assessment of Socio-demographic and Psychiatric Symptoms
Participants’ socio-demographic information (patient’s age, gender, educational background, occupation) and clinical variables (diagnosis, course of illness, current medications) were collected using semi-structured interviews. Patients’ psychopathology was assessed using the PANSS 19 HMSE 21 to rule out significant cognitive deficits in the study participants. HMSE is based on MMSE (Mini Mental Status Examination). It has 23 items to assess orientation, memory, identification, and understanding of simple commands. It has a total score of 31, and a cut-off score of 24 was considered on HMSE to identify cases of cognitive impairment. As HMSE is an objective assessment tool, in the present study, the first author administered the HMSE in the Kannada language to rule out cognitive impairment in the study participants. Neurocognitive tests included the Verbal N-Back Test for Working Memory (VNBT). 24
Primary Outcome Measures
Assessment of Emotion Recognition Ability
Tools for Recognition of Emotions in Neuropsychiatric Disorders (TRENDS) 25 TRENDS is a culturally sensitive, ecologically valid tool developed for the assessment of FER abilities in Indian subjects. This tool consists of two sets of facial emotion images: static (still photographs) and dynamic (video). The stimuli consist of six basic emotions—happy, sad, fear, anger, surprise, and disgust–expressed at high and low intensity along with a neutral facial expression by four trained actors (one older female and one young male, one young female, and one older male) [four posers × (six low-intensity emotions stimuli + six high-intensity emotions stimuli + neutral = 52 static images and four posers× (6 emotions+ neutral) = 28 dynamic images]. The static and dynamic images were randomized and arranged in stimulus presentation software. Images were presented in the same order to all subjects. Subjects are presented with possible emotion choices and are instructed to choose the best response for the image (details mentioned earlier in the description of TRENDS). 25 Three types of scores were calculated for the performance on TRENDS: (a) the total number of correctly identified stimuli was then computed and termed the TRENDS Accuracy Score (TRACS). (b) The total number of images of non-threatening emotions (sadness, happiness, neutral) identified as any of the threatening emotions (fear, anger, and disgust) is termed the TRENDS over-identification score. (c) Similarly, the total number of images of threatening emotions (fear, anger, and disgust) identified as any of the non-threatening emotions (sadness, happiness, and neutral) is termed as the TRENDS under-identification score. 25
Secondary Outcome Measures
Social occupational functioning was assessed using the Social Occupational Functioning Scale (SOFS). 26 This scale has 14 items and assesses functioning in the domains of Adaptive Living Skills, Social Appropriateness, and Interpersonal skills. Each item is rated on a 5-point Likert scale (1 = no impairment to 5 = extreme impairment). The higher the score, the more the impairment.
Statistical Analysis
Data obtained were analyzed using SPSS version 16.0 for Windows. Study variables were examined for normality using the Shapiro-Wilk test. Among the demographic and clinical variables, age, education, age of onset, duration of illness, PANSS, SOFS, and TRENDS scores were normally distributed, but the verbal N-back test and antipsychotic equivalent scores were not normally distributed. We compared the above variables at baseline between the treatment and comparison group using an independent t-test for normally distributed and continuous variables, the Mann-Whitney test for those not normally distributed, or the chi-square test for categorical variables. Changes in emotion recognition scores between T0 and T1 and T0 and T2 in each group were compared using the paired t-test. Repeated Measures of analysis of variance were used to examine the time × intervention effect. We reported significant results at p < 0.05. The effect size was reported as partial eta square ηp 2 (η 2 = 0.01 indicates a small effect; η 2 = 0.06 indicates a medium effect; η 2 = 0.14 indicates a large effect). 27 We additionally adjusted the analysis for the baseline PANSS scores. To account for attrition, all participants who completed the training program were included in the analysis. If the participant did not complete assessments at T2, we used the Last Observation Carried Forward (LOCF) method. Pearson’s correlation analysis was performed to examine the association between SOFS scores and emotion recognition accuracy. To understand the moderators of emotion recognition training response, we ran separate regression models with pre-post differences in TRENDS score as the dependent variable and baseline scores of working memory test scores, SOFS scores, PANSS score, and participants’ age and age of onset as predictors.
Results
A total of 88 patients with schizophrenia were recruited for the current study (n = 45 in the intervention group; n = 43 in the comparison group). Of these, 65 participants completed the post-assessment at T1 (n = 36 in the intervention group; n = 29 in the comparison group; 14 did not compete for training, one had a relapse, and eight did not come for post-assessment) (Figure 1). Of the 36 participants who completed the training, 14 did the training in pairs, and eight did it individually. Forty-six participants (n = 23 in the intervention group and n = 23 in the comparison group) completed the follow-up assessment at T2. The baseline clinical and demographic characteristics of the participants who dropped out were not significantly different from those of the final study participants. No serious adverse events were observed during the study.
Flow Chart of the Study Participants.
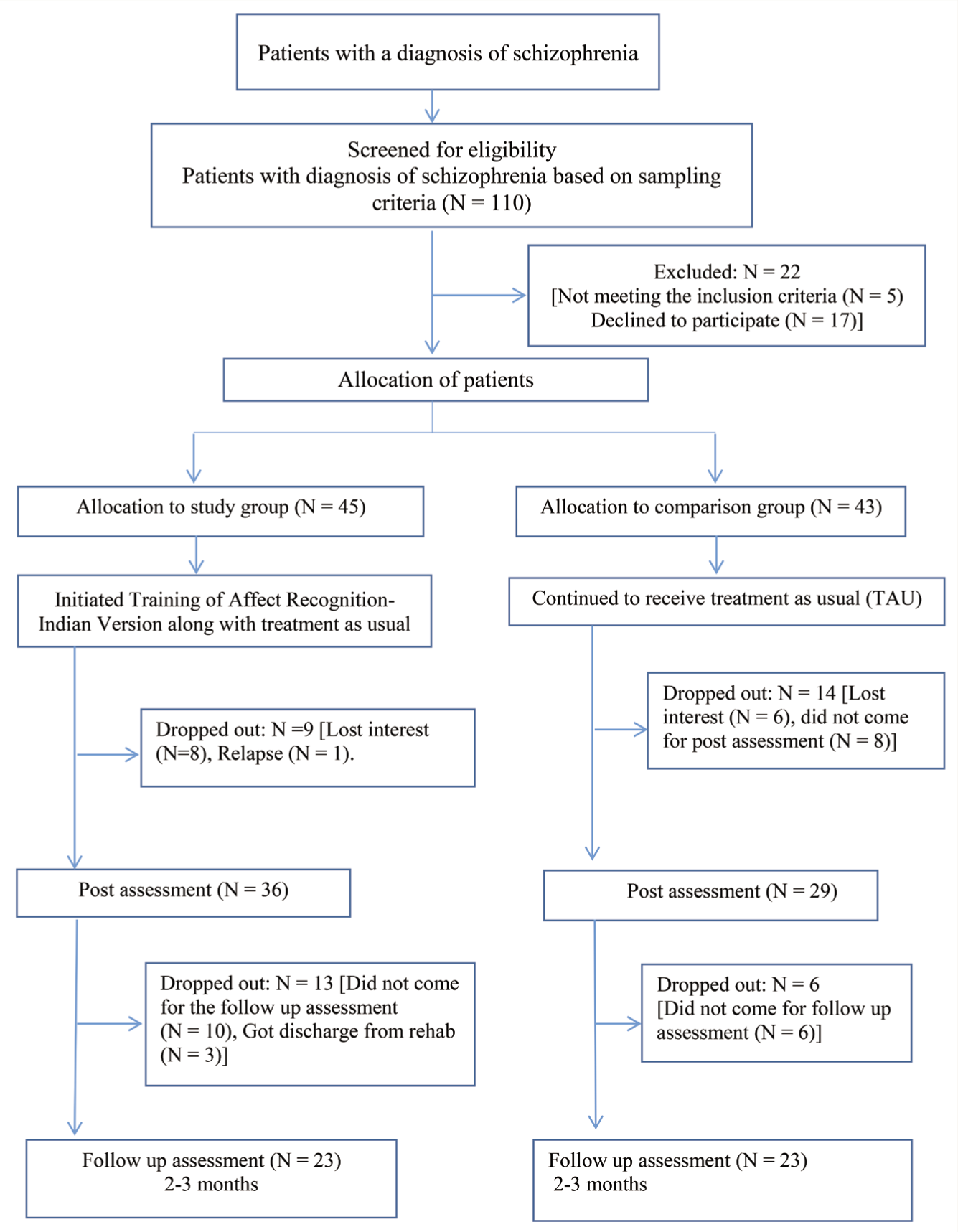
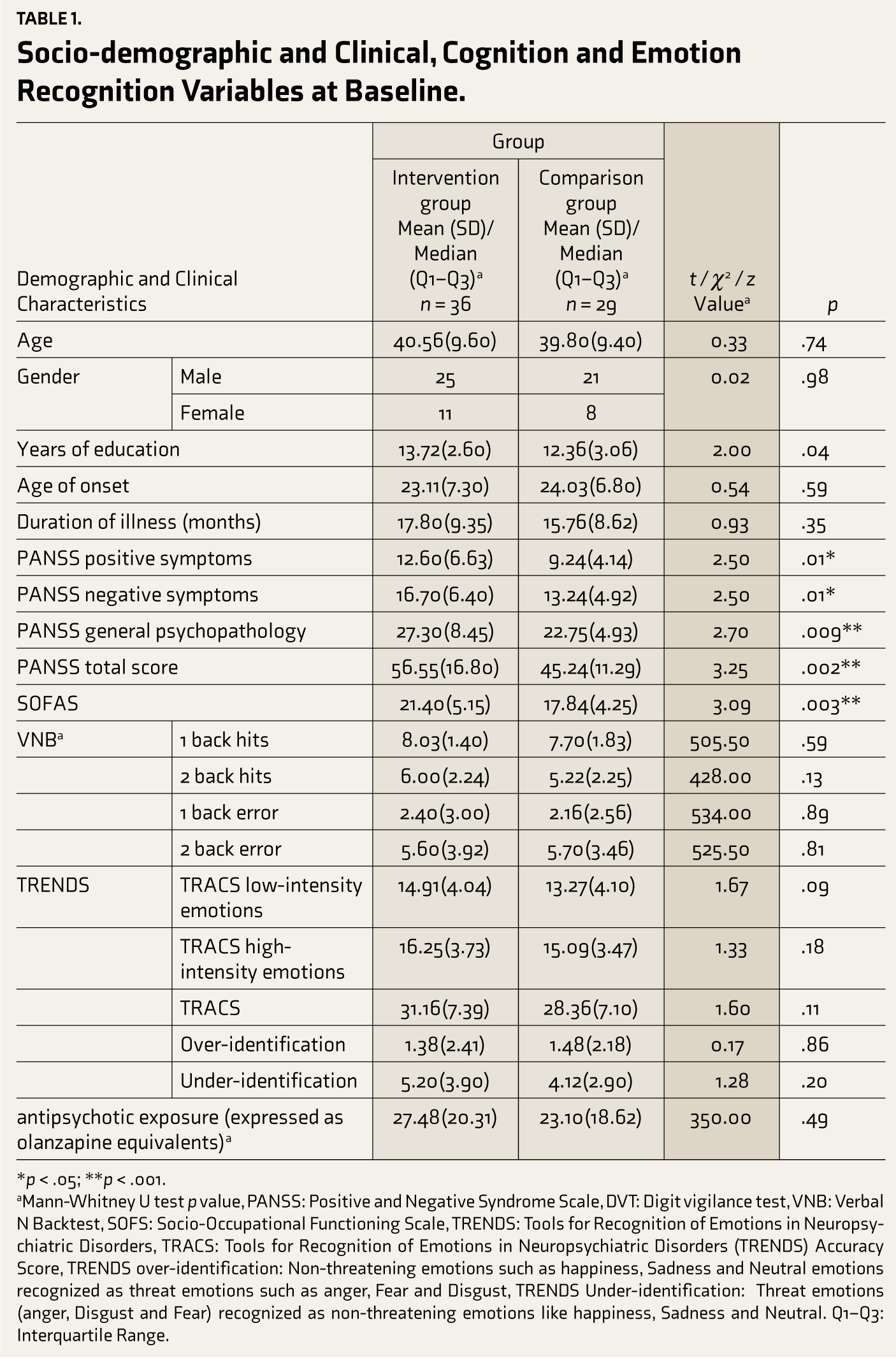
Table 1 shows the demographic and clinical characteristics. There was no difference between the two groups in terms of age, sex, course of illness, duration of untreated psychosis, duration of illness, age of onset, and antipsychotic exposure. At T0, there was no difference between the two groups in performance on the verbal N-back test, TRENDS accuracy score, and over- and under-identification. The intervention group had higher education and baseline PANSS and SOFS scores (Table 1).
Socio-demographic and Clinical, Cognition and Emotion Recognition Variables at Baseline.
*p < .05; **p < .001.
aMann-Whitney U test p value, PANSS: Positive and Negative Syndrome Scale, DVT: Digit vigilance test, VNB: Verbal N Backtest, SOFS: Socio-Occupational Functioning Scale, TRENDS: Tools for Recognition of Emotions in Neuropsychiatric Disorders, TRACS: Tools for Recognition of Emotions in Neuropsychiatric Disorders (TRENDS) Accuracy Score, TRENDS over-identification: Non-threatening emotions such as happiness, Sadness and Neutral emotions recognized as threat emotions such as anger, Fear and Disgust, TRENDS Under-identification: Threat emotions (anger, Disgust and Fear) recognized as non-threatening emotions like happiness, Sadness and Neutral. Q1–Q3: Interquartile Range.
Primary Outcome
Effect of the TAR-IV on Emotion Recognition
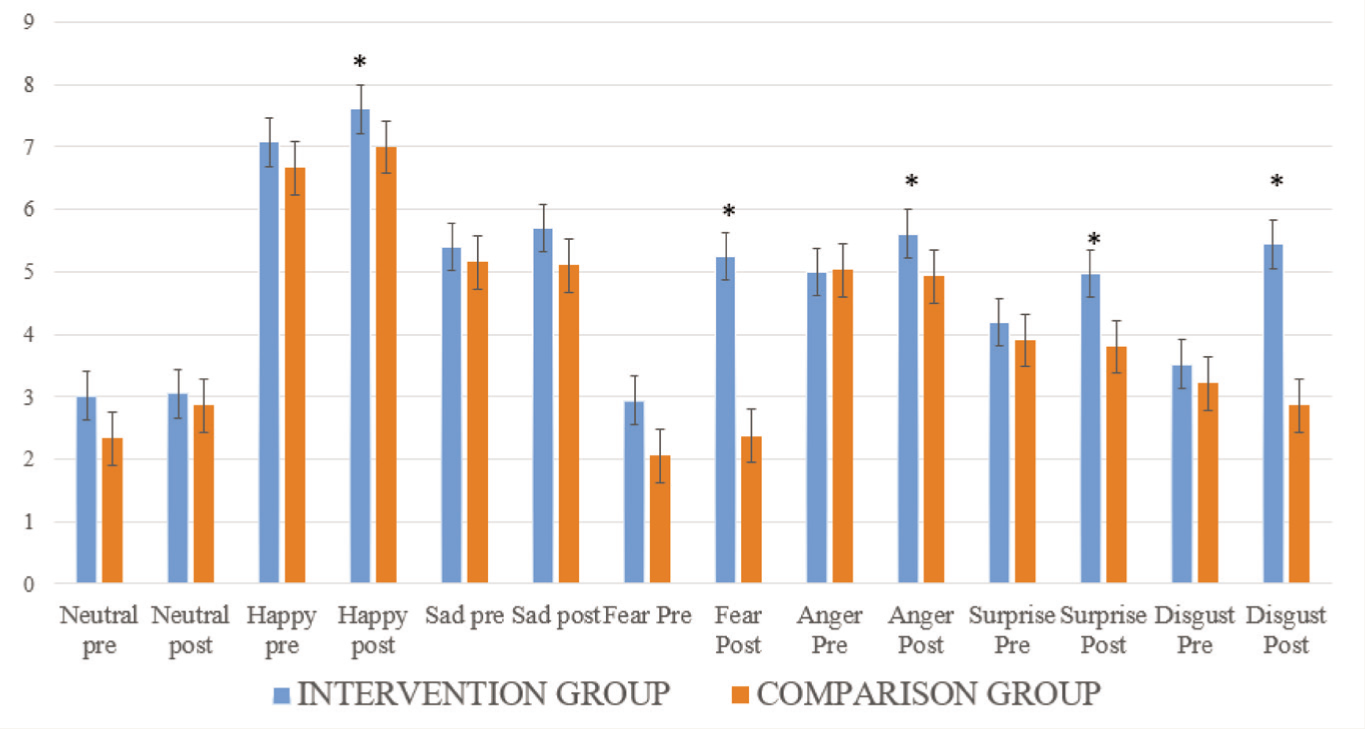
The study participants in the intervention group showed significantly better performance on the emotion recognition task at T1 in terms of total accuracy (t = 10.04, p = .001). This was significant for both low (t = 6.57, p = .001) and high-intensity emotions (t = 8.30, p = .001). Upon examining performance on individual emotions, identification of disgust and fear, anger, surprise, and happy emotions was significantly higher in the intervention group (Figure 2, p = .001). The participants who received the intervention also showed a lower under-identification score (Z = 4.10, p = .001). All improvements observed in the intervention were statistically significant, even at T2. There was no improvement in over-identification. The change in emotion recognition scores between any time points was not significant in the TAU group.
Effect of TAR-Indian version on Individual Emotions (Group Comparison on Recognizing Individual Facial Emotions).
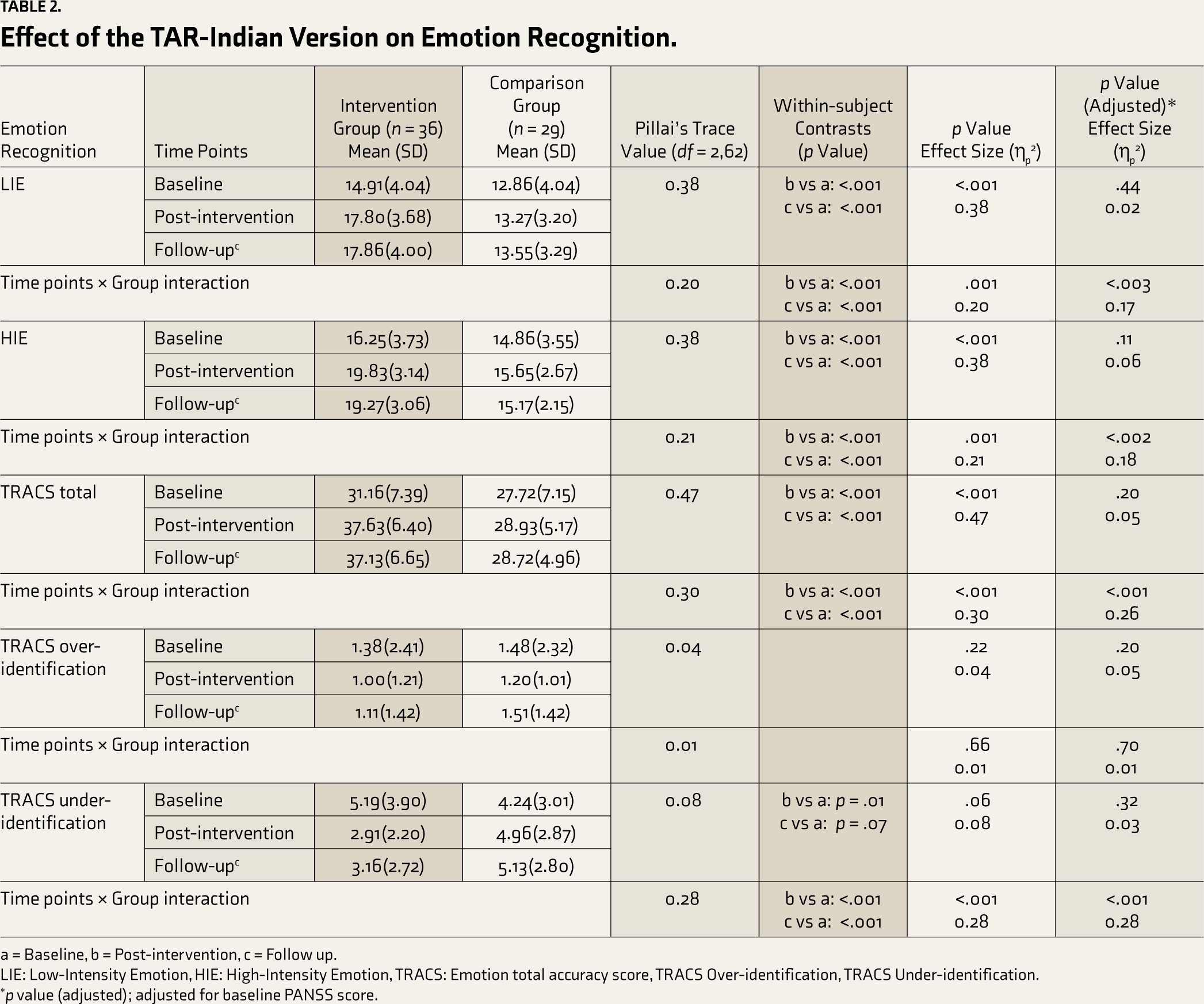
A repeated measures analysis of covariance showed a significant main effect of the TAR-IV on improvement in FER in the intervention group with a large effect size in improving emotion recognition ability in the intervention group (TRACS total: Pillai’s trace F(2,61) = 27.73, p = .001, ηp 2 = 0.47; 95% CI: 3.82–9.88) (Table 2, Figure 3). After adjusting for baseline psychopathology, the differences continued to be significant with some reduction in effect size (p = .001, ηp 2 = 0.26; 95% CI: 3.82–10.30).
Effect of the TAR-Indian Version on Emotion Recognition.
a = Baseline, b = Post-intervention, c = Follow up.
LIE: Low-Intensity Emotion, HIE: High-Intensity Emotion, TRACS: Emotion total accuracy score, TRACS Over-identification, TRACS Under-identification.
*p value (adjusted); adjusted for baseline PANSS score.
Emotion Recognition Accuracy at Three-time Points (Baseline, Post-intervention, and Follow-up).
Secondary Outcome
Effect of the TAR-IV on Social Functioning in Individuals with Schizophrenia
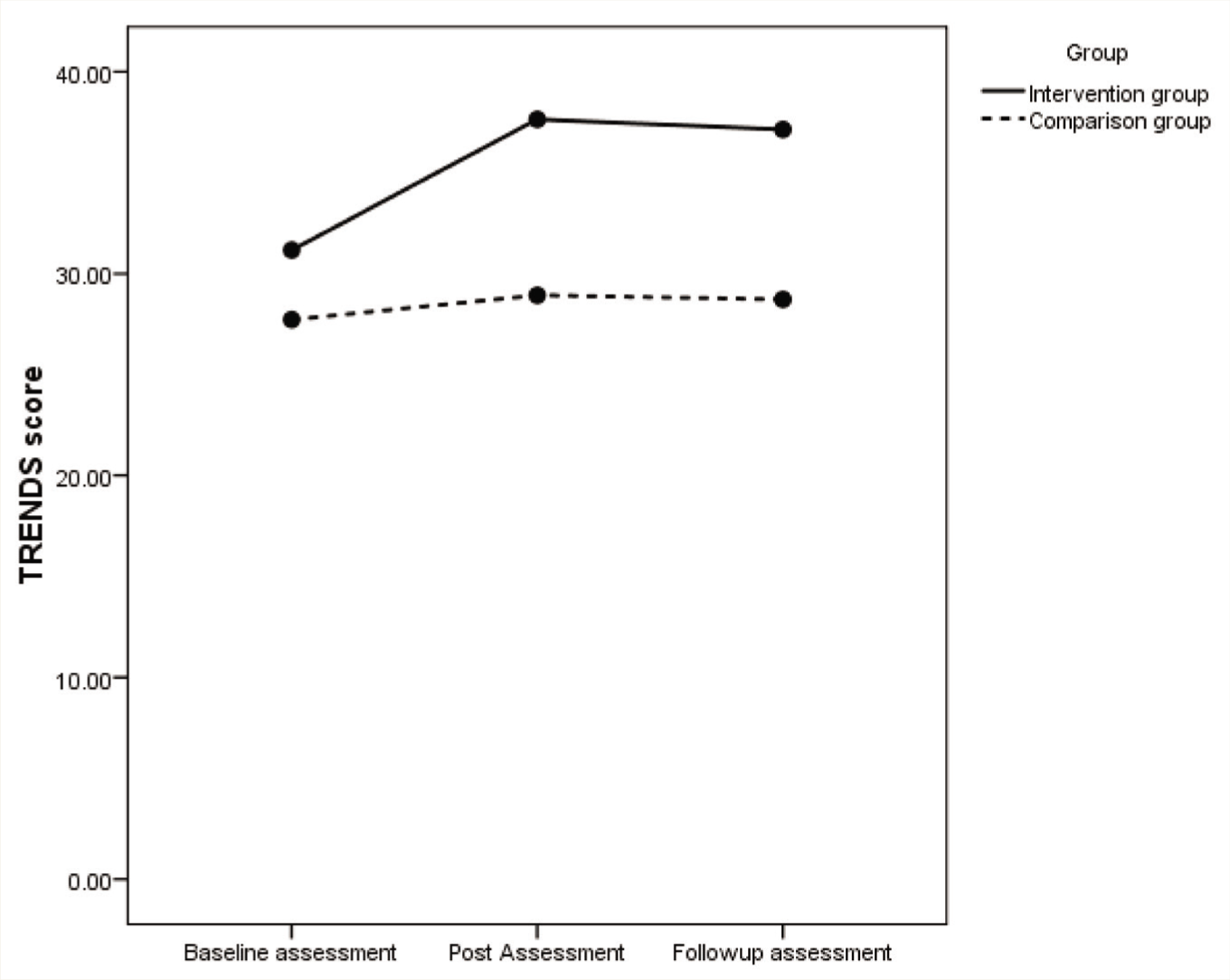
The intervention group showed a significantly higher improvement in the total SOFS score than the TAU group (Pillai’s trace F (2,62) = 0.29, p = .001, ηp 2 = 0.29; 95% CI: 0.19–4.34). The time × group interaction was significant (p = 0.008) for the total SOFS score. Post-hoc comparisons showed that the effect of the intervention remained significant at T2 from T0 (p = .003). After adjusting for baseline psychopathology (PANSS), the differences in SOFS scores between the intervention and comparison groups were no longer significant [(Pillai’s trace F(2,62) = 0.06, p = .13, ηp 2 = 0.06; 95% CI: –1.27 to 2.35] (Table 3). There was no significant correlation between the changes in TRACS scores and changes in total SOFS scores (from T0 to T1) in the intervention group (r = 0.05, p = .73).
Effect of TAR-Indian version on Socio-occupational Functioning Scale Score.
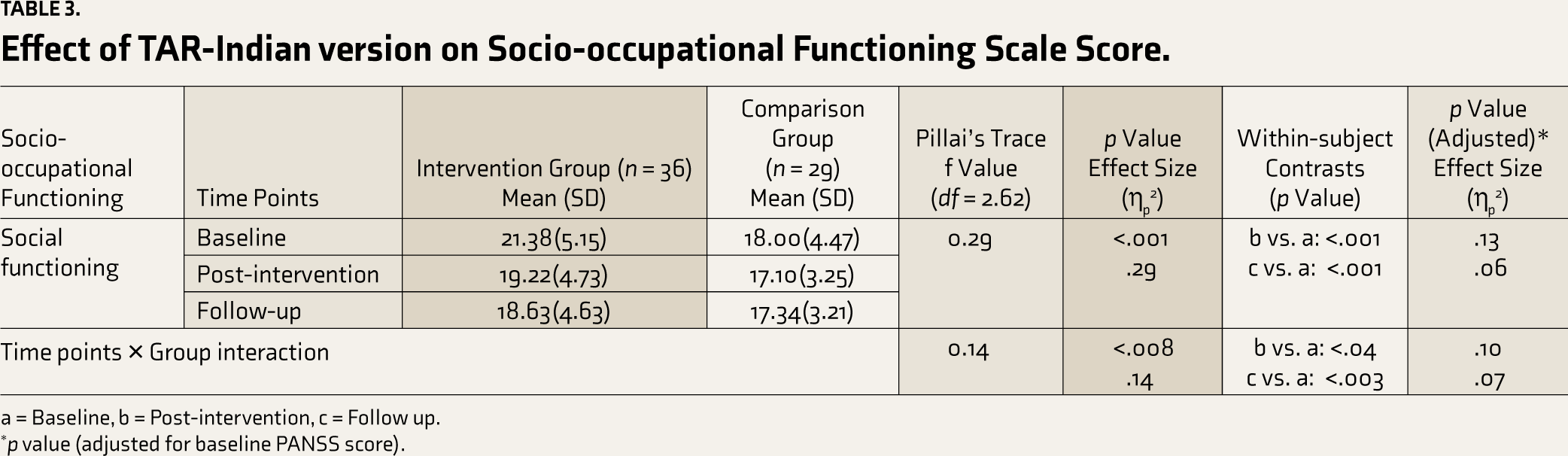
a = Baseline, b = Post-intervention, c = Follow up.
*p value (adjusted for baseline PANSS score).
Predictors of Change in Emotion Recognition
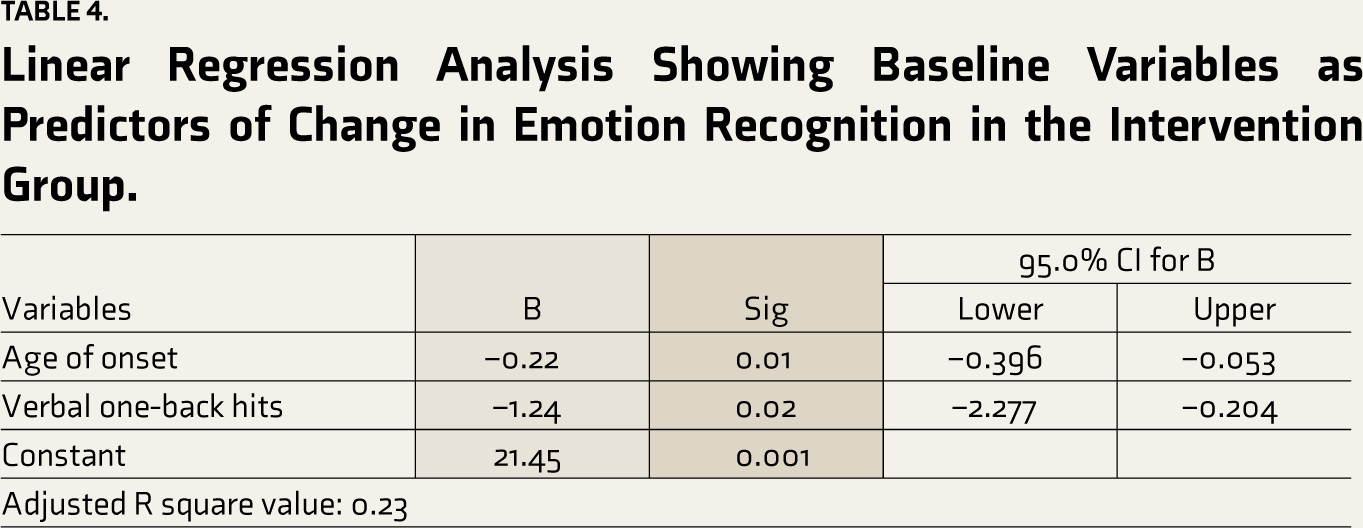
A regression analysis with the change in TRACS score and patient age, age of onset, baseline digit vigilance test total time and error score, baseline verbal N-back test (one-back hits and error, two back hits and error) score, baseline SOFS score, positive symptoms, negative symptoms, and general psychopathology revealed age of onset (β = –0.22, p = .01; 95% CI –0.39 to –0.05) and verbal one-back hits (β = –1.24, p = .02; 95% CI -2.27 to –0.20) as significant predictors, with 21.45% explained variance (Table 4).
Linear Regression Analysis Showing Baseline Variables as Predictors of Change in Emotion Recognition in the Intervention Group.
Discussion
To the best of our knowledge, this is the first Indian study to examine the efficacy of a social cognition intervention program in Indian people with schizophrenia using a culturally adapted training program. We found that the TAR-IV, in comparison with the TAU group, improved emotion recognition abilities in general and specifically for fear, disgust, anger, surprise, and happy facial emotions. The effect of the intervention was sustained after two months of follow-up. We also observed improvement in socio-occupational functioning in the intervention group. However, this improvement was influenced by baseline psychopathology. This suggests that improvement in social cognition may reflect only small changes in socio-occupational functioning, as functioning may depend on multiple factors. These observations are in line with several other studies on TAR, which have demonstrated significant improvement in FER in persons with schizophrenia.4,10,17,28
The findings of our study add to the increasing evidence, which suggests that specific social cognition intervention programs can improve social cognition abilities in schizophrenia. A recent meta-analysis reported that brief but intensive and targeted single-domain social cognition intervention programs have an advantage in improving lower-order social cognition abilities like FER compared to broad-based intervention programs.11,29 A study comparing TAR with a broad-based intervention program, the SCIT, showed that the TAR was more efficacious than SCIT in improving FER. At the same time, the theories of mind were similar in both. This suggests that FER training programs can improve multiple domains of social cognition. However, this study did not assess the effect of TAR on other social cognition domains. 30 In our study, we observed large effect sizes for improvement in emotion recognition abilities, which were maintained at two to three months follow-up. In addition, our findings show the cross-cultural effectiveness of TAR in improving emotion recognition abilities in schizophrenia.11,17,29-31 It also demonstrates the utility of TRENDS as a reliable tool to measure changes in emotion recognition abilities with social cognition intervention. 18 Earlier cross-cultural studies showed a culture-specific effect of the ethnicity of facial stimuli on emotion identification. 32 Our observations support the universality of emotion recognition.
An important observation in our study was the specific improvement in recognizing fear and disgust with the intervention. Deficits in recognition of these “threat” related emotions play a vital role in attributing emotional salience to environmental cues and may contribute to psychopathology and poorer socio-occupational functioning.33,34 Improvement in processing threat-related emotions may contribute to better socio-occupational functioning.
In the present study, the change in emotion recognition score was not influenced by the age or gender of participants, indicating the benefits of intervention across the lifespan. 35 However, Lower age of onset and poorer working memory were observed to predict greater changes in emotion recognition abilities with the intervention. Such patients might benefit from TAR and may be the targeted population for intervention. However, the literature on this is mixed, and some other studies suggest that response to intervention may not be dependent on baseline variables of age at onset, education, duration of illness, and neurocognitive impairment.10,11,36-40 We observed that improvement in socio-occupational functioning after training on TAR was influenced by baseline psychopathology. Future trials on social cognition interventions are needed to address this issue systematically.
This study is the first to describe an intervention for social cognition in the Indian setting. The sample size in the intervention and comparison group was larger than that in previous studies.4,10,17,23,28,41 We recruited persons with stable schizophrenia, which reflects a real-world scenario, as these patients would benefit from psychosocial rehabilitation. We also demonstrated the stability of the improvements over a follow-up duration of two to three months.
We acknowledge that the study adopted an open-label and not randomized study design, which may have resulted in selection bias. The subjects at baseline in the intervention group had higher psychopathology, but the confounding effect of this was controlled for in the statistical analyses. At baseline, the intervention group had lower socio-occupational functioning. This may have been responsible for the larger magnitude of change in this group. In addition, it was not possible to control for the effects of the additional intervention that some participants may have been receiving by virtue of being in a residential care center. Our outcome assessments focused on emotion recognition abilities, and we did not assess changes in other social cognition domains. However, taking into consideration the stability of FER performance between post-intervention measures and follow-up in both groups, it seems unlikely that such non-specific effects are responsible for the enhancement of emotion recognition accuracy in the intervention group. Such non-specific effects would also be active during the follow-up time window.
Finally, the generalizability of the current study findings needs to be examined in a study involving patients from different regional and cultural backgrounds in India. The majority of the participants in the present study were educated and borderline mentally ill to mildly ill. Hence, further studies are required to strengthen the applicability of this intervention program in the Indian context.
In conclusion, this study demonstrated the efficacy of TAR-IV, the Indian adaptation of social cognition intervention, in improving emotion recognition abilities and socio-occupational functioning in patients with schizophrenia. These findings need to be replicated in randomized controlled trials.
Supplemental Material
Supplementary material for this article is available online.
Footnotes
CTRI Registration
CTRI/2017/04/008351
Data Sharing Statement
Deidentified individual participant data will not be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
AI was not used in manuscript preparation.
Ethics Approval
Kasturba Medical College and Kasturba Hospital ethics committee (IEC 211/2013 Dated: 14-05-2013).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Indian Council of Social Science Research (ICSSR), Ministry of Human Resource Development, New Delhi: RFD/2014-15/GEN/PSY/317. PI: Dr. Umesh Thonse.
Informed Consent
All study participants provided written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.