
Abstract
Background:
The emotion of disgust has been linked with the underlying nature of the contamination subtype of obsessive-compulsive disorder (C-OCD). Prior studies show that disgust contributes to the development of C-OCD by reinforcing avoidance strategies. Therefore, experiential avoidance (EA) may influence the effect between disgust sensitivity (DS) and C-OCD symptom severity. This study aimed to investigate the mediational role of EA between DS and C-OCD severity.
Methods:
A cross-sectional design was adopted with 45 patients of OCD and 45 healthy controls. Both the groups were assessed on the Obsessive-Compulsive Inventory, the Disgust Scale (Revised), and Acceptance and Action Questionnaire–II. Yale-Brown Obsessive Compulsive Scale (Y-BOCS) checklist and symptom severity scale were additionally administered to the patients with OCD. Independent t-tests, Pearson’s product–moment correlation, regression analysis, and mediation analysis were used.
Results:
DS and EA were positively associated with contamination-washing symptoms and symptom severity. Regression analysis indicated that DS and EA were highly associated with contamination/washing severity scores among both the patients with C-OCD and the healthy controls.
Conclusion:
The study implicates that disgust is a central emotion underlying the presentation of obsessions and compulsions, which are of contamination concerns. Further, EA has a role in the maintenance of OCD through avoidance learning; however, it may not be interacting with DS to cause OCD.
Disgust and experiential avoidance are associated with C-OCD. The finding supports that avoidance learning plays a role in maintenance of contamination subtype OCD. Experiential avoidance may be targeted using third generation Cognitive behavior therapy.Key Messages:
Obsessive-compulsive disorder (OCD) is characterized by obsessions and/or compulsions, which are severe in most cases, 1 making it the third most severe psychiatric condition. 1 Given the variability in the prevalence of OCD subtypes and symptom dimensions across studies, the contamination/washing dimension is consistent, clearly defined, 2 and the most common among individuals with OCD. 3 The contamination subtype label of OCD refers to predominantly contamination-related symptoms and intrusive thoughts of germs, dirt, or illness, creating anxiety, disgust, or discomfort. 4 These obsessions are further associated with washing and/or cleaning compulsions. Contamination fears are present in approximately half of the patients with OCD and among the most disabling of OCD symptoms. 5 For the present research, we refer to the contamination subtype/dimension of OCD as contamination OCD (C-OCD).
In recent years, an area investigated in C-OCD is the role of disgust in the etiology of OCD. Disgust sensitivity (DS) is the trait-like predisposition of a person to become disgusted in response to a particular group of stimuli, known as disgust elicitors. 6 While most individuals with contamination fear report experiencing anxiety when faced with contaminants, increasing evidence suggests that the emotion of disgust contributes to contamination concerns. 7 DS may contribute to the development of OCD by reinforcing avoidance strategies.7,8
Experiential avoidance (EA) is an unwillingness to experience or remain in contact with unpleasant emotions, thoughts, bodily sensations, or other private experiences. 9 Previous research has found a relationship between EA and OCD. 10 A recent study 11 found that facets of EA (i.e., distress endurance and repression) correlate with C-OCD.
DS has been found to be elevated in individuals with OCD12,13 and may be an associated factor for the disorder. 13 Small-to-medium strength associations between measures of DS and OCD symptomatology have been consistently found for both clinical2,8,14 and nonclinical samples.15,16 However, merely believing that a high level of DS would be the sole associated factor for the development of C-OCD does not go well with the fact that some people with high DS remain free from OCD. It indicates that other putative factors might contribute to the pathology of OCD. EA may maintain C-OCD through relentless efforts to avoid aversive subjective experiences. 17 This could indicate that manipulating EA through appropriate psychological intervention may have additive advantages in treating C-OCD. 17 So far, no empirical study has explored the role of EA and DS in C-OCD. We aimed to study the role of EA and DS in C-OCD and hypothesized that EA would mediate between DS and symptom severity in patients with C-OCD.
Material and Methods
Sample and Design
The cross-sectional study was approved by the Institute Ethics Committee at the National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore. Patients (n = 45) who satisfied the study criteria were recruited from the outpatient department of the institute. Healthy controls (n = 45) were matched for age and gender to that of the patients and recruited through purposive sampling from the local community. Only those who scored <3 on the NIMHANS Psychiatric Morbidity Screening tool 18 were considered healthy controls.
Inclusion criteria for patients were: primary diagnosis of OCD according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and/or International Classification of Diseases (ICD-10) criteria, presence of contamination obsessions, and washing/cleaning compulsions on the Yale–Brown Obsessive-Compulsive Scale (Y-BOCS) checklist, 19 a total score of ≥16 on the Y-BOCS, and age range of 18 to 60 years. Exclusion criteria were having a comorbid diagnosis of psychosis, bipolar affective disorder, severe depression with psychotic symptoms, substance dependence, intellectual disability, epilepsy, head injury, or other neurological disorders that make the patients nonamenable for assessment. Also, patients undergoing or who had undergone CBT or mindfulness-based interventions in the previous year were excluded.
The sample size was estimated using G*Power software based on the total scores of the Disgust Scale-Revised in a previous study 20 in the clinical and healthy control groups. Effect size (i.e., Cohen’s d) of 0.53 at a significance level of 0.01, power of 80%, and a one-tailed analysis were used as criteria for estimating the sample size, which was estimated to be 45 for each group.
Procedure and Assessment
The data were collected between June 2018 and April 2019. The researcher interviewed patients who gave informed consent using Mini-International Neuropsychiatric Interview (MINI Plus 5.0) 21 to confirm the diagnosis of OCD and exclude comorbid psychiatric disorders. They were assessed on the Y-BOCS symptom checklist and severity. The NIMHANS psychiatric morbidity screening tool was administered to the healthy controls for screening. This is a 7-item scale to screen out psychiatric cases. It has a sensitivity of 0.79 and a specificity of 0.76. The scale’s test-retest reliability is 0.89. 18
Further Tools Used in Both Groups
The Obsessive-Compulsive Inventory-Revised (OCI-R) 22 is a self-report instrument to determine the diagnosis and severity of OCD. The OCI-R consists of 42 items in seven subscales. It has high test-retest reliability for both patients with C-OCD as well as healthy controls (OCD, r = 0.87; controls, r = 0.89). Convergent validity for the OCD sample and healthy controls were 0.93 and 0.69, respectively. 23 Only the “washing” subtype score on the OCI-R was considered for the present study.
The Disgust Scale-Revised (DS-R) is a 25-item questionnaire assessing one’s general proneness to disgust. It has excellent internal consistency (α = 0.90) and has been shown to have adequate split-half reliability and convergent validity with other measures of disgust. 13
Acceptance and Action Questionnaire-II (AAQ-II) 24 is a 7-item scale that assesses EA. Its mean α coefficient was 0.84, and the 3- and 12-month test-retest reliability were found to be 0.81 and 0.79, respectively.
Data Analysis
The quantitative data were analyzed using IBM Statistical Package of Social Sciences (SPSS) Statistics for Windows, version 22.00 (IBM Corp., Armonk, NY, USA). Whether a statistically significant difference in DS and EA exists between patients with C-OCD and healthy controls was established using an independent samples t-test. The correlation of DS and EA with Y-BOCS symptom severity in patients with C-OCD was determined using Pearson’s product-moment correlation coefficient. Next, DS, EA, and washing symptom severity (as measured by the OCI-R washing subscale) were correlated for C-OCD and healthy controls. This was followed by regression analysis for both groups to determine to what extent contamination/washing severity scores were predicted by DS and EA. The mediatory effect of EA between DS and washing symptom severity was explored using Andrew F Hayes Process Macro version 3.0 for SPSS. All tests were two-tailed, and the statistical significance level was set at 0.05.
Results
As age was not normally distributed among patients with C-OCD (n = 45) and healthy controls (n = 45), the Mann–Whitney U test was administered to determine how the groups significantly differed. No statistically significant difference was found in the age (P = 0.85) or gender among patients and healthy controls (Table 1). The significance on the Shapiro–Wilk test (0.05) revealed that the patients were normally distributed for their levels of washing symptom severity, DS, and EA. Hence, parametric statistics such as t-tests and Pearson’s product-moment correlation were administered for further statistical analysis.
The difference in levels of washing symptom severity (i.e., OCI-R washing subscale), DS, and EA between patients and healthy controls was significant (P = 0.001, Table 1).
Demographic and Clinical Characteristics of Patients and Controls
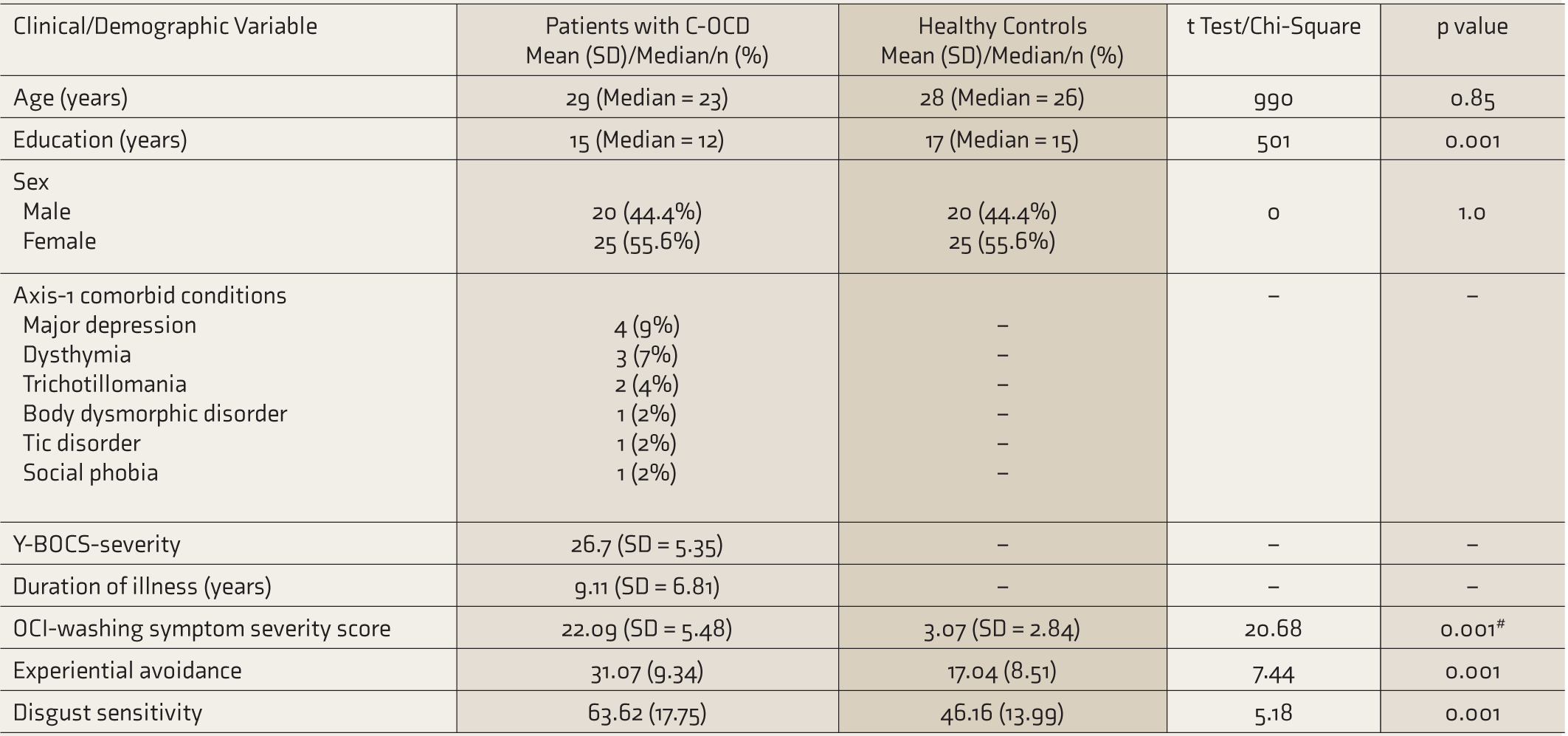
#, Welch Test; C-OCD, contamination OCD; Y-BOCS, Yale–Brown Obsessive-Compulsive Scale; OCI-Washing, washing domain of the Obsessive-Compulsive Inventory-Revised; OCD, obsessive-compulsive disorder; SD, standard deviation.
Among patients, a low positive correlation was seen between the Y-BOCS symptom severity and DS, which was not statistically significant (Table 2). However, Y-BOCS symptom severity had a statistically significant (P = 0.03) moderate and positive correlation with measures of EA.
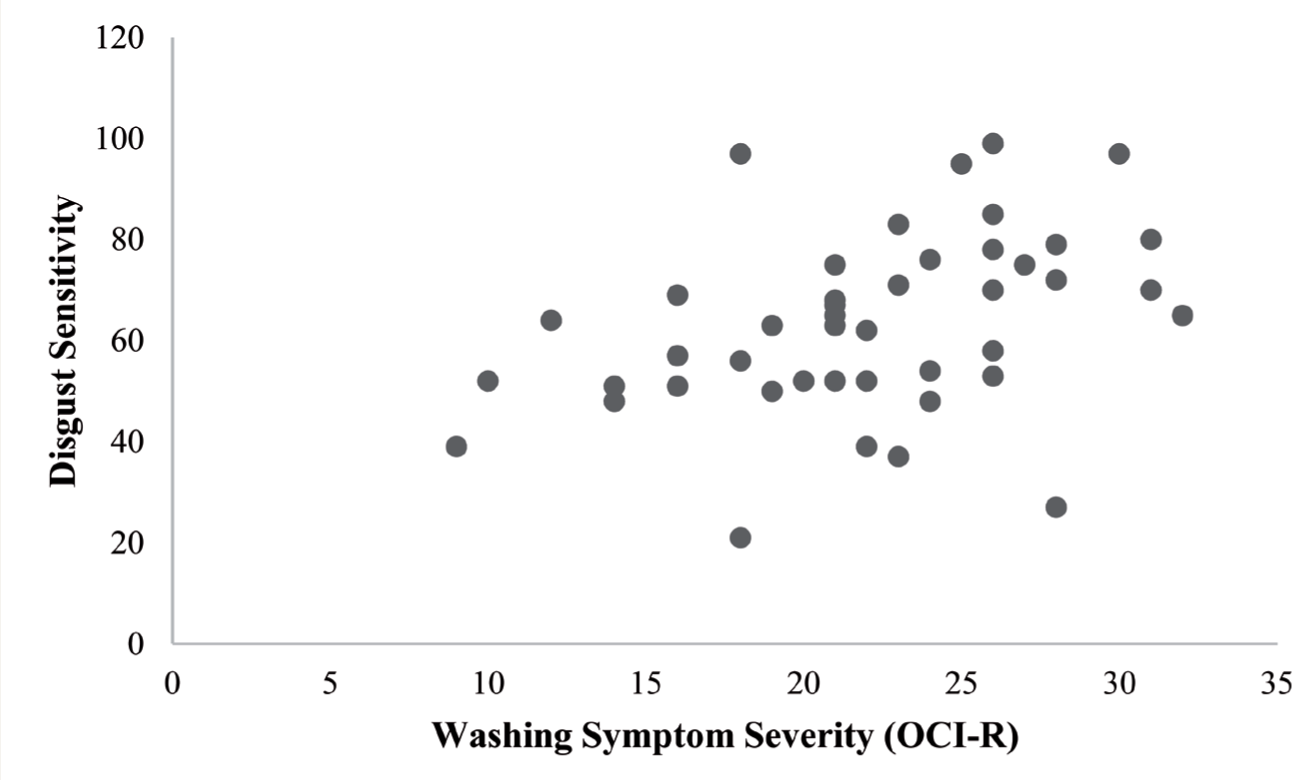
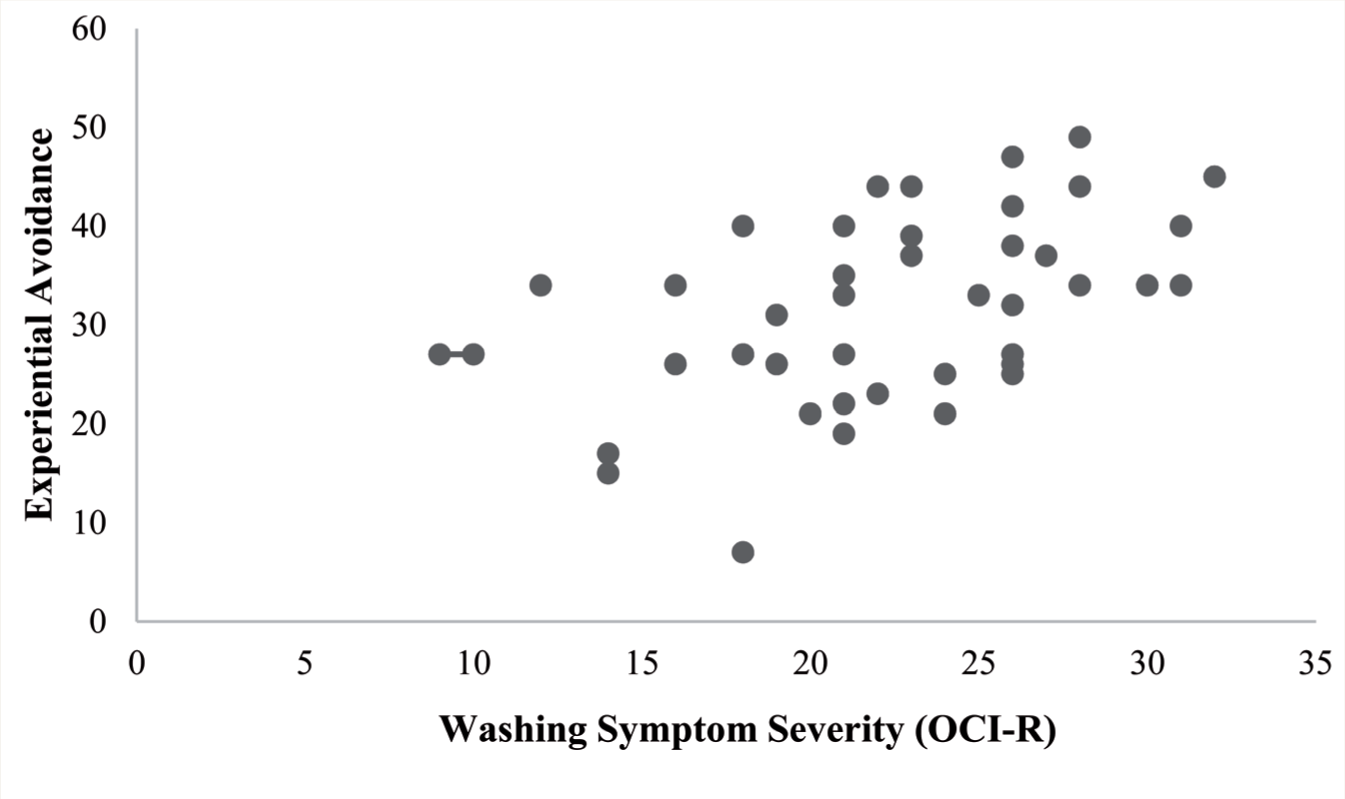
Among patients, both DS (P = 0.005) and EA (P = 0.001) had a moderate positive correlation with washing symptom severity, which was statistically significant (Figures 1 and 2, Table 3).
Correlation of Disgust Sensitivity and Experiential Avoidance with Y-BOCS Symptom Severity Score Among Patients with C-OCD

*P = 0.05. Y-BOCS, Yale–Brown Obsessive Compulsive Scale; C-OCD, contamination OCD; OCD, obsessive-compulsive disorder.
Correlation of Disgust Sensitivity and Experiential Avoidance with Washing Symptom Severity

*P = 0.05; **P = 0.01. C-OCD, contamination OCD; OCI-R, Obsessive-Compulsive Inventory-Revised; OCD, obsessive-compulsive disorder.
OCI-R, Obsessive-Compulsive Inventory-Revised.
OCI-R, Obsessive-Compulsive Inventory-Revised.
Among healthy controls, washing symptom severity had a significant moderate positive correlation with both DS (P = 0.008) and EA (P = 0.03, Table 3).
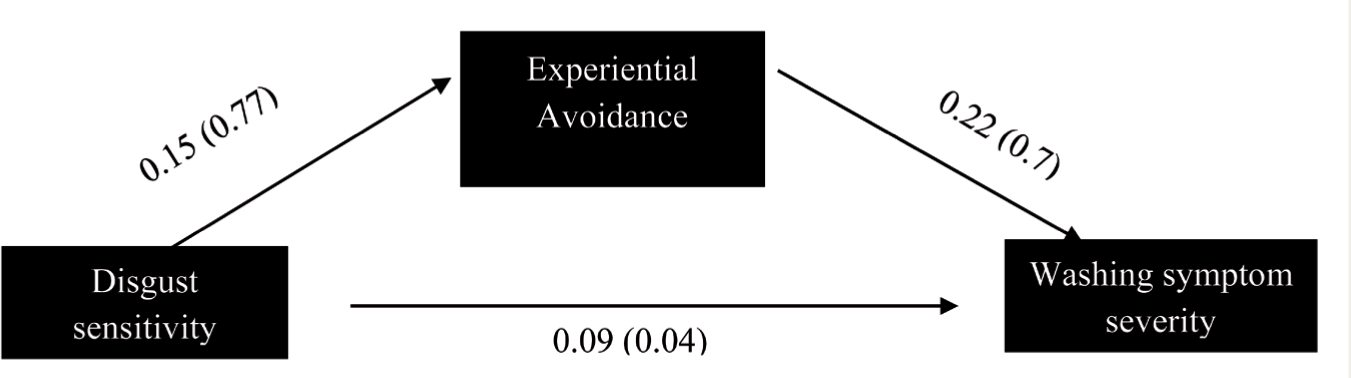
Regression analysis indicated that DS and EA are significant predictors of washing symptom severity among both patients with C-OCD and healthy controls. The regression model explained 25% and 22.4% of the variance in washing scores in patients with C-OCD and healthy controls, respectively (Table 4). Additionally, the direct effect (path coefficient) of DS on washing symptom severity score was found to be 0.09. In contrast, the indirect effect of DS on washing symptom severity score through EA (assumed to be a mediator) was 0.03 (Figure 3). Hence, DS alone has a higher direct effect on washing symptom severity without EA mediating between them.
Predictors of C-OCD Severity (Washing Symptom Severity)
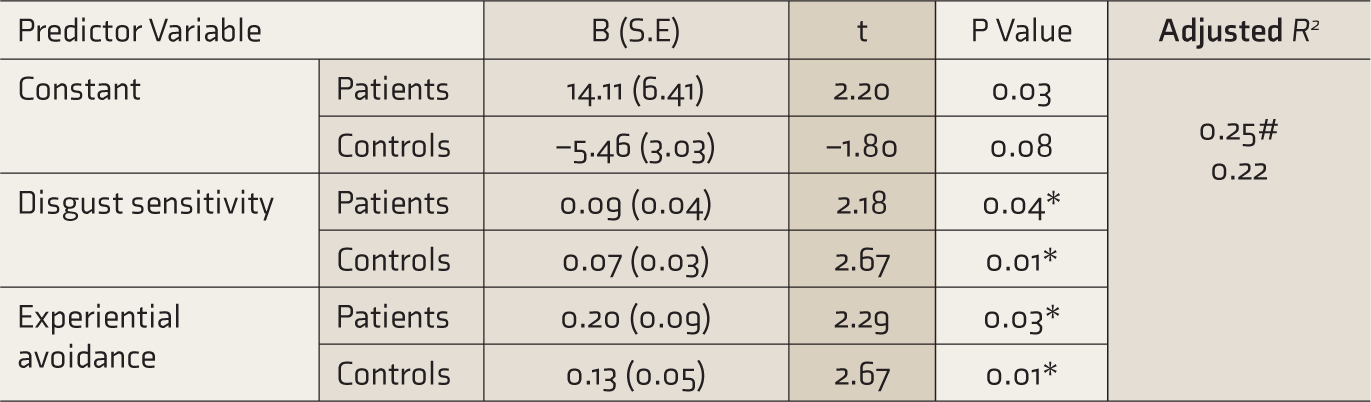
*P = 0.05; #, Adjusted R2 for patients.
C-OCD, contamination OCD; OCD, obsessive-compulsive disorder.
Discussion
The groups significantly differed in the levels of DS and EA. For the symptom severity as measured by the Y-BOCS severity score, DS had a low positive correlation, which was not statistically significant. This may be attributed to the Y-BOCS severity score considering global obsessive-compulsive symptoms rather than concerns related to contamination alone. Hence, it may be understood that while disgust may have some underlying role in explaining contamination, it does not explain the other obsessive thoughts or compulsive behaviors, such as checking, thoughts of harm, need for symmetry, etc. However, EA was still found to have a significant association with Y-BOCS severity scores. This may indicate that irrespective of the nature of the OCD, patients may engage in high avoidance behaviors. However, previous studies have had an inconclusive association between EA and OCD symptoms severity. For instance, in one study, although EA was significantly correlated with the dimensional Y-BOCS score, there were differences across the symptom dimensions, with EA significantly correlating with unacceptable thoughts, responsibility for harm, and symmetry but not with C-OCD. 25 We can assume that there might be some role that EA plays, as patients with OCD have difficulty withdrawing themselves from performing the compulsions.
Increased levels of DS were associated with increased symptoms related to contamination concerns and washing. This finding has been confirmed by several studies in the past, which have consistently proven small to moderate strength correlations between DS and symptom severity.6,7,13–15 In the present study, the correlation between DS and washing symptom severity was moderate, which indicates a specific role of disgust in C-OCD. EA has also shown a significant relationship with washing severity. Disgust has a unique contribution to contamination concerns and washing compulsions, as feelings of disgust may contribute to higher phobic avoidance of the stimulus, which maintains the illness. 26 It is worth noting that this phobic avoidance of the stimulus may be sustained with the EA that a person may have. Previous research had confirmed that individuals high in contamination fears report higher levels of disgust when exposed to contamination-related stimuli and increased avoidance behavior in response to disgust. 27
Predictors of Obsessive-Compulsive Symptom
DS and EA significantly predicted symptoms of contamination concerns and washing. In another study, DS, along with health anxiety, added up to only 2% to 3% of the total variance in OCD severity score. 28 In our study, DS had a higher direct effect on symptom severity alone, without EA. This indicates that EA might not be a potential mediator between DS and washing symptom severity among patients with C-OCD. A previous study 13 also revealed that DS alone had a higher path effect on washing and contamination-related concerns, without trait anxiety being a potential mediator.
Another study concluded that feelings of incompleteness and several “not just right experiences” partially mediated the relationship between disgust and fear of contamination, but harm avoidance and obsessive beliefs around overestimation of threat did not. 29 Hence, we suggest that EA has a role in the maintenance of OCD through avoidance learning. However, it may not be interacting with DS to cause OCD. This goes in line with an earlier model proposed: that some patients with C-OCD are not fearful that contamination will cause harm but rather engage in avoidance and neutralizing behaviors to reduce or eliminate the experience of disgust, thus emphasizing the difference between harm avoidance and disgust avoidance. 30
It is possible that the symptoms of C-OCD do not result much from cognitive appraisals but are sensation/feeling-based, especially when there is a heightened response to disgust. Two studies that focused on exposure tasks involving fear and disgust ratings revealed that while there was a significant reduction in fear, habituation to disgust was much slower.31,32 This highlights the important differences in the unique mechanism of disgust compared with other factors in patients with OCD, with the experience of disgust being more resistant to extinction than fear. 33
A previous study had suggested that response to different stimuli or classes of stimuli could form an important basis for determining intervention methods for different primary presenting symptoms of OCD. 31 Apart from exposure-based interventions, one may assume that changing a person’s thoughts could potentially elicit durable changes in emotional responses. A study showed that participants who engaged in cognitive reappraisal demonstrated a reduction in learned disgust across sessions and further benefited from the extinction of disgust responses. 34 This suggests that cognitive reappraisal may be used further to attenuate learned disgust.
Limitations and Implications of the Study
The study implies that disgust is a central emotion underlying the presentation of obsessions and compulsions that involve contamination concerns. Hence, addressing strong emotional processing as a precursor to the washing symptoms, rather than solely focusing on the maladaptive cognitions, could be beneficial. The role of cognitions, beliefs, and appraisals may not be entirely limited but have the scope to be investigated further. However, discounting the relevance of disgust can impede successful treatment outcomes and, in turn, may limit clinical gains if treatments selectively focus on reducing anxiety or appraisals. Therefore, identifying strategies that effectively target disgust may not only reduce symptoms, but also reduce costs, dropout rates, and duration of treatments.
In the present study, the group was heterogeneous in clinical presentation despite the C-OCD sample having primarily symptoms of contamination. Other factors such as state/trait anxiety and cognitive appraisals were neither investigated nor controlled for. A smaller sample size limits the generalization of findings. Hence, the results need to be validated in a larger sample. Regression analysis was required in this cross-sectional study to perform mediational analysis. Though it does not indicate causality, it needs to be interpreted cautiously. Another limitation is that the sample size calculation was done based on group differences in levels of DS and not solely for mediational analysis, the initial objective of the study. The interaction of disgust and cognitive appraisals could also provide further scope for investigation. Newer research in the domain of disgust and OCD could also examine the role of dispositional mindfulness while considering the individual’s state/trait anxiety levels.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for research, authorship, and/or publication of this article.