
Abstract

To the editor,
Delusional Parasitosis (DP), also known as Ekbom’s syndrome, is characterized by the patient’s fixed and firm belief that his or her skin, body, or immediate environment is infested by small, living (or less often inanimate) pathogens despite the lack of medical evidence for this. 1 DP can manifest as a shared psychotic disorder, affecting commonly the spouse–“folie a deux” 2 or “folie a famille,” where other family members share the same delusion. We are reporting a case of DP (by leech) in a female.
The Case
RT, 29-year-old Nepali married female, is a resident of a village in the Darjeeling district. She and her husband are agricultural day laborers. It was a rainy season. RT and her husband were ploughing paddy seed plants in a field. RT was planting the paddy seed plants in a squatting position, partly submerged in water. She suddenly felt a sensation of something slowly moving inside her vagina. She spotted a few leeches crawling close to her feet and shouted for help. The husband and other laborers in the field rushed in. She said a leech had entered her stomach through the vagina. All others endorsed this possibility as few leeches were seen in the muddy water. Her husband collected a leech in a pot. Rescued to home, she complained of shifting pain in the abdomen, as if the leech was moving inside. That evening they consulted a local faith healer (Jhakri) who gave some herbal root preparation to swallow with hot water, which would kill the leech. But the next day her discomfort increased with loss of appetite and vomiting tendencies and increased itching and frightening crawling sensation over the abdomen. They then consulted a priest (Tantrik) who said that the leech had entered deep inside the abdomen and may need surgical intervention. After three days of suffering, they went to the local government health facility, and the doctor referred her to a gynecologist in a nearby town. They visited the gynecologist, who did a Per Vagina (P/V) examination, discarded the leech invasion claim, and prescribed tablet Diazepam 5 mg tablet once daily. She continued to suffer from loss of appetite and vomiting spells, shifting abdominal pain and nausea, and heightened anxiety and fear of alleged internal blood loss (sucking by the leech). They consulted another religious faith healer, who chanted holy water to drink three times daily to expel the leech but got no result. Then after four weeks, they came to a private clinic.
On examination, she complained of sharp pain traversing from the left to the right side of her abdomen, radiating down to the pubic area. She said she could feel the movement of the leech inside and showed the directions of the leech movement (Figure 1). She felt an itching pain over the abdomen along the path of the leech. Some scratch marks were visible on the lower abdomen. She also complained of a burning sensation in the abdomen along with a sensation of being bitten inside and a crawling or prickling sensation in different areas of the abdomen. She also complained of poor sleep since the infestation. Her husband showed a leech in a bottle. He said that she checks and rechecks her vaginal passage for the presence of leech several times daily. He firmly believed that the leech was still inside her, in spite of the gynecologist’s opinion of “no leech inside” on their first visit. Obviously, his delusional belief was further strengthened by local myths and cultural anecdotes in the community relating to vaginal leech infestation. He strongly believed that a leech could survive inside the human abdomen. He also said that he had heard about three incidents of similar leech invasion through the vagina a few years ago in their farming community. Her mood was a mixture of predominantly anxious feelings and felt sad, especially because of the imagined physical danger due to this unresolved infestation. She feared that the leech may suck all her blood and damage her internal organs and that eventually, she may die.
Patient Showing the Path of Leech Crawling Inside the Abdomen.
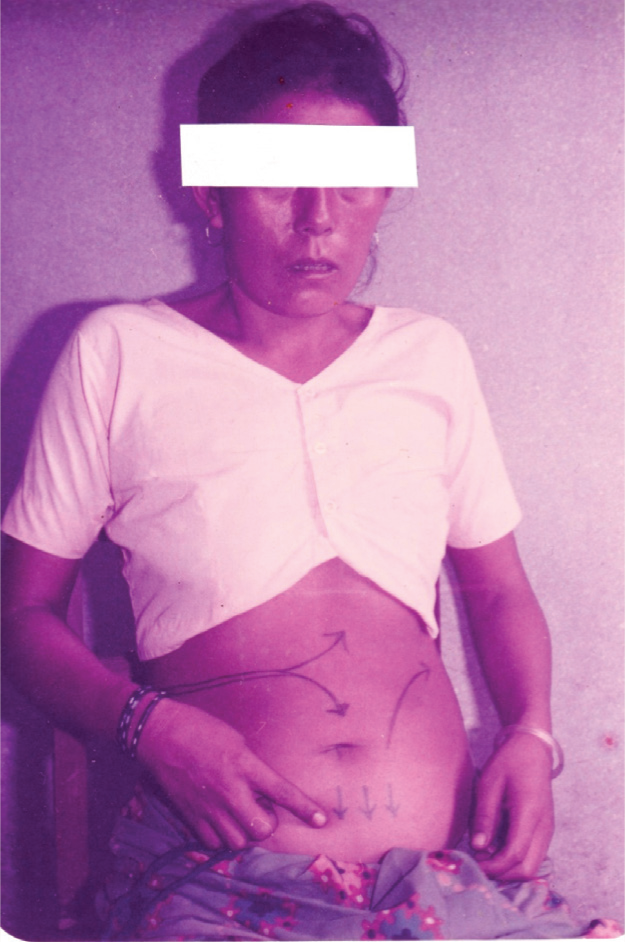
She was examined by a medical specialist and a gynecologist immediately and was uneventful. The inner vulva area had some bruises due to repeated fingering in attempts to catch the leech. No mark of leech bite was found in any parts of the body. A mental state examination revealed her mood was a mixture of predominantly anxious and depressed, and fearful look with depressed affect. She had a firm conviction of leech infestation through the vagina with some acting-out repetitive body-focused behavior (like a reactive obsessive-compulsive behavior of repeated checking and rechecking of vaginal passage) and tactile hallucinatory sensation all over the abdomen along the path of alleged leech movement inside. No other psychiatric symptoms were noted or reported. No history of any drug or alcohol abuse was present. Laboratory examination of whole blood, routine biochemical tests and X-ray abdomen came within the normal range. Ultra-sonogram (USG) abdomen was not done due to the non-availability of this procedure.
Given the firm unshakable belief of leech infestation of both RT and her husband, she was diagnosed with Primary Delusional Parasitosis with Folie a deux (ICD 10 –F22/ F24). Moreover, as they acknowledged similar incidents and beliefs in their farming Nepali community culture, this clinical presentation may be regarded as an example of a cultural variant of Ekbom’s Syndrome.
She has been treated with tablet Risperidone 1 mg twice daily for a week and then 2 mg twice daily, along with tablet Clonazepam 0.25 mg at bedtime. Six weeks of follow-up showed a remarkable improvement. Her belief in leech infestation was still there. However, she acknowledged the effects of the medication in that she felt easier, had no abdominal cramps or feeling of intra-abdominal leech movement, and believed with 90% certainty that the “leech was killed and expelled through stool.” Her husband also endorsed that. A further follow-up at three months showed no residual symptoms.
Discussion
DP patients typically report parasites in or on the skin and, around or located inside body openings or in the internal organs, and high anxiety. Patients usually present an exhibit of skin or clothing debris in plastic or matchboxes as proof of the infestation (matchbox sign). 3 The most commonly reported pathogens are insects (84%), worms (14%), bacteria (2%), and fungi (1%). 4 The common locations of infestation are the skin of the hands and legs, back, feet, scalp, and genitals or body orifices like the nose, ears, mouth, or anus, or the gastrointestinal tract, 5 but the vaginal entry of alleged infestation is not reported to date. This is probably the first reporting of alleged leech infestation in DP in the literature.
Cultural belief systems may play a pivotal role in the pathogenesis of DP. 6 Some Indian researchers have stressed the influence of Hindu cultural beliefs in the development of DP. They discussed the perceived vulnerability of the body orifices such as ears, eyes, mouth, and anal and urethral orifices in developing DP in Indian patients. 7 Immediate environmental factors are usually implicated in DP as the source of the offending organism like particular dress or cosmetics, furniture, house, carpets, automobile, another person, plants, garden vegetation, pets like cats or dogs, or other animals. Here the rural agricultural working landscape with visible leeches acted as the triggering factor on which the delusional thought crystallized with similar beliefs of the family and the community. Here, the patient and her husband narrated their firm conviction about vaginal vulnerability as they have similar information from their local Nepali community. They stressed the vulnerability of body orifices to the invasion of external objects like flies, bees, insects, wasps and lice, and even bad air (cursed or charmed by a malevolent spirit or evil person). This folk concept of “pathogenic intrusion” through body orifices was also supported by the local healers and both the patient and her husband cited local village faith healers or Jhakri who specialize in driving out foreign objects (animate or inanimate) from body, ear or eyes.
Vulnerable Vagina
Braun and Wilkinson 8 in their elegant analysis of socio-cultural construction of the vagina pointed out at least seven persistent negative representations of the vagina that has implications for women’s health and wellbeing. Two social constructs, particularly “vagina as vulnerable and abused” and “vagina as dangerous” have some relevance in the present context. The psychological and physical vulnerability of females has been stressed in many psychoanalytical works. Shaw 9 thus stated that “Women may have fears and fantasies about their genitals as damaged, and likely to be hurt, and may experience a sense of genital vulnerability.” Horney 10 discussed the “fear of vaginal injury.” In the contemporary social milieu, Erikson 11 stated, “Dreams, myths and cults attest to the fact that the vagina has and retains (for both sexes) connotations of a devouring mouth.” Vulnerability of the vagina in different forms and content is a critical socio-cultural construct in every culture, especially in menstruation, childbirth, rape and abuse, and in this case, DP. Genital focus in DP is comparatively rare—only two male reports are available, one patient had a tactile hallucination, and complained of insects crawling into his genitals 12 and the other spent a few years “digging worms out of his scrotum with razor” with intermittent blood loss and required hospitalization. 13
Proper diagnosis and treatment negotiation are vital in DP cases, where a multi-professional approach is essential. In primary DP with solitary delusion, antipsychotic medication is beneficial, especially risperidone. 14 Our patients showed significant improvement at six weeks of treatment with risperidone. Consideration of the Explanatory Model of Illness of patients is essential in the treatment negotiation. Good rapport, reassurance, supportive psychotherapy, and pharmacotherapy yield good therapeutic outcomes. The associated repetitive body-focused behavior responds well to minimizing symptoms with antipsychotic therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Informed written consent was taken from the patient and her husband to publish the case with a photograph in an academic journal.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.