
Abstract
Multiple sclerosis (MS) is a chronic neurological disorder with an autoimmune etiology that more commonly affects women between the ages of 20 and 40 years. Across the globe, the prevalence of MS is reported to be 2.8 million. 1 It has long been established that living with MS can have an impact on the physical, psychological, and social aspects. 2 The prevalence of neuropsychiatric problems in people with MS is estimated to be 95%. 3 Delays in accessing accurate treatment and poor treatment adherence might aggravate symptoms and increase disability. The majority of treatment components at present focus on symptom reduction and clinical management. 4
Self-management is an effective intervention for chronic health conditions, 5 defined as an individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences, and lifestyle changes inherent in living with the condition. 6 Various studies have shown the role of illness education and self-management in reducing symptoms in MS, 7 improving quality of life and reducing anxiety and depressive symptoms.4,8 Self-management interventions also enhance psychological well-being, especially self-esteem, 9 increase problem-oriented coping 10 and social participation, and change the health-related locus of control, optimism, and self-efficacy. 11 Assessment tools have been developed to recognize the increasing relevance of self-management interventions in MS. 12 People with MS who participated in self-management programs felt that they had been able to cope better with the illness. 13 While several models of self-management are discussed in the literature, the components such as knowledge about the illness, self-monitoring, problem-solving, and skill acquisition have been particularly well documented. 7 Context and personal factors can influence successful self-management. 14 Limited studies have explored the dimensions of self-management in MS, particularly in the Indian context.
We report five cases to capture factors influencing self-management outcomes in MS. The case series illustrates self-management interventions from a psychosocial perspective, following the self-management strategies discussed by Embrey. 13 The aim is to highlight the factors that would guide therapists in deciding on the intervention plan. CARE guidelines are followed in preparing the manuscript. 15
The cases were drawn from patients receiving in-patient care at a tertiary care setting from December 2022 to February 2023 and are part of a larger study on the lived experience of MS. The study received ethical clearance from the Institute Review Board. Consenting patients were invited to participate if their functionality score in EDSS was between 0 and 5 and they were between 18 and 40 years old. The patients were on disease-modifying therapies (oral or injectables based on affordability and disease severity). As part of routine multi-disciplinary care, the cases were referred by a consultant neurologist to address psychosocial concerns. Persons diagnosed with severe neuropsychiatric symptoms, neurodevelopmental disorders, severe cognitive impairment, significant behavioral changes, and problems in communication were excluded.
A detailed psychosocial assessment was conducted in each case to understand the socio-demographic background, family dynamics, and clinical profile, including neuropsychiatric manifestations. Open-ended questions as part of the assessment elicited specific concerns and needs of the participants on factors affecting the health-related quality of life. Informed consent was taken during the initial contact with the participant and family by explaining the purpose of the study.
The interventions were delivered by a trained mental health professional [psychiatric social worker (PSW) of the team]. The sessions occurred during in-patient care and were conducted daily, each spanning at least 30 minutes. On average, five individual face-to-face sessions were held, followed by one joint session with the caregiver. The initial session focused on building rapport and establishing a therapeutic alliance through the intake process and helped identify areas requiring focus in the intervention. The patient’s level of motivation was identified as an important determinant. The session focused on the significant psychosocial issues mutually identified as interfering with the patient’s functioning. Telephonic follow-up was carried out post-discharge.
Detailed case notes were kept to capture the history, assessment, concerns, and therapeutic interventions. The case reports were further subjected to thematic analysis using the framework method. 16 A framework was developed to identify the major factors that could influence the outcome of self-management interventions. The framework and thematic analysis were developed in the five steps described by Ritchie and Spencer: 17 ‑ data familiarization, identification of a thematic framework, indexing, charting to summarize the indexed data, and finding the patterns.
Case Series
Case 1
Ms. G, a 27-year-old woman and engineering graduate working as a software firm employee, is single and hails from Andhra Pradesh, approximately 500 km from the treatment center. Ms. G had her first episode of neurological illness in the year 2019, with complaints of intermittent numbness in the anterior part of her thigh and leg lasting for 15 minutes; one week later, it became continuous. She also developed altered sensation and later developed numbness in the right lower limb and pain along with numbness in the right half of the abdomen. A diagnosis of remitting relapsing MS was made and was managed with disease-modifying therapy. The patient responded well to the treatment and was symptomatically doing better. The psychosocial assessment found that the patient and family had adequate knowledge about MS and its management. It was reported that, premorbidly, she had anxious traits.
The patient’s mother was the primary caregiver in the hospital, and she had concerns related to her marriage as well as about the recovery. Uncertainty about the future was a major concern. Ms. G had an insight into the illness and the need for long-term management, such as regular medication and follow-up. Based on the assessment, the intervention was individualized. She was provided with education and was motivated to follow lifestyle modifications in the form of regular exercise and a healthy diet as part of the intervention. On subsequent follow-up, she said she is independent and doing well in everyday activities. Psychologically, the patient was well adjusted, and there were no neuropsychiatric issues. She regularly follows up and is in contact with the treatment team. She also follows a schedule to manage her activities, which includes lifestyle modifications.
Case 2
Ms. R is a 34-year-old female who is married, studied up to high school, is currently self-employed, and hails from Andhra Pradesh. She presented with complaints of headache and blurring of vision. She had undergone treatment in the local hospital in 2017 when the first episode occurred, and symptoms subsided at that time. She was regularly on medication suggested at that time and maintaining well. Subsequently, she developed pain in the upper left limb and presented to the tertiary care hospital outpatient department. On examination, a diagnosis of remitting relapsing MS was made and was managed with disease-modifying therapy. The patient responded well to the treatment and was symptomatically doing better. Ms. R was premorbidly well adjusted, and there was no significant personal history. Neuro-psychiatry assessment is a routine referral service for treating persons with MS. In the psychosocial assessment, it was found that the patient and family had limited knowledge about the illness and the need for regular medication. Apart from this, there were no active psychosocial challenges, and she had good social support in emotional and psychological aspects. She was able to manage the psychological distress, was adequately coping with the illness, and was able to maintain normal biological functioning. The interventions in this case were individualized and focused on education on the illness, fatigue management, and lifestyle modifications. The couple was encouraged to develop strategies to keep MS in its “required space” and not to let the illness take up more space in their family life. Fatigue management was identified as a need, and the factors that led to fatigue were assessed. A structured daily routine was developed and implemented, incorporating regular breaks and prioritizing activities based on energy levels. 18 Ms. R is on regular follow-up. No new neurological problems have been reported. She is maintaining well and is able to manage the disease well. During follow-up, the patient adhered to a regular activity program that included all the suggestions made during the self-management sessions.
Case 3
Ms. S, 22 years old, female, single, engineering graduate, currently not working, hails from Tamil Nadu, approximately 350 km from the hospital. She presented with complaints of weakness in the lower limb and difficulty in walking. She had the first episode in 2021 and was treated elsewhere for the same. Symptoms at that stage subsided with treatment. She further came to the outpatient department with complaints of having difficulty in walking with an imbalance while walking, worsening in the dark, and worsening of urinary urgency and frequency. A diagnosis of remitting relapsing MS was made and was managed with disease-modifying therapy. The patient responded well to the treatment and was symptomatically doing better. Assessment showed that the patient and family have partial knowledge about the illness and the need for regular medication. Ms. S was premorbidly well adjusted, and there was no significant personal history. At the time of assessment, the concerns were predominantly about the recurrence of the neurological problems and the future. There was no diagnosis of neuropsychiatric issues. Given this background, the intervention was individualized to address information about the illness, long-term management, health, and lifestyle modifications. The patient was encouraged to organize the daily activities in a structured manner, take regular breaks, and prioritize tasks based on energy levels that can effectively manage and minimize fatigue. The patient is on regular follow-up. She is doing well with the treatment and can manage her daily tasks. There were no neurological or psychological symptoms subsequently. A discussion about marriage-related concerns and plans was initiated during a recent follow-up.
Case 4
Ms. SL, 22 years old, female, single, studied up to electronic engineering, trained classical dancer, currently employed, hails from Kerala, approximately 575 km from the hospital. In the first episode, she complained of an imbalance while walking and a tingling sensation. Later, she developed a blurring of vision in both eyes. She underwent treatment for the same, and the neurological symptoms responded well to the disease-modifying therapy. The psychosocial assessment was conducted, and partial knowledge about the illness and management was elicited. However, she was able to manage the psychological distress and anxiety of having developed the neurological illness that interfered with her love of dancing and was adequately coping with the illness. Ms. SL was premorbidly well adjusted, and there was no significant personal history. No neuropsychiatric problems were identified. The patient had partial insight regarding managing illness and the need for regular management. The intervention was individualized to focus on information and support, with “maintaining hope” being the core tenet. Through this process, she was empowered with knowledge about illness and building a supportive social network to promote well-being. The patient’s functionality improved after discharge, and she could perform regular activities. The patient experiences anxiety, which is primarily tied to disease, and anxiety reduction strategies were continued during the follow-up session. Since her last stay in 2023, the patient has been symptom-free and healthy. The patient enjoyed extracurricular activities, such as dance and resumed them after discharge.
Case 5
Ms. TJ is 30 years old, female, married, graduated in engineering, unemployed, and hails from Andhra Pradesh. She presented with a recent onset of numbness, imbalance while walking, and fatigue. She was admitted for management of neurological problems. A diagnosis of remitting relapsing MS was made, and she was managed with diseasemodifying therapy. The patient had a good response to the treatment and was symptomatically doing better. A routine psychosocial assessment was carried out, and psychosocial factors were reviewed. The evaluation showed that the patient had partial knowledge of the illness. The sudden onset of neurological symptoms was a source of psychological distress, and she expressed her difficulty in managing her worries and had significantly disturbed sleep. At the family level, adequate support was present. A therapeutic alliance could be established, and the patient and family members wanted to work on addressing the illness better. Ms. TJ was premorbidly well adjusted, and there was no significant personal history. A psychiatry referral was given, and medication was prescribed for sleep disturbances.
However, no major neuropsychiatric diagnosis was made. Fatigue management, a healthy lifestyle, and stress management were the focus of the intervention. Sessions also emphasized offering stress management techniques, including mindfulness-based activities and coping strategies, to enhance overall well-being and resilience. On follow-up, the patient reported a 70% improvement in neurological symptoms, particularly numbness in the upper limb, urinary urgency, and walking speed, although fatigue remained. This improvement was also noted in the EDSS scores, which improved from 5 to 4 and then to 2.5. The patient was on regular medication, both neurological and psychiatric. In subsequent follow-up visits, the patient continued to complain of fatigue and low moods. However, there was a significant improvement in the overall functionality and activities of daily living.
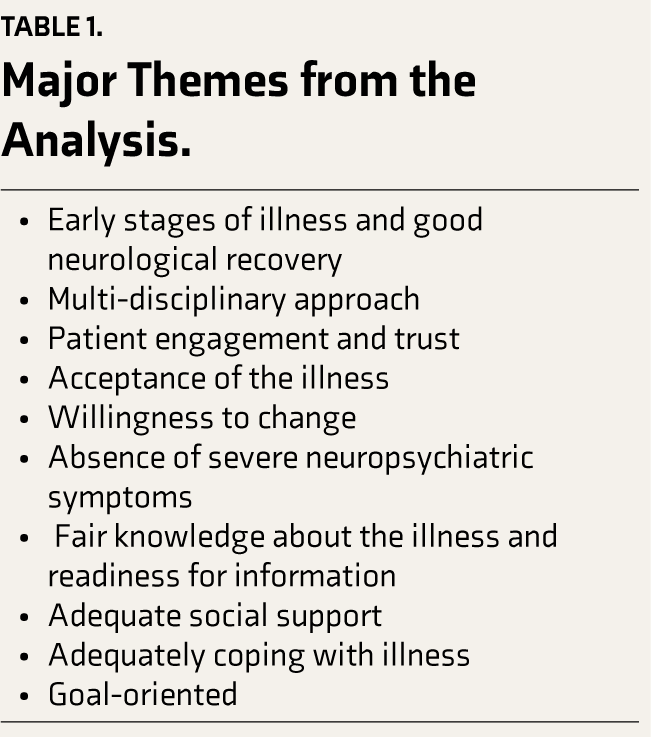
The case notes and assessment findings were subjected to thematic analysis using the framework method to elicit significant themes in this series. Table 1 gives the major themes that emerged as factors influencing self-management outcomes.
Major Themes from the Analysis.
Discussion
The present case series reports self-management interventions in the early stages of coping with MS. The patients had a good recovery from their neurological episode and subjectively reported being better adjusted and being able to cope better with the illness emotionally. The perceived impact of MS on the patient’s life was modifiable through the adoption of a self-management approach to adapting to the illness. This has resulted in positive changes in proactively coping with illness-related challenges. The participants in our study were self-motivated, and self-management education was provided early in their in-patient care. Post-discharge, participants reported the benefits of self-management measures during telephonic follow-up. Managing psychosocial aspects became less daunting, mainly due to the change in perspective to managing better and the support of family members. Similarly, Ghahari et al. 14 identified personal and contextual characteristics that helped patients self-manage and handle the challenges in their lives with the help of self-management strategies.
Most participants were in the early stages of the illness, in either the first or the second episode. All of them were functioning well before the development of the neurological problems and did not have any active neuro-psychiatric problems. MS was seen as an unexpected crisis that they figured out they needed to cope with. The main concern expressed by the participants was a desire to learn more about their illness and how long they would need to continue taking medication. Uncertainty about the future was a pervasive concern. Some of them only had basic information about their illness and the need for regular and long-term medication.
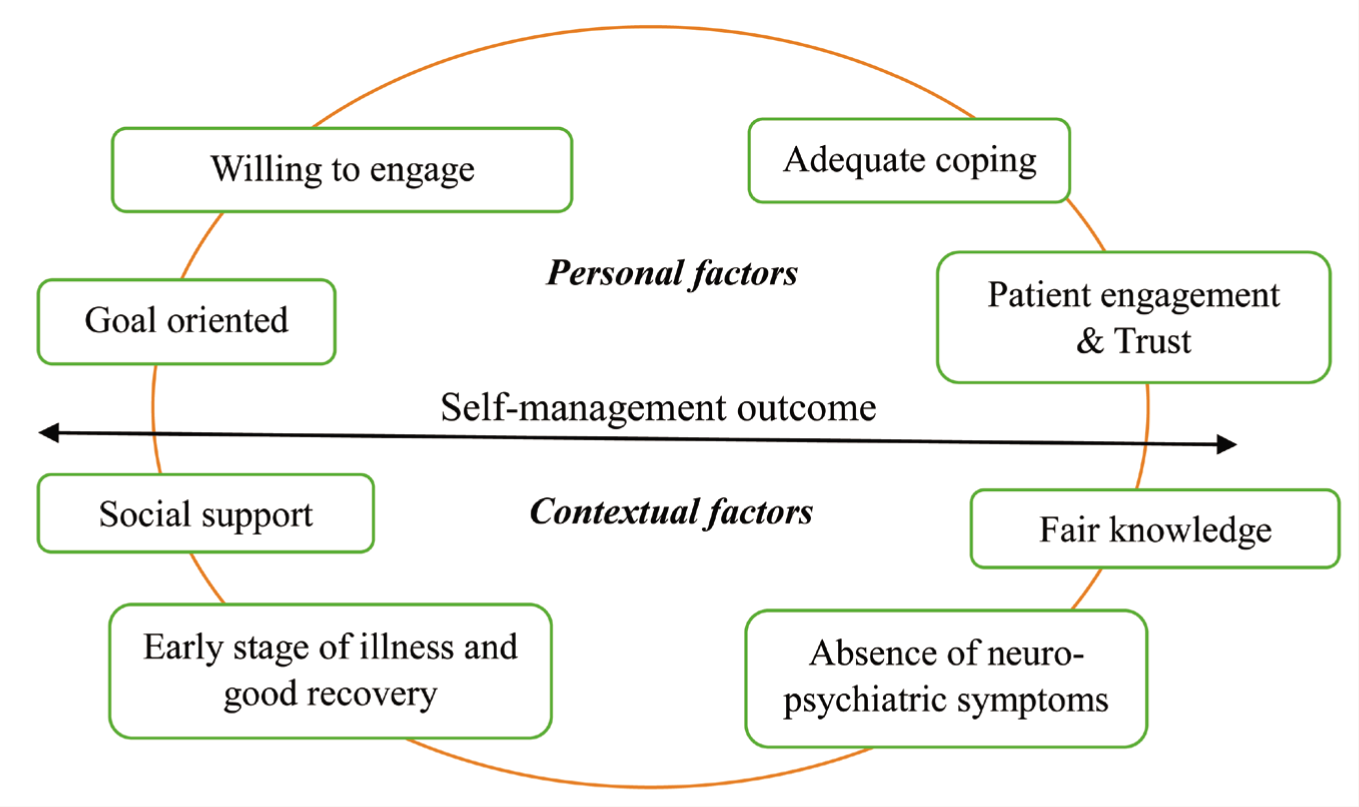
As mentioned by the participants, there was an emotional reactive distress response during the initial phase of diagnosis and treatment. However, the availability of support from various sources emerged as a key protective factor in some instances, assisting them in dealing with their challenges. The analysis identified some of the personal and contextual characteristics that could potentially influence the successful adoption of self-management interventions for clients (Figure 1).
Factors Influencing Self-management Outcomes.
Patient engagement has been advocated as important for chronic illness management and is identified as significant in better treatment adherence and improving quality of life. 19 These themes indicate the significance of internal and external loci of control, which motivate individuals to cope with MS. The review by Plow 20 points out that self-management strategies are helpful for people with MS in addressing their problems related to their psychosocial concerns, such as employment, education, family roles, etc., but they can often be context specific. It is suggested that individuals with neurological disorders can regain control over their lives by modifying their lifestyle and developing strategies to monitor their health. 21
The cultural context of illness management and chronic care can also play a major role in helping patients manage their illnesses better.
Conclusion
Multiple sclerosis is an autoimmune-mediated neurological disease that affects the psychosocial well-being of the individual living with it. Psychosocial interventions using a self-management approach can be a useful adjunct to MS management and will help the individual deal effectively with the illness. Self-management strategies need to consider individual and contextual factors and provide interventions that will support the individual in managing their illness better. Future research should focus on developing and testing culturally adapted self-management strategies tailored to the unique needs of individuals living with MS.
Footnotes
Acknowledgements
The authors would like to thank the participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding Generative AI
The authors are responsible for the entire manuscript content. Artificial intelligence tools have not been used in any part of the development of this case series.
Ethical Approval
The study has been approved by the Institute Ethics Committee (Behavioral Sciences), National Institute of Mental Health and Neuro-sciences.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Individual participant written consent has been obtained for the intervention as well as for publishing the content.