
Abstract

Alcohol abuse is associated with impairments in social functioning and medical problems. 1 Alcohol is one of the most commonly used substances globally and in India. According to a 2019 survey in India, 2.7% of the population is dependent on alcohol, which constitutes around 18.5% of total alcohol users in India. Alcohol causes physiological dependence, and withdrawal occurs when alcohol consumption is reduced or stopped. The severe form is called delirium tremens (DT). Between 5% and 20% of patients experiencing alcohol withdrawal experience DT.2,3
Mihai et al. hypothesized that the method’s efficacy, including a videotape of themselves, was comparable to the efficacy of the cognitive behavioral model. Psychiatrists used the videotape as evidence of impairment and as a tool for poor recall. Since videotapes provide visual stimuli, they have an emotional impact on the person and help gain the motivation to quit. 4
Patients exposed to the videotape during delirium experienced significantly lower relapse rates than controls. A single exposure delayed relapse by 101 days, and those who did relapse after exposure experienced less severe relapses, and the units of alcohol consumed and number of drinking days were comparatively lower. 4
The main goal of motivational interviewing is to resolve ambivalence and tip the scales toward the next stage of motivation. Strategies are verbal, persuasive, and supportive, to change motivation from within.5,6
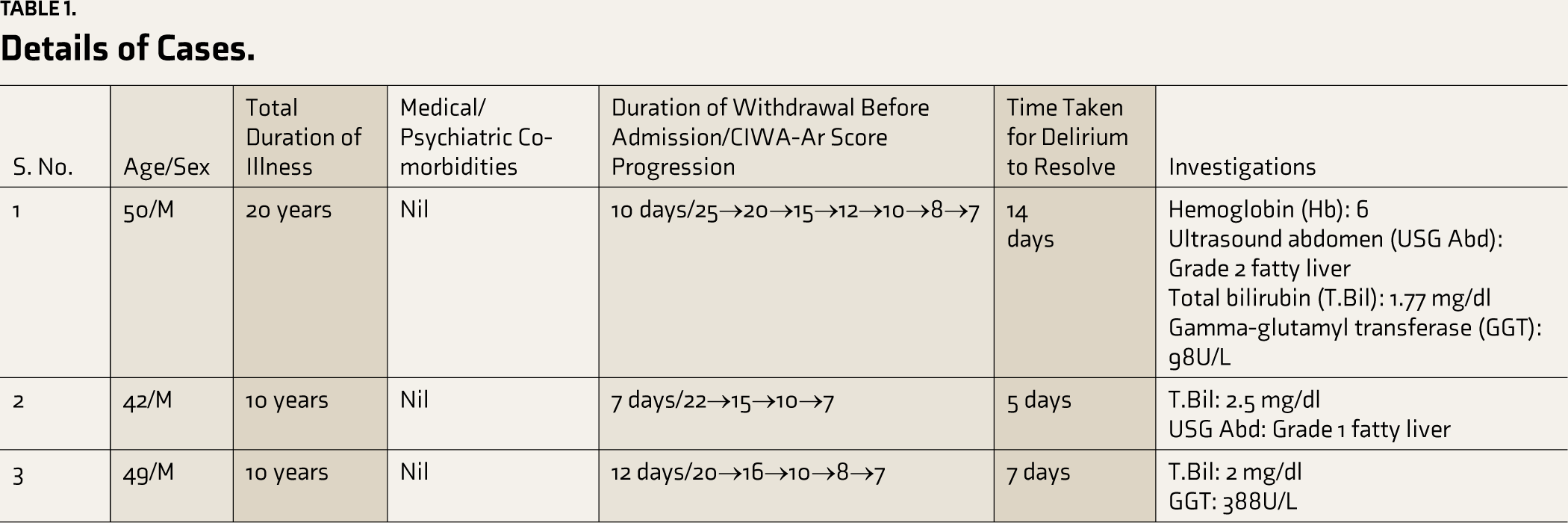
Videotape exposure focuses on changing motivation and uses visual stimuli to create a deeply ingrained effect. Research in this area is deficient, leading to research at hand. Here, we present three cases where video-recording-based feedback was used. We have obtained consent from patients for publishing these cases. Ethical committee clearance has been obtained from the institutional ethics committee. The details of the cases are presented in Table 1.
Details of Cases.
First Case
Mr M was diagnosed with alcohol dependence and having complicated withdrawal symptoms with DT. The general physical examination (GPE) revealed pallor with icterus, with the initial mental status examination (MSE) revealing a conscious but disoriented patient who was unkempt and untidy, with irrelevant speech, increased psychomotor activity (PMA), and a dysphoric mood. Subsequent MSE revealed that the patient had a pre-contemplation stage of motivation with a craving for alcohol with an external locus of control.
The patient was admitted for management of his DT with a long-term goal of abstinence. Detoxification was done with lorazepam in tapering dose, and prophylactic thiamine injections were used in a dose of 500 mg TID dose ATD for five days and subsequently changed to oral thiamine to prevent Wernicke’s encephalopathy and other conservative/symptomatic treatment as needed by the patient which is treatment as usual (TAU). The patient was also started on acamprosate as an anti-craving drug at a dosage of 1332 mg/day.
After the resolution of delirium, the patient was taken for non-pharmacological management, motivation enhancement therapy (MET) sessions every week after the resolution of delirium during a stay at the hospital for 60 days, and sessions continued for four more weeks after the discharge of the patient. A total of 10 sessions were conducted, each lasting for 40 minutes. Stressful situations and emotional disturbances were the most significant cues for relapse. The video that the patient’s sister recorded during his phase of delirium showed his confused behavior, his altered sensorium, and an incident of fall during which the patient sprained his left leg. The video lasted for around 3 minutes and 30 seconds and was used in all 10 MET sessions to increase the motivation of the patient. The patient was given psychoeducation regarding alcohol dependence and alcohol as a causal factor for current DT. The patient reported that the videos were more helpful in changing his motivation to seek further treatment. The video was also shown by the family at home in between sessions to stop the patient from drinking. The patient has maintained follow-up and abstinence for the past year, and this period of abstinence is comparatively more than the previous period of abstinence following admissions in rehabilitation centers which also provided MET sessions but without video.
Second Case
Mr V, brought by his wife, was diagnosed with alcohol dependence and is currently in complicated withdrawal with delirium. The GPE revealed icterus and pallor, and the initial MSE revealed a conscious and disoriented patient who is poorly kempt and tidy with irrelevant speech, PMA, and irritable mood. On subsequent MSE, it was found that the patient had a contemplation stage of motivation with a craving for alcohol with an external locus of control.
The patient was managed with TAU and was started on naltrexone as an anti-craving drug with a 50 mg/day dosage and taken up for MET sessions every week during the stay for 30 days, and eight more sessions were conducted following discharge every two weeks. In total, 10 sessions were conducted, each lasting 45 minutes. The patient’s wife recorded the video of his disinhibited behavior of disrobing himself, abusive behavior toward family, confused behavior, and altered sensorium. This video lasted for around 4 minutes and 45 seconds and was used in all 10 MET sessions with the consent of the patient and family to increase the motivation of the patient. The patient was shown these videos at home as well by family members when the patient expressed a craving for alcohol, and the patient reports that he developed disliking toward alcohol whenever he saw the video. The patient reported that he felt ashamed of his behavior in the video and developed an aversion to alcohol by seeing the video, which is why he decided to seek treatment this time, wherein he had refused treatment several times before this event. The patient is abstinent and has followed up for five months after discharge.
Third Case
Mr D, brought by his wife, was diagnosed with alcohol dependence syndrome and is currently in complicated withdrawal with delirium. The GPE revealed pallor, icterus, and pedal edema, and the initial MSE revealed conscious and disoriented patients with irrelevant speech and increased PMA. Subsequent MSE revealed that the patient had a pre-contemplation stage of motivation with a craving for alcohol with an external locus of control.
The patient was managed with TAU and was started on acamprosate as an anti-craving drug with 1998 mg/day and taken up for MET sessions every week during the stay for 30 days, and eight more sessions were conducted following discharge. Ten MET sessions were conducted, and each session lasted 45 minutes. The family members recorded two videos to show the doctors and one video portrayed his disoriented behavior where he was searching for his family members when they were right in front of him, and this lasted for around 2 minutes and 10 seconds. The social setting was the significant cue for relapse. The other portrayed an episode of generalized tonic-clonic convulsions that lasted for around 2 minutes and 45 seconds. Both these videos were used in all 10 MET sessions with the patient’s consent. The patient was given psychoeducation regarding alcohol dependence and complicated withdrawal with seizures and delirium and their connection with alcohol. Initially, the patient reported he was uncomfortable watching the video, felt ashamed of his behavior in the video, and felt guilty about its effect on his family. So, the patient decided to maintain his abstinence, and the patient has been maintaining follow-up and abstinence for the past eight months, which is comparatively more than the previous period of abstinence following admission in a rehabilitation center where MET sessions were given but without video.
Discussion
Many pharmacological and non-pharmacological treatments are being used for relapse prevention. US-FDA (United States Food and Drug Administration) approved drugs for relapse prevention in alcohol dependence are disulfiram, with fair evidence, and naltrexone and acamprosate, with good evidence. Other drugs used are SSRIs (selective serotonin reuptake inhibitors), ondansetron, and topiramate with insufficient evidence. 7 Naltrexone increased the time to first relapse. 8 A meta-analysis showed that naltrexone decreased relapse rates with a relative risk of 0.64. However, it did not increase absolute abstinence from alcohol. 9 Acamprosate is found to be better than placebo in maintaining abstinence. 10 Absolute abstinence was twice as high in combination treatment with naltrexone and acamprosate than individual drugs. 11 In a meta-analysis, it was seen that participants who were treated for alcohol use disorder had 43% of abstinence rates, which extrapolates into 57% of relapse rates.12,13 Relapse rates in the long term were as high as 80%, ranging from 20% to 80%.14,15
According to Dieperink E et al., MET showed the highest efficacy at three months post-therapy. Before MET, participants had 34.98% abstinence days, which increased to 69.91% after MET. Average drinks in one week decreased from 35.45 to 14.6 in 3 months. However, complete abstinence could not be achieved. 16
Relapse prevention would be a cognitive behavioral approach with two specific aims: prevention of lapse and maintenance of abstinence, along with management of lapse if it were to happen. 17
The effect size for alcohol use for relapse prevention was r = 0.37 with 95% confidence intervals. 18
Aversion therapy is a form of behavioral therapy that aims to modify or reduce unwanted or dangerous behaviors. An aversive stimulus breaks the reward system and associate behavior with painful or negative experiences. 19 This works on the principle of aversive conditioning or counterconditioning. It can be based on either medications, chemicals, electrical aversion, verbal or visual aversion, or any other sensation that may be utilized. 20 Common aversive agent used in alcohol use disorder is disulfiram. 21
In a study by Fuller et al., it was seen that there was a significant relationship between adherence to the drug and complete abstinence, and disulfiram helps in relapse prevention in patients who are compliant with the drug. 22
In the cases described above, in which patients were admitted to tertiary psychiatric care centers, we utilized videos captured by family members on their mobile phones as a visual aversive agent. The videos on the phones of family members’ phones were utilized without any transfer to our mobiles to maintain the privacy of the patient. The video that the family members themselves took during the period of delirium in patients helped increase the motivation of the patient to seek treatment or be abstinent. Before the utilization of videos for therapy, patients were asked for consent, and all the patients agreed to it. The same video was utilized in all therapy sessions. These videos portrayed the symptoms of delirium, such as disorientation to time, place, and person, agitation, abusive behavior, or disinhibited behavior. Patients were offered a detailed explanation of all these symptoms and the connection between the symptoms and alcohol dependence. The psychologist provided these sessions with an accompanying psychiatrist.
Patients experiencing DT do not recollect events, and video helps recover their memory. Two patients described the video as an aversive stimulus that created discomfort. So, we propose using videos showcasing the patient’s behavior in delirium as an aversive stimulus in an aversive therapy. The video is an aversive visual stimulus without side effects like disulfiram. This video may be used as an additional tool in MET to change motivation and nudge them toward abstinence. The latest advances to tackle cravings include virtual reality cue exposure therapy (VR-CET). VR-CET uses videos to expose the patient to various cues inducing cravings. 23 But video record viewing of self in delirium tremens (Vvsdt) uses videos involving patients themselves, which might have more impact.
It will be very helpful in distant or resource-poor situations because it does not require additional resources, financial backing, or specific training. Considering all the literature, we propose VVSDT either as a part of motivational enhancement therapy or as an independent aversion therapy with the patient’s consent.
Footnotes
Acknowledgements
No prior presentation of the case series has been done.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No AI tools have been used to collect or analyze data, produce images or graphs, or write this article.
Ethical Approval
Ethical committee clearance has been obtained from institutional ethics committee with letter number Spandana EC/4/2021.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.