
Abstract

Acatatonic illness that develops due to a general medical ailment is called organic or secondary catatonia. 1 An estimated 20%–40% of catatonias are thought to have organic etiologies. 1 If the lorazepam trial is unsuccessful, electroconvulsive therapy (ECT) is recommended by guidelines. 2 A few studies in the past have used memantine where lorazepam has failed.3,4 Also, studies have used memantine augmentation in lorazepam therapy. 5 γ-Aminobutyric acid (GABA)-A is dysregulated by N-methyl-D-aspartate (NMDA) hyperactivity, and NMDA antagonists probably can restore GABA-A function in the frontal lobes. 6 Glutamate hyperactivity in the posterior parietal lobe likely causes symptoms like posturing. 6 Here, we describe five cases of organic catatonia in a general hospital who did not respond to lorazepam but responded to memantine.
Case Series
According to the Diagnostic and Statistical Manual, Fifth Edition (DSM-5), 7 all of them had a diagnosis of catatonia due to another medical condition, and their clinical data is summarized below and in Table 1. They were assessed using the Bush Francis Catatonia Rating Scale (BFCRS) 8 before and after treatment. There was no significant family history or any history of mood, psychotic, or anxiety disorders. They lacked emotional reaction and facial expressiveness. Following a failed lorazepam trial as per guidelines, 2 lorazepam was stopped, and memantine (20–30 mg) was tried in all the patients. The BFCRS score changed throughout the treatment, showing that all patients recovered significantly with memantine without experiencing any reportable adverse effects. The mental status examination after recovery from catatonia and during the follow-up did not reveal any significant findings except in case C. Written informed consent was obtained in the patient’s vernacular language after complete improvement of catatonia.
Case A
A 64-year-old male with nicotine dependence and abstinence for the past 15 years presented with an abrupt onset of unconsciousness for three hours and, over the first day of hospitalization, regained consciousness with right hemiparesis without facial involvement. His blood pressure was 180/100 mm Hg, total cholesterol was 300 mg/dl, triglyceride was 350 mg/dl, and non-contrast computed tomography (NCCT) of the brain showed a hemorrhagic stroke in the left basal ganglia region (Figure 1). Aspirin 75 mg, clopidogrel 75 mg, and telmisartan 40 mg were stopped, which he was already on, and he was started on mannitol 20%–350 ml stat, three times a day, labetalol 40 mg intravenous stat, amlodipine 5 mg twice daily, rosuvastatin 40 mg stat and HS, and Ringer lactate slowly on the first day itself. From the evening of the second day of admission, he was noted to have suddenly ceased eating, with a marked decrease in social engagement, decreased movement, prolonged looking skyward in one direction, and lying down immobile in one position. On mental status examination, he had immobility, mutism, staring, posturing, negativism, waxy flexibility, withdrawal, and automatic obedience. No improvement was observed with intramuscular lorazepam (4 mg on day one, 14 mg on day two, and 10 mg on day three).
Treatment Course with Memantine and Follow-up of Included Patients.
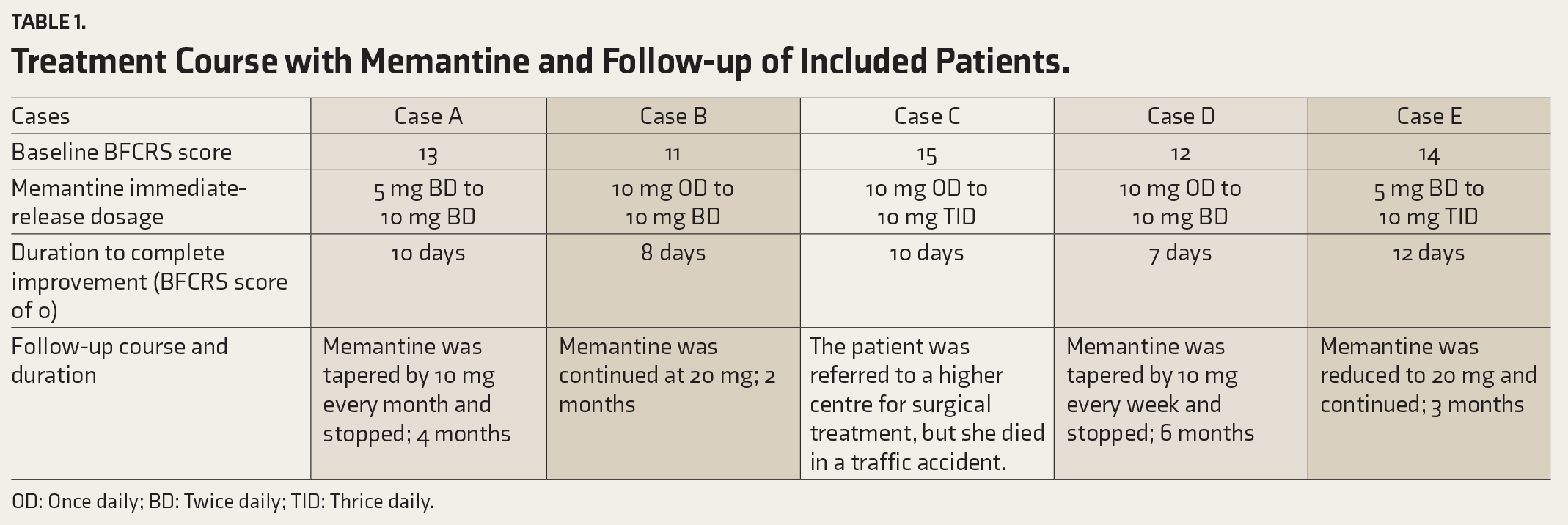
OD: Once daily; BD: Twice daily; TID: Thrice daily.
Non-Contrast Computed Tomography (NCCT) of Brain Showing Hemorrhagic Stroke.

Case B
A 71-year-old male diagnosed with idiopathic Parkinson’s disease for two years and maintaining well on pramipexole 4.5 mg presented with the acute onset of high-grade fever, spasmodic pain in the lower abdomen, dysuria, and frequent micturition for three days without any worsening of parkinsonian symptoms. His total leukocyte count was 16,000/mm 3 ; urine culture revealed Escherichia coli; the c-reactive protein was 60; and the erythrocyte sedimentation rate was 50 in the first hour. He was diagnosed with a urinary tract infection. He was started on intravenous amikacin 500 mg twice daily, flavoxate 100 mg thrice daily, and paracetamol 650 mg SOS for fever. On the third day of admission, he was noticed to have reduced body movements, food intake, and interaction with family members; he was looking in one direction for an extended period and grimacing. On mental status examination, he had immobility, mutism, staring, grimacing, negativism, and withdrawal. No improvement was observed with intramuscular lorazepam (6 mg on day one, 16 mg on day two, and 10 mg on day three).
Case C
A 65-year-old female presented with an abrupt onset and continuous decrease in social interaction, food intake, and body movements for one day. There was a history of dull, aching headaches that were relieved with paracetamol for the past six months. Her NCCT brain showed frontal meningioma with a mass effect and edema in the left frontal lobe (Figure 2). She was started on mannitol infusion (20%, 100 ml) thrice daily and Ryles tube feeding. On mental status examination, she had immobility, mutism, posturing, negativism, waxy flexibility, withdrawal, and automatic obedience. No improvement was observed with intramuscular lorazepam (8 mg on day one, 12 mg on day two, and 10 mg on day three). On day three, BFCRS increased to 15, and catatonia worsened with staring and stereotypy.
Non-Contrast Computed Tomography (NCCT) of Brain Showing Meningioma.

Case D
A 62-year-old male presented with an abrupt onset of high-grade fever and arthralgia without any rash for around seven days, followed by an abrupt onset of decreased mobility, lying down still in one posture, a marked reduction in food intake, staring upward in one direction for extended periods, and a significant decrease in interaction, which started two days prior to presentation. His Chikungunya IgM was positive, the c-reactive protein was 45, and the erythrocyte sedimentation rate was 30 in the first hour. He was started on Ryles tube feeding, intravenous infusion with normal saline and Ringer lactate, and paracetamol infusion for fever. On mental status examination, he had immobility, mutism, staring, posturing, negativism, stereotypy, withdrawal, and automatic obedience. No improvement was observed with intramuscular lorazepam (6 mg on day one, 10 mg on day two, and 14 mg on day three).
Case E
A 75-year-old female with hypertension and diabetes mellitus for 25 years presented with acute-onset left-sided chest pain, dyspnea, dizziness, and diaphoresis for around two hours. While she was being evaluated in the emergency treatment room, her pulse and blood pressure were not recordable during the regular monitoring, and cardio-pulmonary resuscitation and dopamine infusion were initiated, following which her pulse and blood pressure were recordable. The patient’s reduced food intake, social engagement, and range of motion were noted the day after she was admitted to the hospital. Her electrocardiogram showed anterior wall myocardial infarction, troponin I was positive, total cholesterol was 250 mg/dl, low-density lipoprotein was 250 mg/dl, and triglyceride was 300 mg/dl. She was started on enoxaparin 60 mg subcutaneous stat and once daily (aspirin 75 mg + clopidogrel 75 mg)—four tablets stat and one tablet daily; sorbitrate 5 mg stat; nitroglycerin 2.6 mg twice daily; rosuvastatin 40 mg stat and daily; and ramipril 2.6 mg once daily. On mental status examination, she had immobility, mutism, negativism, withdrawal, automatic submission, passive obedience, and grasp reflexes. After three hours, no improvement was seen with 4 mg intramuscular lorazepam and 4 mg intravenous lorazepam. After a 12-hour break, another intramuscular lorazepam, 2 mg, was administered due to the patient’s extreme drowsiness, without any improvement.
Discussion
Catatonia-like symptoms may be caused by excess glutamate and glutamate receptor hyperactivity in the parietal brain, as well as by NMDA hyperactivity, which indirectly affects GABA-A function in the frontal lobe. 6 Also, a decrease in psychomotor activity and a catatonia-like phenomenon have been observed in the background of the rise of pro-inflammatory markers. 9 Increased brain glutamate levels and a rise in pro-inflammatory markers have been observed hours after a hemorrhagic stroke, which can explain catatonia in case A. 10 Lesions in the frontal lobe and the resulting neurotransmitter dysfunction and disrupted connections with the parietal lobe and subcortex have been observed in catatonia, which can explain the symptoms in case C. 8 Infection-related catatonia has been reported; this is most likely the result of increased inflammatory markers and subsequent NMDA hyperactivity, which explains the symptoms in cases B and D.1,9,11 Myocardial infarction has been reported to cause cerebral hypoxia and ischemic injury, which in turn can result in a rise in pro-inflammatory markers. 12 This can result in catatonia due to glutamate excitotoxicity, which can explain the symptoms in case E. 3
Memantine may improve catatonia by inhibiting NMDA receptors, which reduces aberrant glutaminergic transmission. 13 This aberrant glutaminergic transmission includes increased glutamate activity due to allosterically opening NMDA receptors and increased extracellular glutamate. 13 Additionally, memantine has been demonstrated to lessen oxidative stress brought on by inflammation, thus reducing neurotoxicity. 14 Amantadine, which has an NMDA antagonism mechanism similar to memantine, has helped treat refractory catatonia. 13 NMDA receptor hyperactivity is associated with lorazepam resistance; memantine and amantadine can be helpful in such cases. In our cases, the improvement of catatonia may be due to these processes.13,14 Only a few studies in the past used memantine in catatonia after discontinuing lorazepam due to non-response. One study in the past used memantine 20–25 mg for catatonia following stroke, which is similar to our case A, where 20 mg of memantine was used. 3 Another case series used memantine 20–30 mg for catatonia secondary to infection, which is similar to case B, where 20 mg of memantine was used. 11 Memantine has been similarly used with 10–20 mg dosage for treating catatonia associated with schizophrenia and depression, where lorazepam failed. 15
Acute onset, a shorter duration of catatonic symptoms, the presence of secondary or organic factors, and being elderly may have predicted an excellent response to memantine. Infrastructure problems restricted the use of ECT in our cases, along with patient family members’ reluctance to be referred to a higher facility, the possibility of elevated intracranial pressure in cases A and C, and a recent myocardial infarction. Besides, there was non-response to lorazepam and sedation in case E, which restricted its use, which prompted us to try memantine in our cases. This study’s observational design, lack of a control group, and comparison with conventional treatment are the limitations.
Conclusion
Memantine may be an effective treatment for organic catatonia in elderly patients when lorazepam has failed, and ECT options are limited.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained in the patient’s vernacular language after complete improvement of catatonia.