
Abstract

Dear Editor,
Early-onset Parkinson’s disease has an onset between 20 and 40 years of age, and juvenile-onset Parkinson’s disease is diagnosed when the disease emerges before 20 years of age.1,2 Several mutations have been linked to early onset and juvenile-onset Parkinson’s disease. This report highlights the difficulties encountered in diagnosing and treating a patient with Juvenile-onset Parkinson’s disease along with treatment-resistant psychotic symptoms.
Case Report
A 15-year-old boy presented to the general hospital psychiatry unit of our tertiary care teaching hospital with a 1-year history of slowness of movements, stooped posture, and bent knees. All these motor symptoms gradually progressed. After about 6 months of the onset of motor symptoms, he developed auditory hallucinations and persecutory delusions. There was no history of substance abuse or seizures. There was a family history of paranoid schizophrenia in his father.
Neurological examination revealed a shuffling gait (he took short steps with bent knees and a stooped posture). Bradykinesia, cogwheel rigidity, and resting tremor were present. Features of Parkinson-plus syndromes like cranial nerve abnormalities, eye movement abnormalities, dysarthria, ataxia, and cognitive impairment were absent. Prominent and disturbing auditory hallucinations were the most striking abnormality on serial mental status examinations over several weeks.
Complete blood count, renal function tests, liver function tests, thyroid function tests, blood sugars, and lipid profiles were normal. Wilson’s disease was ruled out due to the absence of a Kayser–Fleischer (KF) ring and normal serum ceruloplasmin. Electroencephalogram and magnetic resonance imaging of the brain (MRI brain) did not reveal any epileptiform activity or structural abnormality. Genetic testing revealed a heterozygous missense variant(c.5000G>A; p.Gly1667Asp) in exon 43 of the DNAJC13 gene (chr3:g.132507238G>A; Depth: 83x) that resulted in the amino acid substitution of aspartic acid for glycine at codon 1667 (p.Gly1667Asp; ENST00000260818.11) A final diagnosis of Juvenile-onset Parkinson’s disease and organic psychotic disorder was made.
There was no improvement in psychotic symptoms with adequate trials of olanzapine (up to 20 mg per day) and Quetiapine (up to 800 mg per day). His neurological symptoms were initially treated with Amantadine (200 mg per day) and Trihexyphenidyl (4 mg per day). As the improvement of symptoms was partial, a trial of Pramipexole (0.5 mg per day) was tried for 1 month along with the above medications. Psychotic symptoms persisted unabated during the pramipexole trial, but there was no worsening. Fluoxetine (20 mg/day) was also added due to prominent depressive symptoms with suicidal ideas in response to persistent auditory hallucinations. At the time of writing this report, the patient was on a combination of Clozapine 200 mg/day (due to previous two failed antipsychotic trials), Trihexyphenidyl 4 mg/day, and Fluoxetine 20 mg/day. Psychotic symptoms were prominent, whereas a partial improvement in neurological symptoms was noted.
Discussion
In this report, we have presented a young boy who presented with neurological and psychiatric symptoms and the approach taken to reach the diagnosis. Also, the lack of response to standard antipsychotic treatments in this patient is highlighted.
Drug-induced parkinsonism was considered due to the co-occurrence of anti-psychotic use and parkinsonian symptoms. This was quickly ruled out, as the motor symptoms had started several months before the onset of psychotic symptoms. Wilson’s disease was strongly considered due to the presence of co-existing neurological and psychiatric symptoms in a young boy. It was ruled out using standard blood (normal serum ceruloplasmin) and ophthalmological evaluations (absence of KF ring). Blood investigations and brain imaging ruled out other metabolic and intracranial abnormalities. Genetic testing was considered, considering the early age of onset and the presence of prominent motor and Parkinsonian symptoms. It revealed a rare missense variant in the DNAJC13 gene. Other rare missense variants in this gene have been reported in patients with Parkinson’s disease.3–5 Even though many studies have demonstrated the association of DNAJC13 mutations in familial PD and early-onset Parkionson’s disease3,6–8, the etiological role of this has not been proven. Some studies have shown similar mutations in the control population. Hence, they may play a relatively minor role in the etiology of PD. 9,10
Juvenile-onset Parkinson’s disease has been linked to mutations in parkin, PINK1, and DJ1. 2 SNCA region was implicated in a genome-wide association study in early-onset Parkinson’s disease in India. 11 Genetic analysis of first- degree relatives, particularly his father (who had otherwise typical symptoms of schizophrenia without any neurological symptoms and showed complete recovery with antipsychotic treatment) was considered but could not be carried out due to cost constraints.
Quetiapine and olanzapine were the initial antipsychotic medications used in this patient as they have a lower propensity to induce drug-induced parkinsonism. A clozapine trial was initiated after documenting a lack of response to adequate trials of both these antipsychotic medications. Unfortunately, this patient’s response to clozapine was also unsatisfactory.
On the Brief Psychiatric Rating Scale (BPRS), 12 scores were 47–53 during all the assessments. Clinical Global Impression – Severity (CGI-S) 13 was rated as six at baseline, indicating a severely ill patient. Clinical Global Impression – Improvement (CGI-I) 13 was rated as 4, indicating no change from baseline during all three antipsychotic trials (see Table 1). Parkinsonian symptoms were treated with Trihexyphenidyl 4 mg per day and Pramipexole 0.5 mg per day, and a significant improvement in motor symptoms was noted.
Severity of Psychotic Symptoms at Baseline and During the Follow-up Visits.
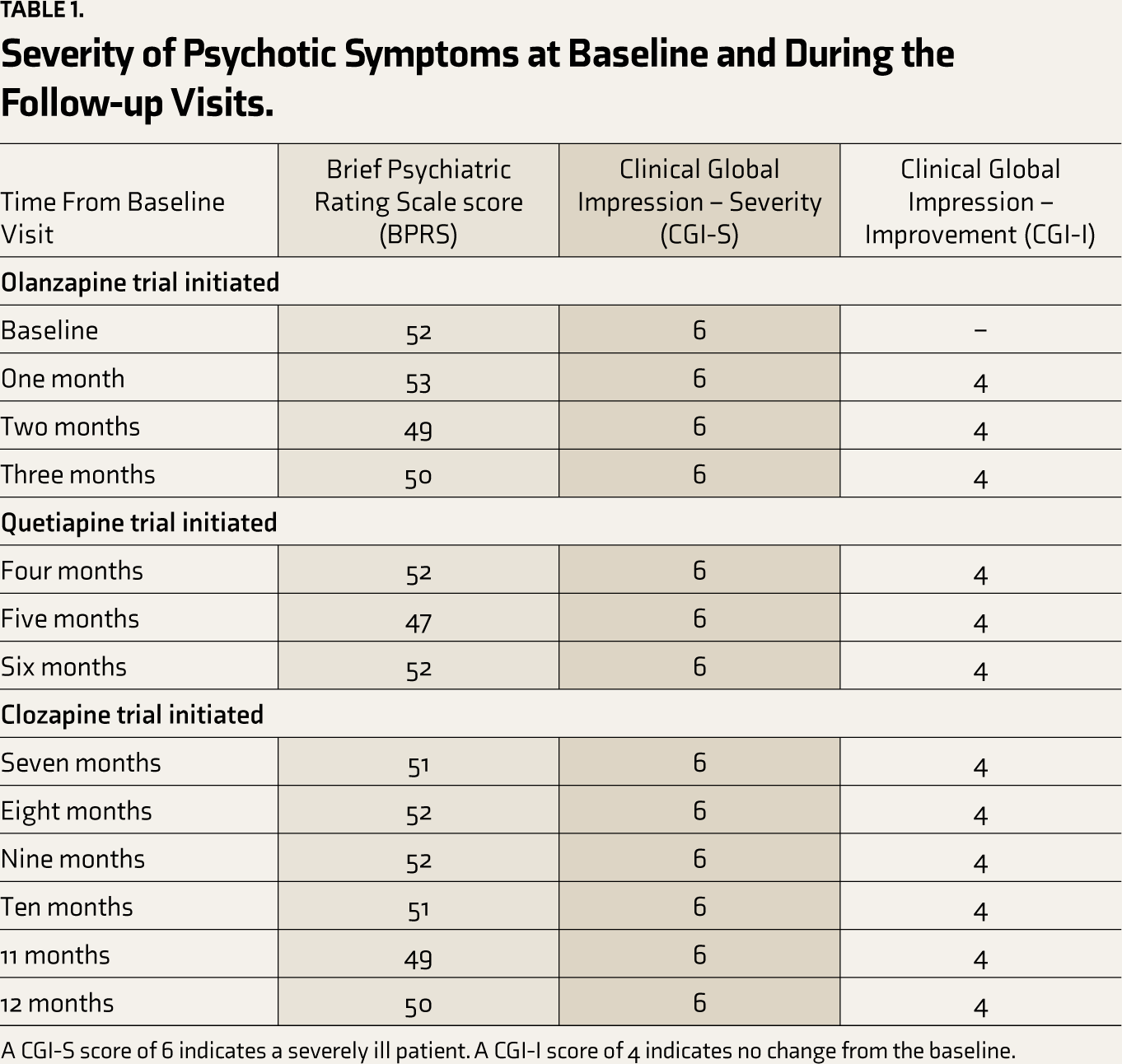
A CGI-S score of 6 indicates a severely ill patient. A CGI-I score of 4 indicates no change from the baseline.
Conclusion
Careful consideration of differential diagnosis and systematic evaluation is necessary to reach an accurate diagnosis in patients with motor and psychotic symptoms. Treatment involves gradual titration of antipsychotic and antiparkinsonian medications under close clinical monitoring.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval and Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. Institute Ethics Committee approval was obtained for publication (RC/2024/34).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.