
Abstract
The Mental Health Care Act 2017 (MHCA) of India places restrictions on the use of electroconvulsive therapy (ECT) in minors (persons less than 18 years of age). However, it also recognizes that treating psychiatrists may recommend ECT under specific clinical conditions. In such cases, it is mandatory to have the informed consent of the minor’s legal guardian and prior permission from a Mental Health Review Board (MHRB). While the regulations on the use of ECT are essentially intended to prevent irrational practice, there has been concern among clinicians about possible delays in MHRB approvals, or even disapproval, that may impede treatment of serious conditions such as suicidal risk and catatonia. 1 The MHCA does not give the clinician any discretionary powers for using ECT in minors. 2 These concerns could be addressed with more explicit guidelines on the processes to be followed by the clinician and MHRB.
This article brings together the evidence and support for ECT in child and adolescent psychiatry. We look at published empirical literature on the use of ECT in minors, recommendations from international guidelines, as well as clinical experience at our center before and after the MHCA. Informed by this triangulation, we put forth recommendations for a conducive alignment of clinical practice with the MHCA.
This article involves a review of literature and clinical case series that did not require approval of the Institutional Ethics Committee at the National Institute of Mental Health and Neurosciences, Bengaluru, India. Individual patient consent has not been taken since the case series did not involve detailed case descriptions, rather only specific de-identified clinical data.
Empirical Evidence for the Safety and Efficacy of ECT in Minors
ECT has been used in minors for more than five decades.3,4 Evidence for the safety and efficacy in affective and psychotic disorders, especially for clinical presentations like catatonia and suicidality, has grown.5–7 Safety concerns with the use of ECT in minors have been empirically examined. No long-term impact on cognitive abilities has been found. 8 On the contrary, ECT used timely for the treatment of mental illnesses may have neurorestorative properties. 9
Several centers worldwide have reported on the safety and use of ECT in minors. Puffer et al. 10 reported their center’s experience over the 20 years, between 1991 and 2013. Fifty-one adolescents, with a mean age of around 16 years, were treated with ECT for a primary mood, psychotic or catatonic condition. Bitemporal ECT given over a mean of nine sessions resulted in a 77% rate of clinically significant improvement. They recorded that young people may commonly have a prolonged seizure duration; however, this declined with age over adolescence. A Swedish report published last year 11 reported ECT use data over five years (2012–2016) in young people (age <19 years) in the country’s National Patient Register. Over that period, 118 individuals (~20% were less than 16 years old) received ECT in all of Sweden. The commonest indications for ECT were depression with or without psychotic symptoms, psychosis, mania, and catatonia. A majority of patients had failed multiple previous treatments, indicating a degree of treatment resistance. Right unilateral ECT for a mean of seven sessions was used. Fifty-seven percent of patients responded adequately, with better response rates for depression. Adverse effects reported in 25% of patients were minor, the commonest being headache and subjective memory impairment.
Clinical Reports from India
The first systematic report from India on the utility of ECT in children and adolescents came around a decade ago when Grover et al reported on 25 patients below the age of 18 years who received ECT. 12 These were almost 6% of the total number of patients receiving ECT over a span of 12 years. The mean age was around 16 years, and more than 60% were male. The commonest diagnoses included schizophrenia (56%) and depression (12%), with the commonest indication for ECT being catatonia (68%). After a mean no. of 10 ECTs, the overall response rate was 76%, and half the patients had >/=85% symptom resolution. Headache, nausea/vomiting, and prolonged seizures were the most typical adverse effects seen in less than 10% of patients each. In a more recent report 13 from the same group, over a 7-year study period (2012–2018), 51 individuals up to 19 years of age received ECT. These formed around 4% of the total patient population receiving ECT in the said period. Schizophrenia, depressive disorder, and mania were the most common diagnoses. ECT was chosen considering inadequate response to medication (70%) and long duration of illness with a need for early response (58%). A mean of 8 ECTs resulted in significant clinical improvement (≥50%) in 86% of patients, with the highest response magnitude for catatonia and mania.
A report from our center covered the practice of ECT over 10 years (2002–2012) in children younger than 16 years of age. 1 Twenty-two children, with a mean age of 14 years, received ECT at our center over these 10 years. The youngest child was 10 years old. Affective and non-affective psychoses formed the commonest disorder groups, with catatonic features in more than 50%. The most frequent indications for ECT were the need for quick recovery (when there was a high risk to self or a prolonged illness) and an augmentation strategy where there was an inadequate response to medication and other treatment modalities. The commonest side effect, recorded in close to 35% of patients, was prolonged seizure; other minor side effects were headache and subjective memory impairment. Most patients received less than nine ECT sessions, after which clinically significant response was achieved in >75%.
A qualitative study that explored parental experiences of their child receiving ECT 14 reported that despite initial apprehensions about the utility and efficacy of ECT, parents found ECT to have had a beneficial role in symptom control. Parents felt that when medications were not helping, the choice of ECT was in line with the patient’s welfare and that they would recommend the same to other parents in a similar situation.
All these clinic-based reports from India and elsewhere suggest ECT to be a safe, efficacious, and acceptable modality for psychiatric illnesses in youth.
International Guidelines for the Use of ECT in Young People/Minors
We reviewed the latest guidelines15–20 for treating various child and adolescent psychiatric conditions that list the therapeutic indications and role of ECT (Suppl Table 1). There are several points of concurrence across guidelines:
The general clinical indication for ECT in minors is the presence of severe illness, life-threatening symptoms, or when symptoms have not responded to other adequate treatment trials. Among diagnostic categories, ECT is uniformly recommended for mood disorders and catatonia. There is a need to monitor cognitive functioning before and after treatment sessions.
Use of ECT in Minors Over the First Six Months (August 2022–February 2023) Since the Constitution of the MHRB at Our Center
ECT has been used in minors at our center for several years now. 1 After the implementation of the MHCA, we reworked the procedure of facilitating the use of ECT in minors. Suppl Table 2 lists 10 cases in which ECT was used after the constitution of the MHRB. Most children were 16–17 years old; however, three were young adolescents 14 years of age. The commonest (>80%) clinical profile was characterized as an older adolescent (16–17 years of age) girl with a mood disorder, severe symptoms, and high risk to self, with poor response to multiple medications in the past. These were all inpatients. Suppl Table 2 lists the past and current medication treatments.
In each case, a written summary was submitted to the MHRB, and permission was sought after seeking informed consent from the child’s primary caregivers, usually the parents. The MHRB responded within a few days without any inordinate delay or objections. Permission for ECT was not denied in any case.
Between 6 and 14 ECT sessions were conducted, with generally bifrontal electrode placement. They tolerated the treatment well, with minor side effects that recovered after stopping the ECT sessions. A Clinical Global Impression—Improvement rating of 1 or 2, that is, very much improved or much improved, respectively, was recorded for a majority (8 out of 10) of the adolescents.
Recommendations for Aligning Clinical Practice with the MHCA
The recommendations below are informed by empirical literature on the efficacy of ECT in minors, international clinical practice guidelines, as well as clinical experience at the Department of Child & Adolescent Psychiatry, NIMHANS, Bengaluru. The recommendations, listed in Table 1, are divided into two sections. The first section details clinical indications under which ECT may be recommended to treat minor psychiatric patients. The second section makes recommendations for review processes to be undertaken by the MHRB.
Criteria for Selecting ECT in the Clinical Care of Minors.
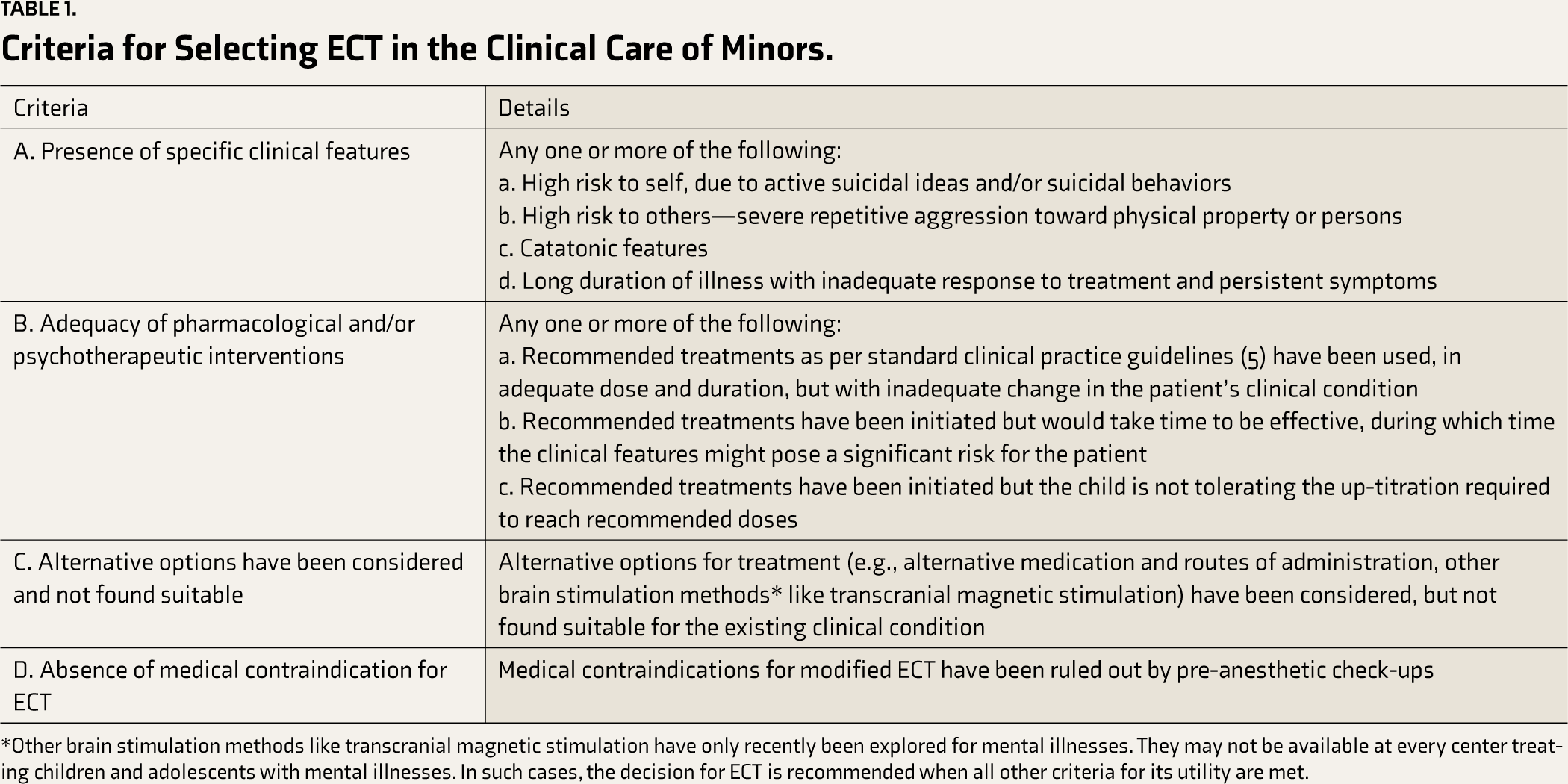
*Other brain stimulation methods like transcranial magnetic stimulation have only recently been explored for mental illnesses. They may not be available at every center treating children and adolescents with mental illnesses. In such cases, the decision for ECT is recommended when all other criteria for its utility are met.
Section 1: Recommendations for Clinical Indications for the Use of ECT in Minors
ECT can be used in children and adolescents safely. Its use is primarily to achieve rapid and short-term improvement of severe symptoms. Commonest diagnostic indications for ECT include—mood disorders (major depressive disorder, mania, mixed affective state), Psychotic disorders (including schizophrenia, schizoaffective disorder, psychosis not otherwise specified, acute and transient psychotic disorder), and catatonia; mental disorders due to medical conditions (including delirium), and certain medical disorders (neuroleptic malignant syndrome, intractable seizures) have also been described in the literature.15–18,21 ECT can be used in any of these diagnostic conditions when criteria A–D, presented in Table 1, are fulfilled.
It is to be noted that ECT is sometimes recommended for indications like self-injurious/aggressive behavior in children/adolescents with neurodevelopmental disorders. In such cases, the recommendation for ECT may be considered on a case-by-case basis, considering the clinical scenario, including risk to self/others, response to alternate treatments, and risk/benefit ratio, considering the limited evidence for ECT for such indications.
Section 2: Recommendations for the Review Process by the MHRB
The treating psychiatrist must submit the following documents to the MHRB:
A clinical summary of the patient. Documentation detailing criteria under Section 1. In case of urgent, life-threatening indications for ECT, the urgency must be clearly documented in the requisition by the treating psychiatrist. Informed consent form signed by the parent/legal guardian: The informed consent process must reflect a detailed discussion of the clinical indication of ECT and consideration of other treatment options.
Subsequent steps should occur within consecutive single working day periods:
Upon receiving an email requisition from the treating psychiatrist, the MHRB could forward the documents to all its members. The MHRB members could raise their objections, if any, via email. If no objections are raised, the MHRB could proceed to permit ECT, which should be communicated to the treating psychiatrist directly via email.
If any MHRB member/s raises any objections, the same must be communicated to the treating psychiatrist immediately, and one of the following courses may be taken:
The treating psychiatrist can address the query/concern raised satisfactorily, and the MHRB proceeds to permit ECT. The MHRB may seek the clinical opinion of another psychiatrist regarding the suitability of ECT for the minor patient. This may involve either a review of the submitted documents, an independent evaluation of the patient, or both. This evaluation may be conducted either in person or through electronic mode. The MHRB may convene a board meeting with the treating psychiatrist for an online or in-person discussion, whichever can be organized without delay, to facilitate a consensus decision.
Communication could be over electronic mail wherever feasible for all the above processes. Hard copies of all documents must be processed in parallel. Clinical and MHRB communication records must be maintained with the treating psychiatrist and the MHRB.
Conclusions
There has been concern among psychiatrists about the practice of ECT in minors in the context of the MHCA regulations. The above recommendations, which are based upon a triangulation of empirical evidence, international guidelines, and our practice, are intended to aid clinical practice to promote the safe and effective use of ECT in minors. They explicitly list criteria for clinical decision-making regarding the selection of ECT in a particular case, describe the overall process and timeline to be followed by the treating psychiatrist and MHRB, list different possible scenarios that may come up in the MHRB’s consideration of a particular case and how they may be handled urgently.
Psychiatrists treating children and adolescents should be aware of the literature on ECT. This is essential for practice decisions and to engage families better in the treatment process. The family’s awareness of legal regulations around ECT may elicit additional concerns for the young person. In the future, we need to evolve ethical and scientifically rigorous mechanisms to enable empirical research on ECT use in minors, such that the clinical recommendations can be better informed and questions such as the long-term effects of ECT on the developing brain can be comprehensively addressed.
Supplemental Material
The supplemental material for this article is available online.
Supplemental Material
The Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.