
Abstract

Dear Editor,
Early identification may lead to improved outcomes 1 in treatment- resistant schizophrenia (TRS), a condition otherwise associated with worse clinical and functional outcomes. 2 Microbiomes, both gut 3 and oral, 4 influence brain functioning via the hypothalamic–pituitary–adrenal (HPA) axis, vagus nerve, tryptophan metabolism, and immune modulation, which makes them a biomarker candidate for TRS.
Microbiome studies in schizophrenia have reported alpha (within-group) diversity and beta (between-group) diversity. 5 Only two studies have studied gut microbiome and treatment response. One reported dysbiotic (imbalanced) gut microbiota composition at intake predicted response to treatment at 12 months in first-episode patients, 6 while the other 7 reported differences in microbial structure between TRS and the responsive group. Considering alpha diversity has been recommended 8 as a promising predictor for schizophrenia and given that the oral microbiome has the highest alpha diversity, we aimed to study whether alpha diversity measures in the oral microbiome could distinguish between TRS and treatment-responsive groups. This has yet to be studied.
Fourteen consenting patients with Diagnostic and Statistical Manual of Mental Disorders (DSM-V) 9 schizophrenia, including seven with TRS as per treatment response and resistance in psychosis criteria 10 , were recruited from a subacute psychiatric unit in Australia. The “treatment-responsive” group did not meet the criteria for TRS. 2 The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the local Research Ethics Committee (HREC 2020/ETH00136). We collected socio-demographic measures, anthropometric scores, and clinical information, including psychotic symptoms, cognitive functioning, oral health, and substance use.
Saliva was aliquoted into two 2-mL cryovials each, transported on ice, and stored in a –80°C freezer before sending for deoxyribonucleic acid (DNA) extraction. The V3–V4 region of the 16S ribosomal ribonucleic acid (rRNA) gene was amplified by Polymerase Chain Reaction (PCR) and sequenced on the Illumina MiSeq platform using 300 bp paired-end chemistry. Sequenced reads were clustered into taxonomic groups (amplicon sequencing variants [ASVs]) using the naïve Bayes taxonomy classifier pretrained on the SILVA v132 database. Data were imported into R (version 4.0.2), and putative exogenous ASVs were identified and removed using the package decontam (version 1.14.0).
Alpha diversity (Shannon and Simpson index, Chao 1, and observed ASVs) and beta diversity (weighted Unifrac metrics) were studied. Statistical tests included the Wilcox test to assess differences in alpha diversity between treatment-responsive and TRS groups and permutational multivariate analysis of variance (PERMANOVA) on the Unifrac distances for associations between the treatment response (TRS or treatment-responsive) and the overall microbial community. Linear regression models were used to identify relationships between treatment response and taxa at phylum, family, and ASV levels, and p-values were corrected for multiple testing using a false discovery rate (FDR). Alpha and beta diversity analyses were repeated to test for differences in the oral microbiota associated with oral hygiene, obesity, or diabetes. Socio-demographic and clinical characteristics were compared using Student’s t-test or Fisher’s exact tests. Visualizations of the data were generated using the ampvis2 package (ampvis2_2.7.17).
The two groups did not differ in socio-demographics, substance use, oral hygiene, obesity, or diabetes status. During the COVID lockdown, the participants recruited from the same unit ensured they all had similar diets. TRS groups performed worse on total psychotic symptom scores (P = 0.003) and cognitive scores (P = 0.012) (Table 1). We found 1810 ASV in the 14 samples, indicating a complex oral microbiota. The TRS group had significantly increased Alpha diversity (Wilcox test; P < 0.023, FDR = 0.125), family Nocardiaceae and Actinomycetaceae (phylum Actinobacteria), Flavobacteriaceae (phylum Bacteridetes), and Desulfomicrobiaceae (P < 0.015, FDR < 0.12), and a decrease in ASV related to Gemella (phylum Firmicutes) (P = 0.003, FDR = 0.17) compared to the treatment responsive group. Secondary analysis performed showed that cognitive function was not associated with alpha diversity (Wilcox test, P > 0.07) or beta diversity (ADONIS, weighted Unifrac distances, P > 0.1).
Summary of Socio-demographic and Clinical Variables.
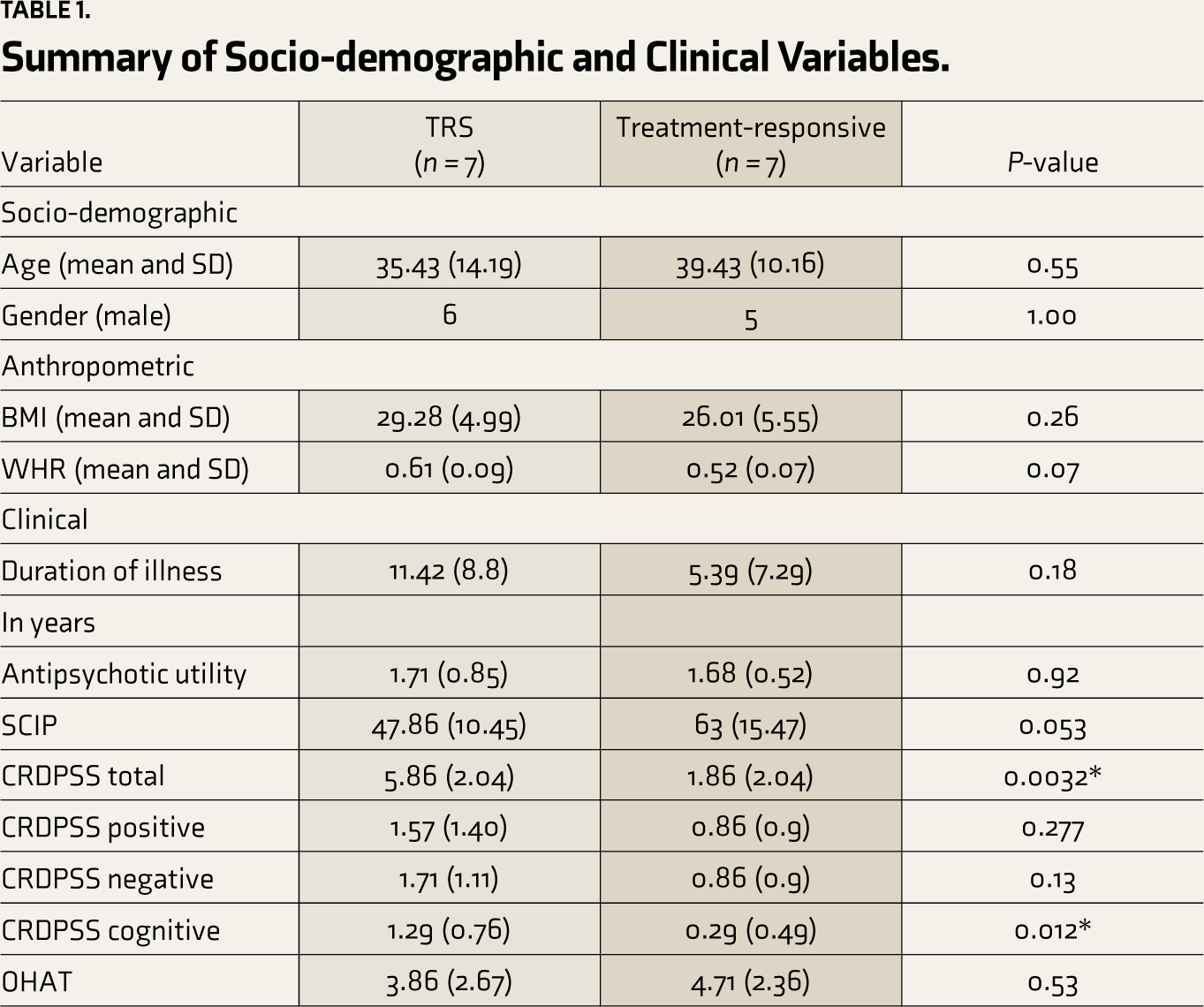

TRS: treatment-resistant schizophrenia; Non-TRS: non-treatment resistant schizophrenia; BMI: body mass index; WHR: waist-to-hip ratio; SCIP: screen for cognitive impairment in psychiatry; CRDPSS: clinician-rated dimensions of psychotic symptoms severity; OHAT: oral health assessment tool.
Observed ASVs, Chao1, Shannon, and Simson diversity in TRS (blue) and in the treatment-responsive (red) group.

Even though oral microbiota contributes only 5% of the gut flora 11 and our limitations of small sample size and absence of a healthy control group, our finding that oral microbiome differentiates patients with TRS from treatment-responsive patients supports its use as a potential biomarker for TRS. We speculate that the possible association between oral microbial diversity and treatment resistance in schizophrenia is mediated through the glutamate pathways or inflammatory changes. Alternatively, this could point towards an abnormal dietary pattern among TRS that changes oral microbial diversity. The findings need to be validated in a larger cohort. Further research is needed to confirm these findings, which could improve identification and outcome in TRS.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Western Sydney Local Health District (LHD) Human Research Ethics Committee (HREC2020/ETH00136).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.