
Abstract

To the Editor,
In obsessive-compulsive disorder (OCD), functional impairments may be attributable to neurocognitive impairments persisting in remission. Cognitive training (CT) may enhance cognitive and clinical recovery through neuroplasticity. 1 Studies on CT in OCD are sparse and demonstrate limited improvements in untrained domains.2–6
The current study attempts to pilot a structured 8-week cognitive control training (CCT) program for OCD, which is based on previous work demonstrating improvements in trained and untrained domains. 7
Methods
We recruited, with informed consent, 10 individuals with remitted obsessive-compulsive disorder (OCD), who were right-handed, were aged 18–50 years, had a minimum of 7 years of education, were suitable for neurocognitive testing, were on stable medication for 3 months, had not received structured psychotherapy in the preceding 6 months, and did not have severe depression, psychosis, bipolar disorder, substance/behavioral addictions, acquired brain damage, or developmental disorders. Of those recruited, 5 received cognitive control training (CCT) over the next 8 weeks; practical constraints prevented the other 5 from attending the intervention; these comprised the usual care (UC) comparison group.
After screening, all participants were assessed at baseline, and after 8 weeks, on the severity of OCD, anxiety, and depression; cognitive control; planning; memory; perceived cognitive deficits; metacognitive monitoring; and socio-occupational function (Table 1). The study was carried out in accordance with the guidelines of the Institute Ethics Committee and approved by the Department of Clinical Psychology Ethics Subcommittee.
The CCT program 7 was delivered individually, with 1 hour, weekly, therapist-guided sessions and 30 min, 4 times weekly homework (logged by participants), and included the following:
Cognitive stimulation: This refers to challenging and progressively difficult activities facilitated by neuroplasticity 8 and delivered through games (weeks 1–7 – Cogtrain, Mental Counting, Sudoku, Connect-4, and Brainvita). 7 Cogtrain, a novel smartphone application for visuospatial working memory, was developed through the process of domain identification, item generation, item analysis, game development on an open-source platform, quality testing, debugging, expert validation, and iterative modification, followed by deployment on Android, iOS, and browser platforms through a link. The game requires the player to reproduce a visual sequence of windows lighting up in a building. Speed and span length are pre-set and progressively increase in difficulty based on player success (details of the game described previously). 7
Metacognitive strategy monitoring involves monitoring one’s own strategy use through training. 8 This component (weeks 2–7) was operationalized as: (a) improving awareness of cognitive processes—through discussion/education regarding attention, memory, planning, procrastination, decision-making, and perfectionism; (b) enhancing monitoring abilities—through mindfulness exercises like coloring, clock for mindfulness, and 3-min meditation; and (c) task-specific application—facilitated through monitoring of strategy use during the cognitive stimulation tasks and identifying, modifying, and reviewing the strategies.
Generalization involves facilitating the transfer of training effects to daily life through the mechanisms of rehearsal and practice. 8 This component (weeks 2–8) was delivered through discussion of real-world applications of abilities and strategies, scheduling of daily routines, role-plays, and engagement in occupational tasks from participants’ own everyday lives.
The UC group received medications and routine follow-ups in the OCD Clinic.
Data were analyzed using the Statistical Product and Service Solutions (SPSS 20.0; IBM Corp.). Pre- and post-intervention differences were examined through change scores, with Cohen’s effect sizes corrected using Klauer’s formula.
Results
Participants in both groups were comparable in sex distribution (n (males), CCT:UC = 3:2); age in years, mean ± SD (CCT, 33.4 ± 11.01; UC, 29 ± 5.43), years of education (CCT, 16 ± 1; UC, 15.8 ± 0.84), duration of illness in years (CCT, 5.4 ± 1.2; UC, 5.6 ± 2.70); number of illness episodes (CCT, 1.4 ± 0.55; UC, 1.2 ± 0.45), duration of remission in months (CCT, 9.2 ± 1.47; UC, 8.4 ± 2.30), and common comorbidities (1 each in CCT and UC with generalized anxiety disorder and depression, social anxiety disorder, and panic disorder). Both groups were on medication (CCT:UC—Escitalopram, 2:2; Sertraline, 1:2; Fluvoxamine, 1:1; and Venlafaxine, 1:0). Pre-intervention clinical measures were similar in both groups, and the CCT group showed significant improvements across all domains with large effect sizes (Table 1).
Comparison of Baseline and Post-Intervention Differences in Clinical, Cognitive, and Socio-Occupational Measures for CCT and UC Groups.
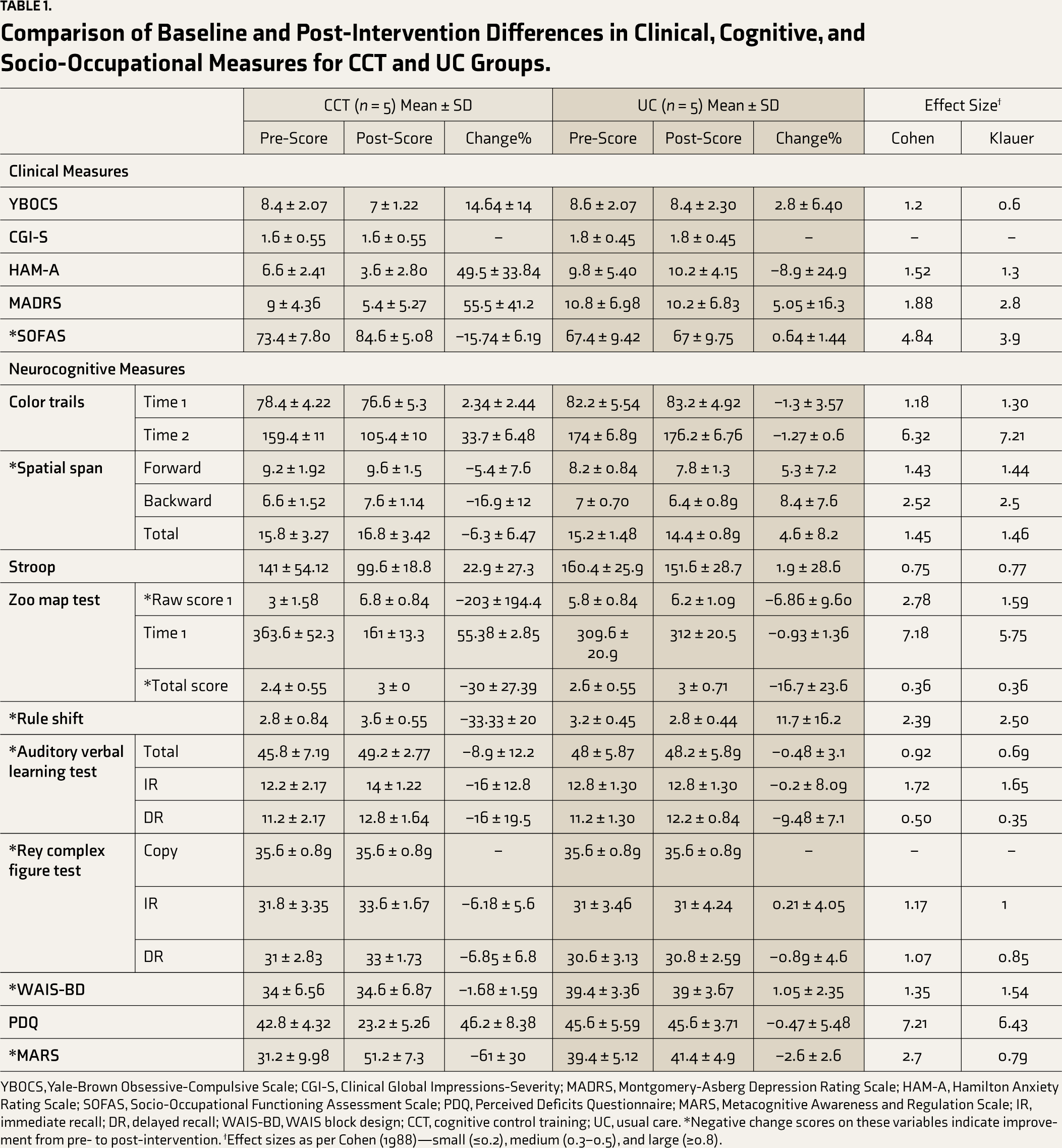
YBOCS, Yale-Brown Obsessive-Compulsive Scale; CGI-S, Clinical Global Impressions-Severity; MADRS, Montgomery-Asberg Depression Rating Scale; HAM-A, Hamilton Anxiety Rating Scale; SOFAS, Socio-Occupational Functioning Assessment Scale; PDQ, Perceived Deficits Questionnaire; MARS, Metacognitive Awareness and Regulation Scale; IR, immediate recall; DR, delayed recall; WAIS-BD, WAIS block design; CCT, cognitive control training; UC, usual care. *Negative change scores on these variables indicate improvement from pre- to post-intervention. ϯEffect sizes as per Cohen (1988)—small (≤0.2), medium (0.3–0.5), and large (≥0.8).
Participant feedback highlighted benefits from cognitive stimulation, metacognitive monitoring, and generalization (A: “…reflections after each game helpful. Before… mess in mind. Now I can track what is going on in my mind and regulate it”; D: “used to procrastinate a lot… now… able to start something by seeing it as a challenge…”).
Discussion
The piloted CCT program demonstrated improvements in cognitive control (cognitive flexibility, working memory, and inhibitory control), along with the transfer of training to untrained domains—other neurocognitive functions (planning, verbal and nonverbal memory, and visuospatial construction), self-reported cognitive deficits, metacognitive monitoring, clinical measures (severity of OCD, depression, and anxiety), and socio-occupational functioning. The UC group did not match the change scores of the CCT group.
Several factors may explain the observed broad transfer of training, in contrast to previous studies:
Dose and duration: a total of 24 h of training across 8 weeks utilized in this study fits with evidence-based recommendations
9
and contrasts with briefer interventions in previous studies (1–9 h in total). The focus on cognitive control, a core process impacting higher-order functions in OCD, contrasts with narrower foci chosen in previous studies that may not apply to all individuals within a diagnostic category.
1
A process-specific approach to training (vs. content-specific training), involving complex and variable task settings with progressive difficulty levels and multiple response possibilities at every move may have facilitated transfer and minimised rote learning.
10
Use of techniques for enhancing self-awareness and generalization, including metacognitive monitoring, and application to everyday life, is in line with evidence-based recommendations for cognitive training (CT).
8
Although the current study examined remitted OCD, improvements based on the above principles may also apply to symptomatic OCD. Our study had several limitations, including the small sample, lack of random assignment, active intervention comparison, and lack of follow-up data to assess the durability of improvements. However, the presence of blind raters for clinical measures minimized measurement confounds.
Given the nascent stages of CT research in OCD, the improvements across cognitive, clinical, and functional domains make room for cautious optimism. Our findings highlight the role of process-specific cognitive stimulation, accompanied by metacognitive monitoring and generalization exercises, and will inform larger efficacy trials of symptomatic OCD (e.g., inhibitory control, which currently demonstrates medium effect size, needs strengthening in future). Possible mechanisms, necessary and sufficient components, and predictors and moderators of treatment engagement and response remain to be understood. 1 Given the significance of functional impairments in many psychiatric disorders and the transdiagnostic role of cognitive control and metacognitive strategies, there is potential for the extension of the CCT program to other disorders.
Footnotes
Acknowledgements
The authors would like to thank Dr. Janardhanan C. Narayanaswamy and Dr. Paulomi Sudhir for valuable inputs on the cognitive training program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.