
Abstract
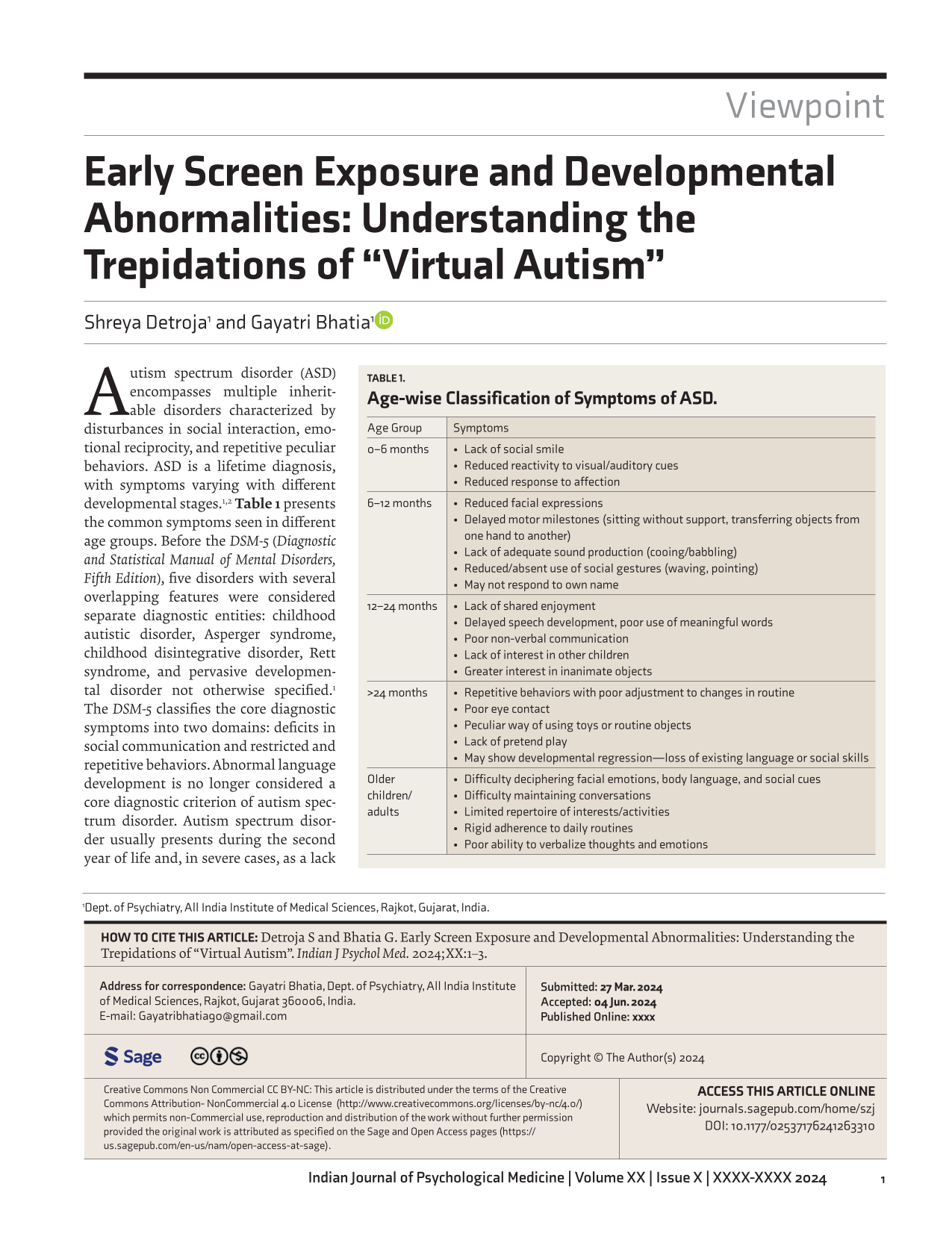
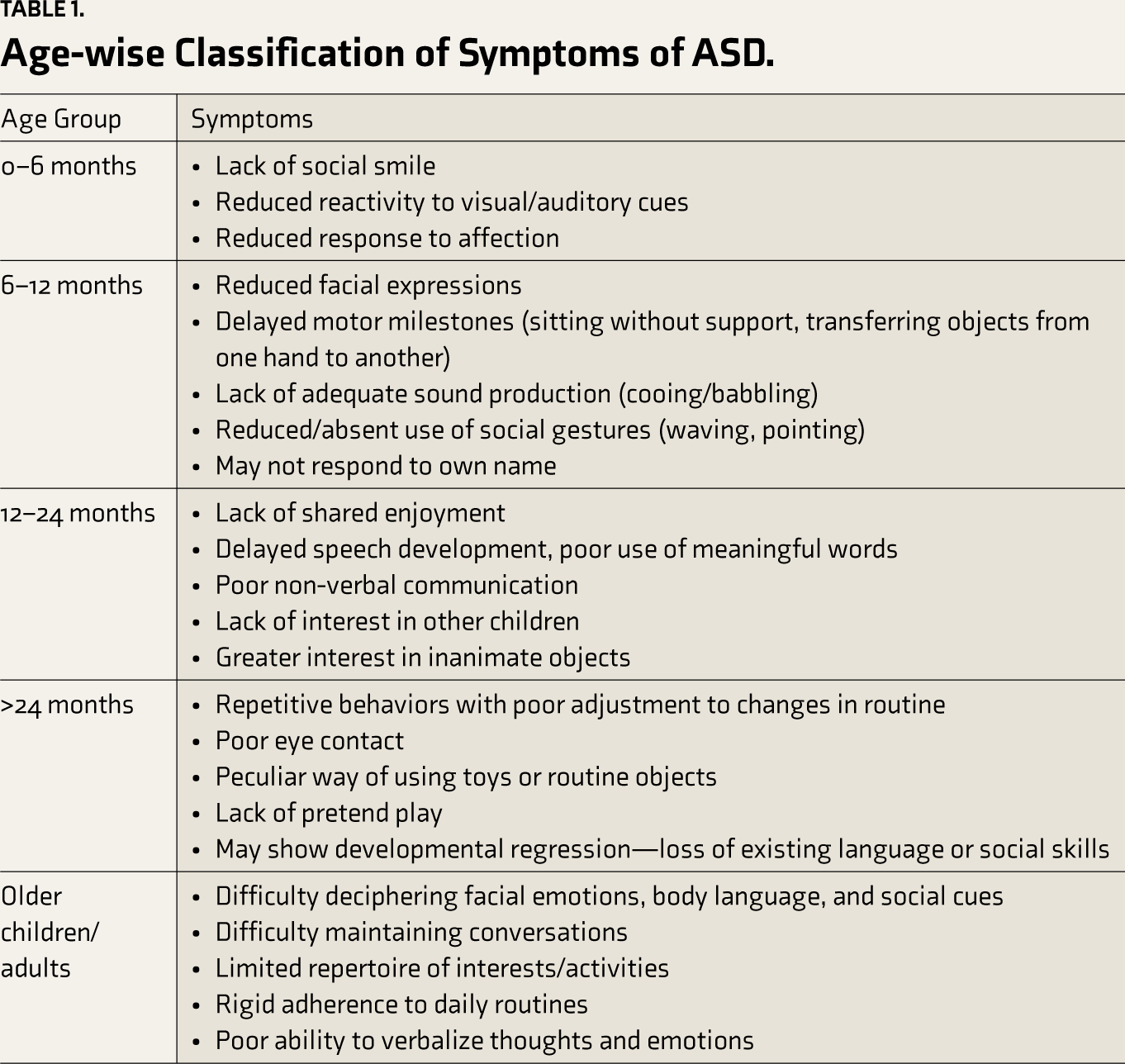
Autism spectrum disorder (ASD) encompasses multiple inheritable disorders characterized by disturbances in social interaction, emotional reciprocity, and repetitive peculiar behaviors. ASD is a lifetime diagnosis, with symptoms varying with different developmental stages.1, 2 Table 1 presents the common symptoms seen in different age groups. Before the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition), five disorders with several overlapping features were considered separate diagnostic entities: childhood autistic disorder, Asperger syndrome, childhood disintegrative disorder, Rett syndrome, and pervasive developmental disorder not otherwise specified. 1 The DSM-5 classifies the core diagnostic symptoms into two domains: deficits in social communication and restricted and repetitive behaviors. Abnormal language development is no longer considered a core diagnostic criterion of autism spectrum disorder. Autism spectrum disorder usually presents during the second year of life and, in severe cases, as a lack of developmentally appropriate interest in social interactions, which may be identified in the first year of life.1, 2 Evidence-based etiology includes genetic factors, immunologic factors, prenatal and perinatal factors, and comorbid neurologic disorders. Treatment options are psychosocial interventions, intensive behavioral programs, parental training, and participation, with academic and vocational interventions tailored to the needs of individual patients. 1
Age-wise Classification of Symptoms of ASD.
In 2018, Marius Zamfir, a Romanian psychologist, used the term “virtual autism” to describe behavioral abnormalities seen in children between zero and three years old, arising from sensory-motor and socio-affective deprivation caused by exposure to more than four hours/day of virtual environment. 3 According to Zamfir, the functional and developmental symptoms seen in such children were similar to childhood autistic disorder, as per DSM-4 and ICD-10. This was followed by several studies confirming the presence of “autism-like symptoms” in toddlers exposed to electronic screens excessively. Even though the evidence is too preliminary for it to be recognized as a diagnostic entity or included in current disease classification systems, several newspapers and magazine articles also warn parents about the risks and signs of virtual autism. 4 In this article, the authors explore the current research on virtual autism, discussing the various implications and considerations associated with it.
Current Research on Virtual Autism
Excessive screen exposure during the early years of life has been studied in several research papers for any relation to behavioral and developmental abnormalities in the past few years. A few of these papers have undertaken an objective evaluation of ASD symptoms using standardized tools, including M-CHAT (Modified Checklist for Autism in Toddlers), CARS (Childhood Autism Rating Scale), and ADI-R (Autism Diagnostic Interview-Revised). None of the existing studies have explored the use of specific modules of psychological interventions, pharmacotherapeutic agents, or a combination of the two, apart from the withdrawal of screens and the introduction of regular social contact. According to these studies, screen use was associated with young children being less active, less verbal, and less social than expected as per developmental norms, increasing the risk of developmental delays, behavioral problems, and ASD symptoms (avoidance of eye contact, discomfort in understanding social cues, delayed language development, poor non-verbal communication, and poor tolerance to variation in routine activities). 5 An earlier review by Harle et al., which included several case studies, reported improvement in symptoms by stopping screen exposure and encouraging dyadic interaction between parents and children and drew a causal association between early screen exposure and ASD symptoms using Branford Hill’s criteria for causation, referring to this cluster of symptoms as virtual autism. 6
Research also suggests the possibility of a bi-directional relationship between screen time and symptoms of ASD. 7 A case-control study in Bangkok on children aged 15–48 months reported an association between early exposure, high frequency of TV viewing, and language delay. 8 A retrospective study comparing the screen time of 108 children with ASD and their typically developing (TD) siblings concluded that the ASD group had longer screen viewing time, started screen viewing at a younger age, and spent less playing time with their mothers than their TD siblings. 9 Another study conducted in Indonesia on nine children with symptoms of ASD showed that children who spent less than three hours per day viewing television had delayed language development and short attention spans. In contrast, children who spent more than three hours per day had greater language delays and shorter attention spans in addition to hyperactivity, indicating the deleterious effects of excessive exposure to screens on children on the autism spectrum. 10
A recent meta-analysis of 46 studies concluded that this association between screen exposure and ASD symptoms was not adequately supported in the existing literature. They also stated that although excessive screen use may pose some developmental risks, the mixed findings, the small effect sizes, and the correlational nature of the available research require further scientific investigation. They also put forth a complementary hypothesis that children with ASD may prioritize screen activities to avoid social challenges. 11 This evidence, while indicative of a mutually harmful association between screen exposure and developmental issues in the early years of life, begs the question of whether “virtual autism” is the appropriate terminology for its description and understanding.
Implications of “Virtual Autism”
The term “virtual autism” does make a certain sense, as the presenting symptoms, such as language delays, delayed social milestones, poor attention, etc., are quite similar to those seen in autism spectrum disorders. The name is also directly associated with the etiology, that is, excessive consumption of virtual environments. It may also contribute to sensitizing parents/caregivers about the risks associated with excessive screen exposure in the initial years of life, thus leading to preventive steps and early identification of behavioral signs, enhancing help-seeking. However, it also carries the ominous connotations associated with a diagnosis of any autistic spectrum disorder, such as persistent abnormal behaviors, language difficulties, affective and cognitive issues, suboptimal quality of life for both the patient and caregivers, the lifelong requirement of supportive services, along with low chances of recovery. 12 This may wrongly propagate stigma and misconceptions about the condition among the general public and the caregivers of the affected toddler.
Considering the neurochemical changes that may occur in young children with behavioral anomalies secondary to excessive screen exposure during the early years of life, studies indicated deficiencies in major neurotransmitter levels, including dopamine, acetylcholine, gamma-aminobutyric acid (GABA), and 5-hydroxytryptamine (5-HT).10, 13 These findings stand in contrast with some neurochemical alterations seen in ASD, notably GABA and 5-HT, whose levels are elevated along with those of Glutamate, while other neurotransmitters showed typical receptor polymorphisms altering their metabolism and biological activity. 14
As per definition, ASD is characterized by a lack of developmentally appropriate interest in social activity, with the essential condition that adequate opportunities for social interaction are provided. However, studies on virtual autism highlight the significant mediating role of poor parent-child interaction in the relation of excess screen exposure with the development of ASD symptoms, drawing attention to the fact that screen exposure may not always result in symptoms of ASD as long as adequate social interaction is provided to the child.10, 15 This raises further questions on whether virtual autism is the best terminology for this scenario.
Moreover, technological advancements in managing ASD utilize artificial intelligence and virtual reality-based interventions, showing positive outcomes in language development, cognitive functioning, and social learning.16, 17 A term like “virtual autism” may propagate misgivings and resistance against such interventions among those seeking help, also proving a barrier to further research and therapeutic advances in ASD.
Currently, research on virtual autism is dominated by case studies and narrative reviews and needs a larger volume of systematic evidence before being recognized as a diagnostic entity. It is probable that with emerging research, more similarities or differences with ASD will be brought to light. Some burning questions, such as whether this gamut of symptoms fits better in the autism spectrum or another diagnostic group or as a separate entity altogether, may be answered conclusively. Until then, other terminologies to denote this clinical picture may be adopted, such as neurodevelopmental disorder due to early screen exposure. This terminology has the benefits of including attention deficits and hyperactivity, which are commonly seen in children exposed to virtual environments at an early age but are not core symptoms of ASD, and also avoiding the false labeling of a disorder that is still not well understood. It also encompasses the reversibility aspect of virtual autism, based on the evidence that neurodevelopmental disorders may be reversed with treatment, providing hope for a normal life to the toddlers’ caregivers, who may perceive a grim prognosis with the term “virtual autism.” 18 While the process of detailed characterization of “virtual autism” is underway, it is important that scientifically verified information be disseminated to parents/caregivers in order to undertake timely preventive and remedial measures without the propagation of unfounded stigma and fear.
Conclusion
While there is no denying the occurrence of developmental delays and behavioral abnormalities in children exposed to excessive virtual environments during the early years of life, current research on the topic is limited. While Zamfir’s term “virtual autism” explains the symptom profile seen in these children, it is associated with some pitfalls, raising questions as to whether it is the best-suited term for the condition. Further research is needed in order to understand it better, draw clear parallels or contrasts with ASD, and find its rightful place as a diagnostic entity.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors declare that no AI generative tools were employed in preparing this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.