
Abstract
Dear Editor,
Foreign accent syndrome (FAS) is a rare speech disorder characterized by an individual’s sudden and involuntary alteration of their native language usage. 1 It can have a neurogenic or psychogenic etiology. FAS is typically associated with Broca’s aphasia, secondary to stroke, head injury, etc. 2 However, commonly dissociative disorder may also present with FAS. 2 In fact, the term “foreign accent-like syndrome (FALS)” specifically describes the psychiatric variant of FAS. 3 There have only been a few reports from India on FAS, describing both psychogenic 4 and neurogenic 5 presentations.
Intriguingly, FAS is rarely documented in Wernicke’s aphasia (WA) cases. WA, a subtype of fluent aphasia, typically manifests as impaired comprehension and production of meaningless speech. 6 This atypical association of FAS with WA, 7 superimposed by the overlap of neurogenic and psychological factors, is presented in this case. By exploring this rare occurrence, we attempt to contribute to understanding the complex interplay between language deficits and accent modification in neurological disorders.
This report describes a septuagenarian, a native Telugu speaker, who experienced acute-onset difficulty in communication and expressed herself in Deccani Urdu (DU), a completely different vernacular language. Telugu and DU are Telangana, India’s two commonly spoken vernacular languages. Local vernacular variants of FAS are rarely reported from India.
Case Report
A 75-year-old married female from a Hindu nuclear family residing in sub-urban Hyderabad presented to us with a history of change in her daily language from Telugu to DU and, therefore, difficulty in day-to-day conversations in the last two weeks. These symptoms began dramatically after an altercation with her husband, leading to a provisional diagnosis of dissociative neurological symptom disorder (6B60) and subsequent referral and hospitalization in the psychiatry unit for assessment. There was history of tobacco chewing since adolescence, hypertension, type 2 diabetes mellitus for 15 years (on treatment), and past stroke 1.5 years ago, followed by right hemiparesis, which resolved in six months. The differential diagnoses that were entertained were post-stroke dysphasia, apraxia/dyspraxia of speech, and malingering.
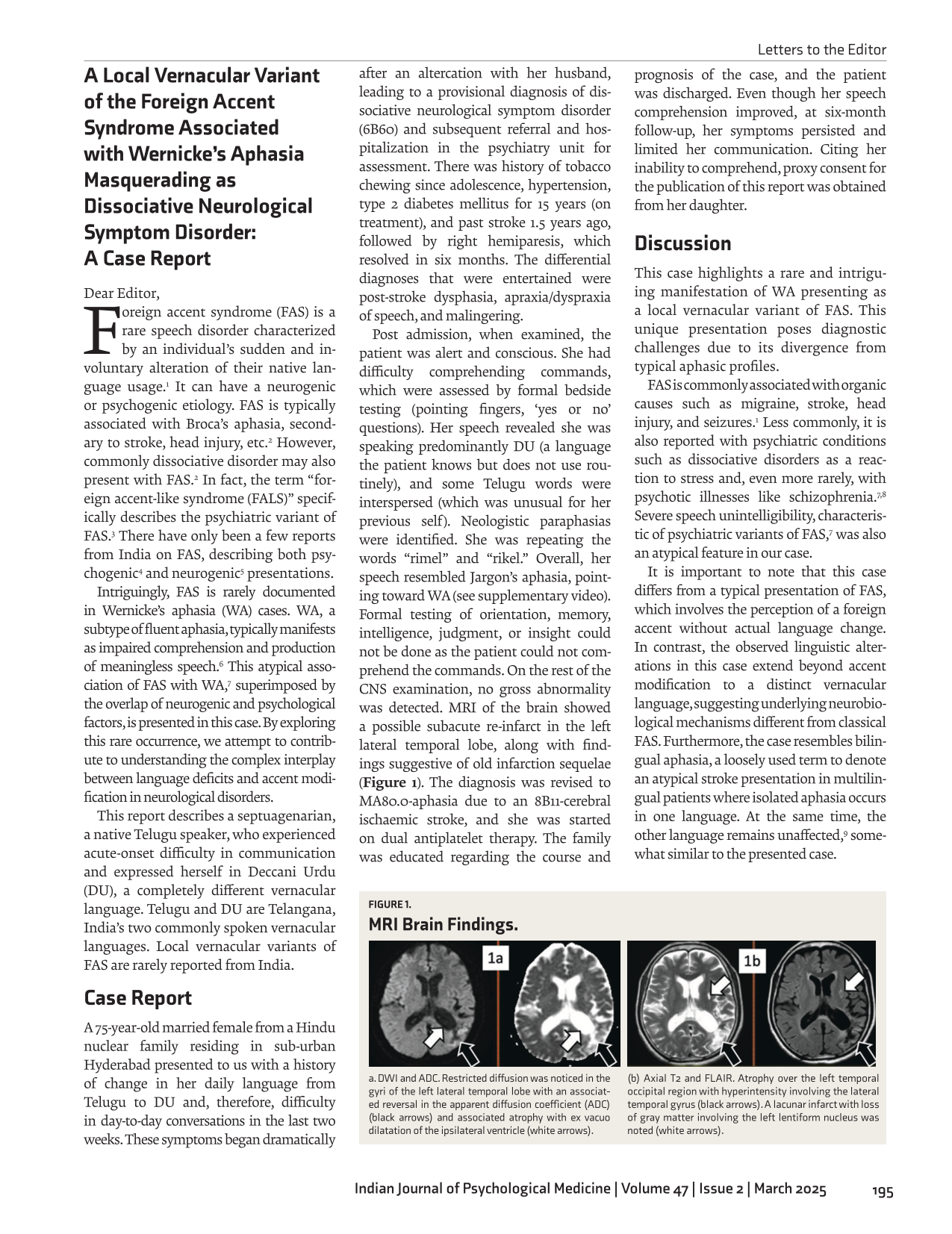
Post admission, when examined, the patient was alert and conscious. She had difficulty comprehending commands, which were assessed by formal bedside testing (pointing fingers, ‘yes or no’ questions). Her speech revealed she was speaking predominantly DU (a language the patient knows but does not use routinely), and some Telugu words were interspersed (which was unusual for her previous self). Neologistic paraphasias were identified. She was repeating the words “rimel” and “rikel.” Overall, her speech resembled Jargon’s aphasia, pointing toward WA (see supplementary video). Formal testing of orientation, memory, intelligence, judgment, or insight could not be done as the patient could not comprehend the commands. On the rest of the CNS examination, no gross abnormality was detected. MRI of the brain showed a possible subacute re-infarct in the left lateral temporal lobe, along with findings suggestive of old infarction sequelae (Figure 1). The diagnosis was revised to MA80.0-aphasia due to an 8B11-cerebral ischaemic stroke, and she was started on dual antiplatelet therapy. The family was educated regarding the course and prognosis of the case, and the patient was discharged. Even though her speech comprehension improved, at six-month follow-up, her symptoms persisted and limited her communication. Citing her inability to comprehend, proxy consent for the publication of this report was obtained from her daughter.
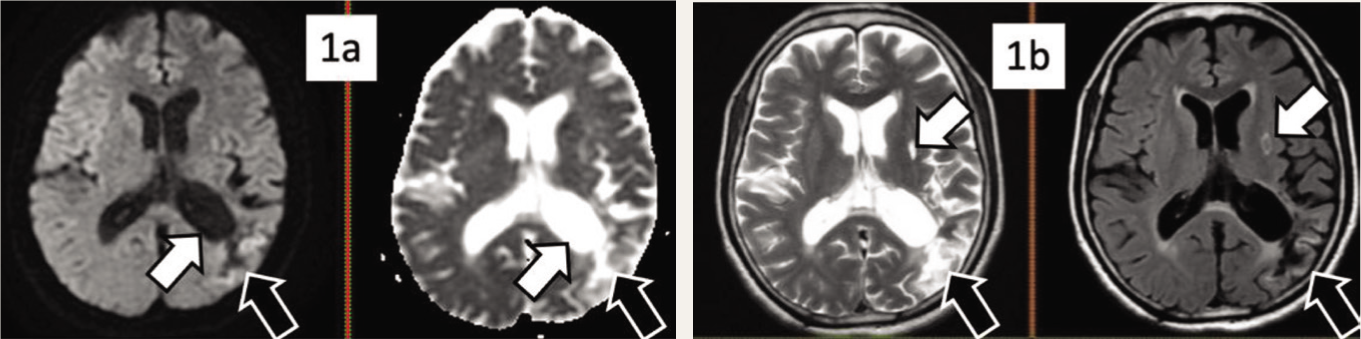
a. DWI and ADC. Restricted diffusion was noticed in the gyri of the left lateral temporal lobe with an associated reversal in the apparent diffusion coefficient (ADC) (black arrows) and associated atrophy with ex vacuo dilatation of the ipsilateral ventricle (white arrows).
Discussion
This case highlights a rare and intriguing manifestation of WA presenting as a local vernacular variant of FAS. This unique presentation poses diagnostic challenges due to its divergence from typical aphasic profiles.
FAS is commonly associated with organic causes such as migraine, stroke, head injury, and seizures. 1 Less commonly, it is also reported with psychiatric conditions such as dissociative disorders as a reaction to stress and, even more rarely, with psychotic illnesses like schizophrenia.7,8 Severe speech unintelligibility, characteristic of psychiatric variants of FAS, 7 was also an atypical feature in our case.
It is important to note that this case differs from a typical presentation of FAS, which involves the perception of a foreign accent without actual language change. In contrast, the observed linguistic alterations in this case extend beyond accent modification to a distinct vernacular language, suggesting underlying neurobiological mechanisms different from classical FAS. Furthermore, the case resembles bilingual aphasia, a loosely used term to denote an atypical stroke presentation in multilingual patients where isolated aphasia occurs in one language. At the same time, the other language remains unaffected, 9 somewhat similar to the presented case.
Neurobiological correlates of this phenomenon likely involve disruptions in language-processing networks, particularly within Wernicke’s area. This emphasizes the importance of neuroimaging in clarifying the underlying pathology in atypical aphasia presentations. A plausible explanation for using DU in the present case could be as a compensatory mechanism arising from her word-finding difficulties in her mother tongue, Telugu, which usually happens secondary to WA. 10 Her familiarity with DU also subdues the “foreignness” of the FAS.
Conclusions
This case highlights the complexity of speech disorders and the importance of considering broad differential diagnoses when approaching speech disorders.
Supplemental Material
Supplementary material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Proxy consent for the publication of this report was obtained from the patient’s daughter.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.