
Abstract
Purpose:
This systematic qualitative review explored how psychotherapists use their self in therapy within the psychotherapy literature. It sought to examine the key documented ways through which the therapist’s self is intentionally used in therapy and the process of using the therapist’s self.
Methods:
Following PRISMA guidelines, databases including PubMed, ProQuest, APA PsycArticles, and APA PsycINFO were searched. The review question “How do therapists use their self in therapy?” guided the search using derivative keywords. Of the 149 screened articles, 20 underwent full-text review, and only four studies met inclusion criteria.
Findings:
All studies that met the inclusion criteria were from the West. Therapeutic self-disclosure (TSD) emerged as the primary way through which therapists used their self in therapy—notably, the only way documented in the studies reviewed. Studies discussed the nature, rationale, influencing factors, and effectiveness of TSD. This article elaborates upon the themes from the reviewed studies. It critically examines existing literature, lists avenues for future research, and discusses implications for psychotherapy practice.
Conclusions:
The review underscores a significant gap in empirical qualitative research regarding therapists’ use of their self beyond TSD in therapy. There is an urgent need for further exploration in this domain.
Keywords
Therapists significantly influence the effectiveness of the therapeutic process 1 accounting for about 8% of the variability in psychotherapy outcomes,2,3 while the therapeutic relationship explains an additional 15%. 2 The therapist’s self plays a pivotal role in shaping this alliance, impacting perceptions of authenticity, empathy, and trustworthiness.4,5
Interest in individual and relational factors affecting therapy outcomes has surged in recent decades, highlighting the importance of evidence-based relationships and therapist contributions.2,6 Researchers have delved into understanding why certain therapists excel, 1 exploring various aspects of the therapist’s self, such as responsiveness, presence, and multicultural competence. 1 Effective therapeutic relationships hinge on therapist qualities such as empathy, genuineness, and the ability to manage countertransference. 2
The use of the therapist’s self in therapy refers to the conscious integration of the therapist’s personality, experiences, and feelings into the therapeutic process.7,8 The therapist is seen as a being with a unique set of characteristics that can be used to facilitate the therapeutic relationship and promote client growth. 9
Historically, different therapeutic schools have viewed the therapist’s self through different lenses, accorded it different degrees of importance, and offered differing insights on how it is best used in therapy. Early psychoanalysis marginalized the therapist’s personal qualities and emphasized neutrality, 10 emphasizing a neutral and detached stance, an objective therapeutic environment, and avoiding therapist self-disclosure (TSD). 11 In contrast, behaviorists were divided on the issue of the value of TSD. 12 While, classically, cognitive-behavioral therapy (CBT) has focused on the therapist’s “use of self” only insofar as it contributes to a collaborative therapeutic relationship,13,14 self-awareness and awareness of countertransference are considered important,12,15,16 with contemporary acknowledgment of the usefulness of appropriate self-disclosure.12,13,17
Humanistic-existential thinkers, particularly Rogerian therapists, emphasized the therapist’s connection to self for validating clients. 7 In contrast, existential therapists prioritized awareness of the therapist’s self at the moment and its role in fostering authenticity and reflection. 18 Self-disclosure in existential therapy is noted to be potentially beneficial with contextual considerations. 19
Relational shifts in psychotherapy have harbingered viewing therapy as an interpersonal process in which the therapist and client co-construct meaning, with the therapist being acknowledged as both affecting and being affected by the client. 20 This dynamic, recursive relationship emphasizes the therapist’s self as a crucial influence on the therapeutic alliance and outcomes.20,21 In this context, the self that the therapist brings to the therapy space has a critical influence on the nature of the relationship that ensues.
Postmodern psychotherapeutic approaches have furthered this recognition and brought about a novel paradigm by questioning whether neutrality in therapy is possible, given the subjectivity of experiences. 22 They have also promoted critical reflexivity toward one’s positions, assumptions, beliefs, values, and ethical self-disclosure. 23 Contemporary perspectives also recognize the impact of culture, diversity, and power dynamics on the therapist’s self.
The therapist’s self and personality are also invaluable to applying therapeutic techniques and interventions. Therapists’ expressions can elicit differences in their effectiveness in the therapeutic process. 24 Therapists bring resources, such as their authenticity and power, to help them move beyond artificially applied techniques. 24 These theories and techniques come to life through the therapist’s person. The self of the therapist is the funnel through which they become manifest. 25
The Present Review
The use of self in therapy, thus, is an essential component of psychotherapy. Empirical research on the use of the therapist’s self in psychotherapy, however, is still in its nascent stages.
Hence, this study aimed to systematically review and document empirical literature on how therapists bring their self into therapy, emphasizing the deliberate use of the self and not the inadvertent presence of the therapist. This intentional use is defined by how the therapist applies and extends aspects of their personality to influence the client therapeutically. The use of self thus involves the operationalization of personal characteristics so that they impact the client in such a way as to become potentially significant determinants of the therapeutic process. 26
Methods
Search Strategy
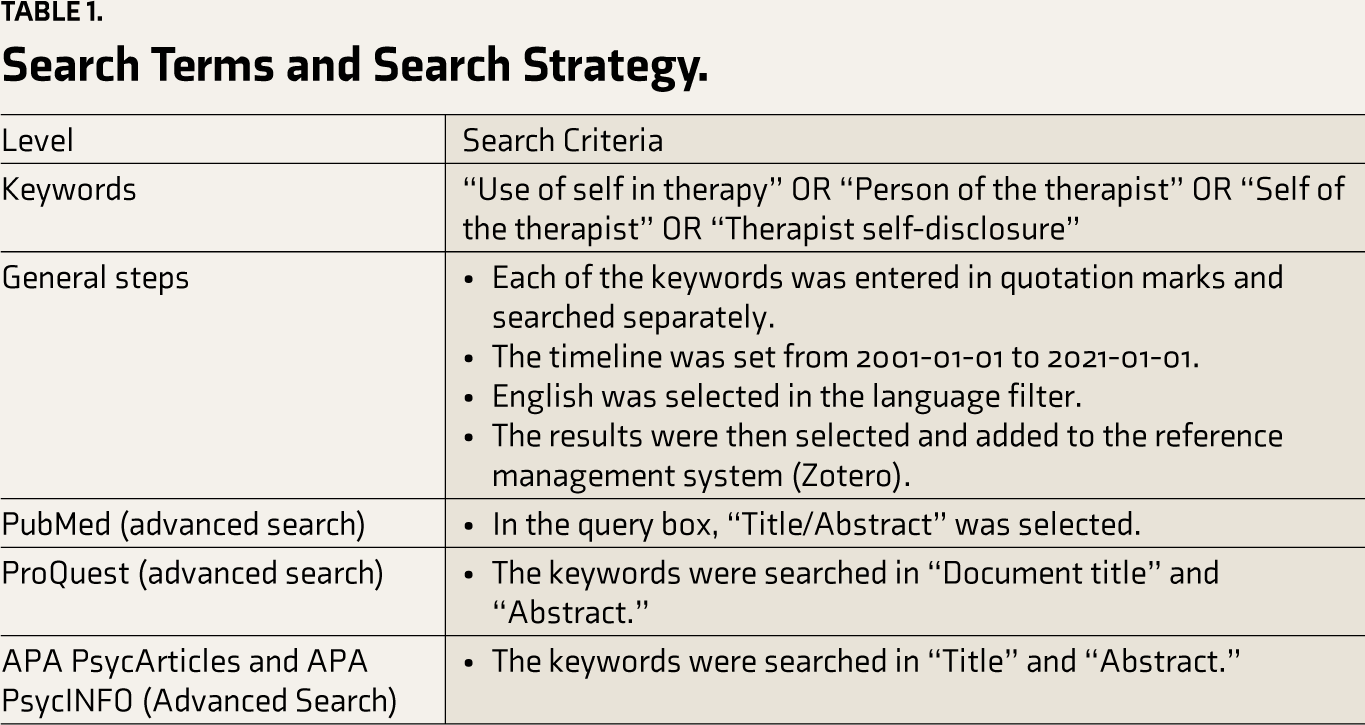
The review question was “How do therapists use their self in therapy?” and suitable keywords were identified. PRISMA guidelines were followed, 27 and databases such as PubMed, ProQuest, APA PsycArticles, and APA PsycINFO were used to search for journal articles. Full search terms can be found in Table 1.
Search Terms and Search Strategy.
Eligibility Criteria and Study Selection
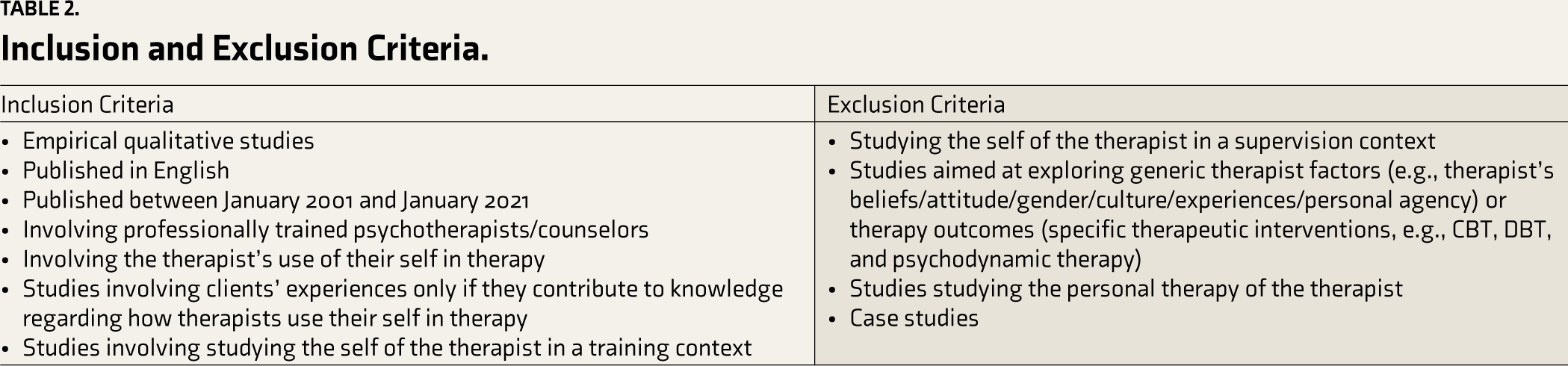
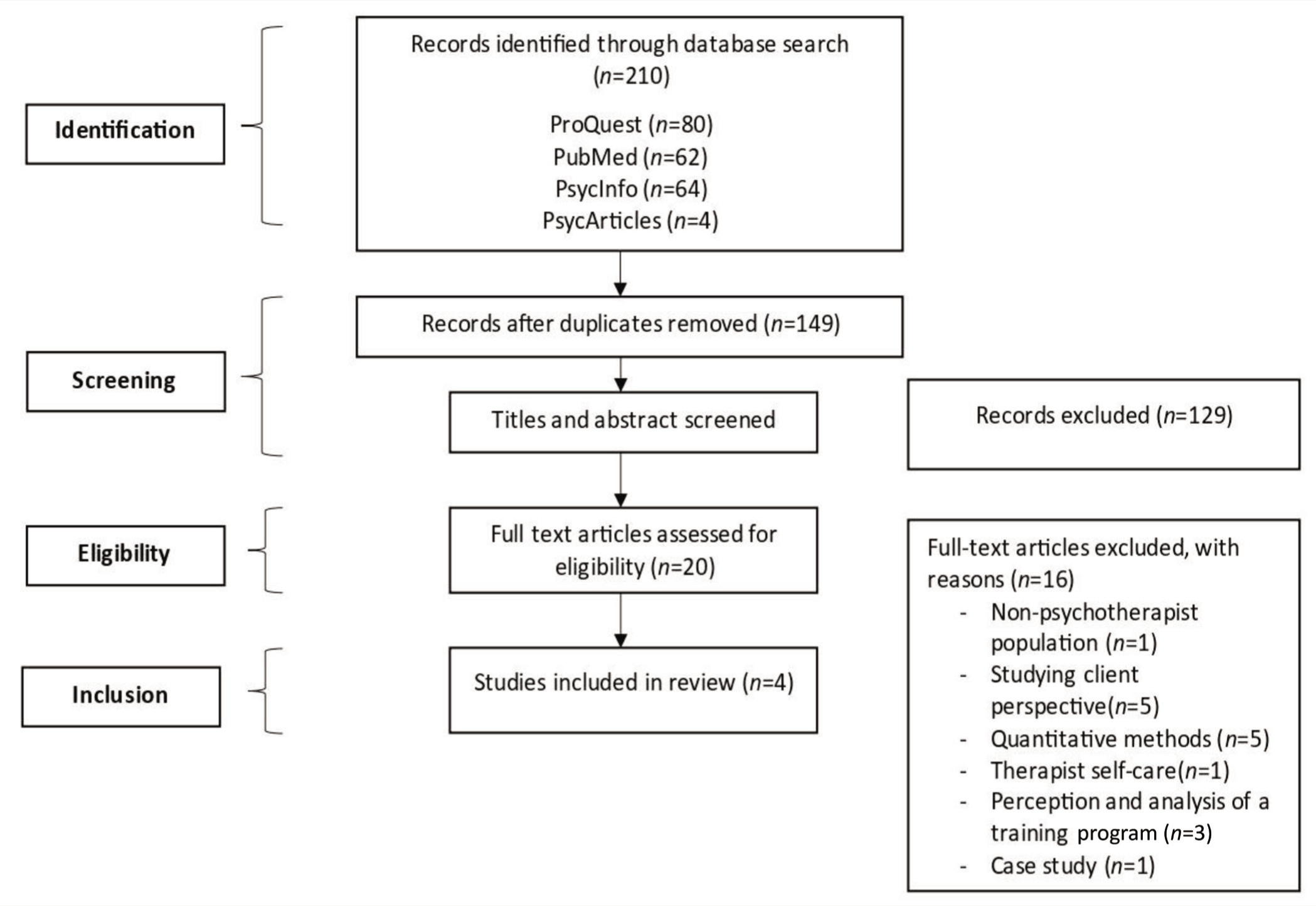
According to Wosket, the definition of self in therapy was described as the therapist’s active and intentional engagement of their personal qualities, experiences, and attributes in the therapeutic relationship to facilitate the client’s growth and healing. 26 Additionally, it involves the therapist’s ability to be self-reflective and self-aware and to use their emotional responses, thoughts, and behaviors in response to the client’s expressions and behaviors. 26 Qualitative studies focusing on using the therapist’s self and its link with the therapeutic process were selected. Full inclusion and exclusion criteria can be found in Table 2. The initial search led to 210 articles (details in Table 3). Abstracts and titles were screened for relevance by the lead author. From this, 20 articles were shortlisted for full-text screening by the lead author. Finally, four articles were included in the qualitative synthesis.
Inclusion and Exclusion Criteria.
Search Outcomes.

Articles were assessed for study quality using the “CASP checklist for qualitative research,” which is part of the Critical Appraisal Skills Programme (CASP). 28 The checklist includes 10 questions in three sections: Are the study’s results valid? (Section A) What are the results? (Section B) Will the results help locally? (Section C).
A second reviewer additionally screened all four articles. This inter-rater reliability returned 100% agreement on inclusion or exclusion. Any discrepancies during this process were resolved through discussion with the supervisor. Four articles were found to meet the inclusion criteria and were included in this systematic review. Figure 1 displays the PRISMA diagram of the search strategy.
PRISMA Flow Diagram.
Data Synthesis
Due to the inclusion criteria emphasizing qualitative methods, a narrative approach was utilized to synthesize the study findings. Common themes were identified across studies and are documented in the results.
Results
Description of the Included Studies
The final review included four qualitative studies. Data for three studies was from semi-structured interviews, with one coming from focus groups. Participants were all female in one study, not specified in two studies, and males and females in the last study (with the majority being male). Ethnicity was all Caucasian in two studies and not specified in the other two. All four were from the West: one from the USA, two from the UK, and one from New Zealand. Table 4 summarizes the characteristics of the included studies.
Study Characteristics.
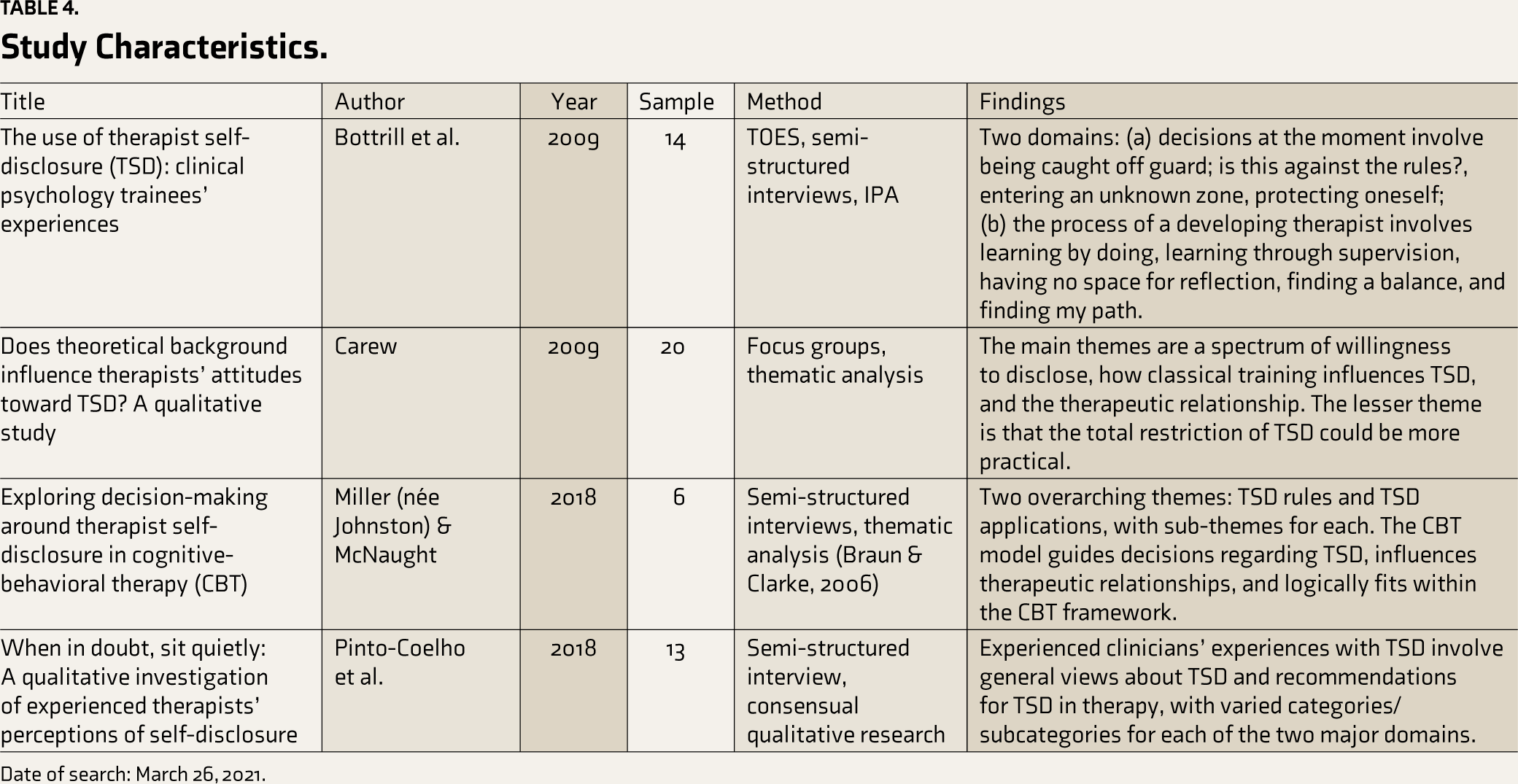
Date of search: March 26, 2021.
Quality of Studies
Using CASP, studies were of high quality, with no significant methodological flaws detected. They utilized appropriate study designs and data collection methods, and the qualitative analysis was well suited for the research question. However, it should be noted that the studies were predominantly from Western (high-income) countries, thereby limiting generalizability.
Themes
Across the four studies, a consistent theme that emerged in response to the research question was the exploration of therapist self-disclosure (TSD) as a means by which therapists use themselves in psychotherapy.
In order to gain a better understanding of TSD and how it is used in therapy, common themes were identified across the four studies.
The Nature of TSD
This section discusses the nature of TSD by understanding how it has been defined across the four studies, the types of instances where TSD is necessitated or initiated, and the types of TSD used by therapists.
Definitions of TSD
The selected studies cited various definitions of TSD. The most frequently cited definition in the four studies was by Hill and Knox, defining TSD as “statements that reveal something personal about therapists.” 8 The authors emphasize that TSD is a deliberate and purposeful act. This definition of TSD excludes unintentional and non-verbal forms of self-disclosure, such as self- disclosure by unintentional means—for instance, by details about a therapist’s marital status becoming apparent by their wearing (or not wearing) a wedding ring. While this definition was adopted by the majority of the studies insofar as it shaped their focus, the definition was not always shared with the participants. For instance, Carew’s study did not share any definition of TSD with participants during the data collection process, which allowed them to define it in their terms. 29 It did, however, include the Hill and Knox definition of TSD, 8 in its recruitment screening measure.
Types of TSD
In addition to the definition adopted, the studies focused on differentiating various forms of self-disclosure in therapy. These included differentiating between inescapable (e.g., physical appearance, such as skin color) and inadvertent (i.e., occurring in the context of transference-countertransference) forms of self-disclosure from deliberate TSD. Intentional, reasoned, and deliberate TSD were emphasized across studies. Studies differed in whether they included immediacy and self-involving statements as part of TSD, with a majority distinguishing self-involving statements from self-disclosing statements, except Bottrill et al.’s study. 30 Further, in some studies, TSD was explicitly seen as disclosing facts about the therapist and the therapist’s feelings.29,30
The Rationale for TSD
While most of the goals in the reviewed studies related to strengthening the therapeutic relationship, other purposes for engaging in TSD were also mentioned.
Strengthening the Therapeutic
Relationship
All studies referenced the role of TSD in building and maintaining a stronger therapeutic alliance and working relationship. TSD was seen as beneficial if it could result in a greater sense of collaboration, a sense of shared experiences and characteristics, helping overcome an impasse in therapy, reducing the power differential held by therapists in the therapeutic relationship.29-31 TSD was also seen as a means by which therapists could be perceived as more “human” by their clients, as hypothesized by Goldfried et al., 12 by highlighting a sense of similarity that enabled clients to relate more easily to the therapist. The role of TSD in fostering transparency in the therapeutic relationship was also highlighted.
Normalizing Client Experiences and Modeling Behavior
Across most of the studies, normalizing client experiences was seen as a recurring motive for intentional TSD in that it allowed clients to observe and learn that their thoughts, fears, and anxieties were not uncommon or abnormal and that the therapist had also experienced similar situations. Highlighting the universality or commonness of the client’s experiences through TSD could also provide reassurance and invite the client to continue exploring areas that they may feel hesitant to discuss freely. By taking an active role and offering information related to the self, TSD was also seen as modeling clients’ open communication, expressing their emotions, and inviting them to share openly.
Fostering Insight and Exploration
TSD was also viewed as promoting exploration of the client’s concerns and allowing for fostering insight across articles. It was seen as facilitating action or change, 31 opening up new avenues, and broadening therapy. Within cognitive-behavioral therapy, TSD was also used to challenge clients’ beliefs and assumptions sensitively. 32 Exploring the therapist’s situation was seen as offering clients an objective distance to reflect on their own experiences securely. 32
Influences on TSD
TSD was seen as influenced by different theoretical orientations and therapist factors. In addition, contextual factors were emphasized in the use of TSD.
Influence of Different Theoretical
Approaches on TSD
The four studies included therapists from different psychotherapeutic orientations trained in different modalities. One study by Carew explicitly examined the role of different theoretical orientations in therapists’ willingness to engage in TSD. 29 Findings related to this differed across studies. While Carew’s study suggested that classical psychodynamic training tended to reduce therapists’ willingness to engage in TSD, most experienced therapists in the Pinto-Coelho et al. sample were psychodynamically oriented and supported the view that TSD could be helpful in therapy. 31 TSD was seen as something to be cautiously approached in cognitive-behavioral orientations, promoted to the extent that it could be used as a tool of change and strengthened the therapeutic relationship.29,32 A spectrum of willingness to self-disclose, regardless of therapeutic orientations, including psychodynamic, systemic, person-centered, and cognitive-behavioral schools, was reported by Carew. 29
Different schools also appeared to impact the purposes for which TSD was used, with psychodynamic and humanistic-existential therapists using TSD to build rapport and trust with clients and cognitive-behavioral and integrative therapists using it to help clients better understand the therapeutic process or to challenge maladaptive thoughts and behaviors.29,32 Carew asserted that the total restriction of TSD is impractical. 29
Influence of Professional Stage and
Experience on TSD
Three out of the four studies had samples of experienced therapists, while one specifically studied the experiences of trainee therapists. Trainee therapists expressed various concerns about using TSD, including feeling that they were entering an unknown zone, worrying about protecting themselves, and having concerns about whether engaging in TSD was “against the rules” and feeling caught off guard. 30 Supervision was noted as potentially helpful in guiding beginner therapists regarding TSD use. 30 On the other hand, experienced therapists expressed a greater willingness to engage in TSD, 31 within a spectrum of willingness. 29 The use of TSD was seen as becoming more flexible and less guided by rigid rules as experience and time progressed. 31
Effective Use of TSD
All of the studies included directly or indirectly addressed whether the use of TSD was helpful or unhelpful, effective or ineffective, and how to determine which category it fell into. Further, they highlighted strategies, rules, and recommendations for effectively using TSD.
Effective Versus Ineffective Use of TSD
While one study explicitly compared helpful and unhelpful self-disclosures in the context of experienced therapists, other studies also featured therapists’ reports of whether they believed that specific instances of TSD were effective or unhelpful. A common subtheme herein was that TSD was/is ineffective when it shifts the focus away from the client, centers it on the therapist, and makes it difficult to re-center the focus on the client’s concerns.
Trainee therapists reported that unhelpful disclosures could adversely impact the boundaries of the therapeutic relationship and come back later in therapy to invite several more disclosures, whereas helpful ones involved minor disclosures that helped with the flow of therapy or with strengthening the therapeutic alliance. 30 Experienced therapists reported that unhelpful disclosures were met with impatience from clients, did not correctly identify the client’s emotions behind the experience, and did not result in increased emotional awareness for the client. 31 Consensus based on interviews with experienced CBT therapists was that effective use of TSD necessitated that TSD must have a clear purpose, must fit the client’s situation, must retain the maintenance of boundaries, and must be reflected on by the therapist post its use. 32
Interestingly, two studies found that there were often discrepancies between what was considered helpful or unhelpful TSD. The intentions and content of TSD across helpful and unhelpful TSD were often similar, focusing on aiming to normalize clients’ experiences and communicate the therapist’s understanding, with the content typically revolving around perceived similarities to the client’s experiences. 31 Regardless of whether TSD was seen as helpful or unhelpful, the primary metric behind this judgment was whether TSD was “in the service of the therapeutic relationship.” 29
Considerations for Effective Use of TSD
Miller and McNaught identified several factors that influence the decision-making process for TSD in cognitive-behavioral therapy, but this can be extended to all therapeutic approaches. 32 First, TSD should have a clear purpose and be utilized to help the client achieve meaningful change. Second, therapists must ensure that their self-disclosures are appropriate for the client and situation. This involves determining whether the TSD fits the therapeutic relationship, case conceptualization, and session goals. Lastly, therapists must prioritize maintaining boundaries and consider their well-being before disclosing personal information. 32
In addition to these factors, Pinto-Coelho and colleagues highlight other considerations for the effective use of TSD. 31 These include the therapist’s general attunement to the client’s dynamics, ability to gauge the client’s readiness, skill in managing countertransference, and ability to use a specific TSD appropriately.
TSD should be used cautiously, as it can have positive and negative effects on the therapeutic relationship and outcome. Therapists should carefully reflect on their use of TSD and seek supervision or consultation when in doubt. 31
TSD can be useful in psychotherapy when utilized appropriately and when considering the client’s needs and the therapeutic relationship. It is crucial for therapists to carefully reflect on the purpose and fit of the self-disclosure, maintain appropriate boundaries, and consider their well-being before deciding to disclose personal information. The therapist’s general attunement to the client’s dynamics, ability to gauge the client’s readiness, skill in managing countertransference, and ability to use a specific TSD appropriately are also important factors to consider in the decision-making process.
Discussion
The therapist’s self significantly influences psychotherapy through direct effects, impacting outcomes and shaping the therapeutic relationship. Therapists must actively cultivate and maintain their sense of self, recognizing its pivotal role in enhancing therapeutic interventions. 33 The intentional use of the therapist’s self is deemed crucial in building effective therapeutic relationships, often referred to as the “soul of therapy.” 34
Research on common factors in psychotherapy underscores the therapist’s self as a critical element transcending diagnostic boundaries and theoretical orientations. 35 Over the past two decades, a surge in literature has explored the deliberate use of the therapist’s self, acknowledging its renewed importance.10,25,34,36-41 This review systematically analyzed empirical studies on the intentional use of the therapist’s self, aiming to uncover diverse methods, processes, and considerations involved.
Investigating the therapist’s self poses significant methodological challenges due to the subjective nature of capturing and analyzing experiences that are difficult to measure quantitatively, such as emotional expression, countertransference, and therapeutic wisdom. Quantifying these complex processes using traditional measures proves challenging, necessitating innovative methodologies to capture the dynamic nature of self-of-the-therapist processes and their impact on therapy. The intricate interplay between therapist and client and the therapeutic relationship further complicates isolating specific effects solely to the therapist’s self. Developing and piloting novel methodological approaches becomes imperative to address these challenges and better understand the nuanced dynamics of the therapist’s self in psychotherapy.
This review highlighted the significantly limited availability of empirical qualitative studies on the use of the therapist’s self, in stark contrast to the abundance of theoretical and conceptual research on the use of the therapist’s self. 7 This raises important concerns regarding the potential gap between theoretical concepts and therapeutic practice. This dearth of empirical evidence may limit therapists’ ability to integrate themselves into the therapeutic process effectively and have important implications for their ability to engage in evidence-based practice. Additionally, empirical evidence may be needed to develop effective therapeutic training and supervision practices.
TSD emerged as the key aspect of the therapist’s use of their self in the present review, cutting across all four studies. While TSD is undoubtedly crucial in therapy, it is only one of many ways therapists can use their self in therapy. Other aspects may include empathy, 42 genuineness, 43 warmth, 42 creativity, 45 and therapeutic presence. 45 The therapeutic relationship is a complex and dynamic process, and therapists use various parts of themselves to help clients feel understood, accepted, and supported. Processes involving the therapist’s self also include therapist responsiveness, inner experience, interpersonal effectiveness, attachment, multicultural competence, expression and regulation of therapist affect, and therapeutic wisdom. 1 Other ways in which the self of the therapist can be involved in fostering a therapeutic relationship are through emotional expression, managing countertransference, and repairing alliance ruptures. 2 TSD is an important aspect of using the self in therapy in psychotherapy and outcome literature. 46
The studies included in the present review reflect a consensus on the utility of TSD across various theoretical orientations, consistent with contemporary and recent literature.7,12,19,22,47,48 Therapists perceive TSD as potentially beneficial in normalizing clients’ experiences, strengthening the therapeutic relationship, and promoting insight and exploration. The current review adds to the existing literature by highlighting the differential impact of theoretical orientation and developmental stage of therapists, with openness to TSD increasing with professional experience and greater openness of humanistic and relational psychotherapists to TSD. These findings suggest implications for training, emphasizing the need for explicit training and support to develop TSD skills for trainees. At the same time, experienced therapists may rely more on their intuition and judgment.
While the review’s findings suggest important avenues for using the self through TSD to benefit the therapy process, the current review highlights the need to integrate the diverse ways therapists use their self in the therapy process in empirical studies. Despite its close relation to the concept of TSD, no empirical studies on immediacy were found while surveying the literature for the present review. Defined by Kuutmann and Hinsenroth as “any discussion within the therapy session about the relationship between therapist and patient that occurs in the here-and-now, as well as any processing of what occurs in the here-and-now patient-therapist interaction,” it immediately offers another evidence-based pathway through which the self of the therapist can be used with beneficial clinical consequences. 46 (p.188) Further research is needed to explore these diverse aspects of the therapist’s self. The underrepresentation of other ways therapists use their self raises important questions about whether these need to be more studied, under-reported, or appropriately considered as the use of the self of the therapist.
Another important consideration when using TSD is cross-cultural factors. A majority of the existing literature on TSD reports studies from White or European American individuals and may not adequately address cross-cultural considerations. Constantine and Kwan offer a framework for examining these cross-cultural considerations and a clinical example of how TSD may play an important role while working with people of color. 49 In the context of cross-cultural therapy, TSD is seen as playing a role in reducing mistrust toward the therapist and promoting the therapist’s awareness and reflection, which may also promote the same for clients. 49
Based on the studies included in this review, TSD can be a helpful tool in how the therapist uses their self in psychotherapy when utilized appropriately and considering the client’s needs and the therapeutic relationship. The review’s strengths lie in its thematic focus, which allowed an analysis of the various ways therapists use themselves in therapy and identified gaps in current literature. Adopting a qualitative systematic review also allowed for an in-depth analysis of the narratives of therapists and their personal experiences in the use of their self. However, the study was limited by the databases searched and the highly specific phrases and keywords searched, which may have inadvertently led to the exclusion of articles that are relevant to the review but may have yet to use the keywords that the review specified. Further, the review’s findings must be interpreted with the recognition that it focused exclusively on qualitative studies. Consequently, several empirical quantitative studies found during the screening stage were excluded.
In conclusion, this systematic review sheds light on the limited empirical research on the intentional use of the therapist’s self in psychotherapy. It highlights that TSD is a key means by which therapists use their self. The findings emphasize the need for more empirical research exploring diverse aspects of the therapist’s self and cross-cultural considerations. Developing a culturally valid framework and consensus on training and practice guidelines can enhance evidence-based practices grounded in diverse perspectives. Future research should address these gaps to deepen the understanding of the therapist’s self and its implications for psychotherapy outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical approval was not sought since this is a review and no primary data was involved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Patient consent was not required since no primary data is involved.