
Abstract
Background:
The role of memory in obsessive-compulsive disorder (OCD) has been an area of research that has yielded mixed results, particularly in prospective memory (PM) functioning. Hence, one objective of the study was to assess PM deficits in patients with OCD. Also, research in this area has been sparse, and most researchers have used questionnaires and people with subclinical symptoms of OCD, which might have impacted the generalizability of the findings. Thus, the second objective was to assess PM functioning using a performance-based task in persons with OCD having clinical symptoms.
Methods:
This is a cross-sectional comparative study of 30 adults with OCD and 30 adults without psychiatric morbidity. The tools used were Dimensional Yale-Brown Obsessive-Compulsive Scale (DY-BOCS), Hamilton Depression Rating Scale (HAMD), General Health Questionnaire-12 (GHQ 12), and Cambridge Prospective Memory Test (CAMPROMPT).
Results:
Event-based PM was significantly poor in the OCD group. In time-based PM, no significant difference was found between the groups. Three subgroups in OCD, predominantly obsessions, predominantly compulsions, and mixed types, did not differ significantly with respect to PM.
Conclusion:
The result suggested a deficit of event-based PM in OCD, which can help understand the psychopathology of memory deficit in the clinical population and bridge the gap with respect to memory research in this domain.
Keywords
The role of prospective memory (PM) in obsessive-compulsive disorder (OCD) has been an unexplored area. Ours is one of the few studies to use a sample with clinical symptoms of OCD to explore the possibility of dysfunction of PM. Its finding of deficits in event-based PM might help us understand the neuropsychological basis of this disorder more effectively.Key Message:
People with obsessive-compulsive disorder (OCD) have often been found to have pathological doubt, which probably reflects their uncertainty about the properties of the stimulus, situation, or event. 1 For example, people with OCD frequently tend to report uncertainty about whether they have performed actions correctly, have contacted contaminants, etc. People with obsessive-compulsive symptoms are likely to engage in compulsive behaviors such as checking, washing, assurance-seeking, and repeating activities in an attempt to reduce their doubt. As one of the hypotheses, memory deficit is regarded as the source of doubt in OCD, 2 although research on memory deficits in OCD has yielded mixed results. 3
Prospective memory (PM) is a type of memory where a person has to remember to perform future actions at a particular time (e.g., remembering to call the clinic at 11 am for an appointment) or in response to a particular event (e.g., remembering to switch the light off after leaving the room) that are important in our daily lives. This type of memory has been extensively studied in various neurological and psychiatric disorders like Parkinson’s disease, 4 schizophrenia,5,6 depression,7–10 and Alzheimer’s disease11–13 and is found to be impaired.
However, studies exploring its role in OCD have been sparse and equivocal. 14 Most studies have used individuals with subclinical OC symptoms,15–19 thereby reducing the generalizability of findings. In another study, PM and metamemory were compared between normal persons and individuals with obsessive symptoms/features in the general population, impacting the findings’ generalizability to individuals with clinical OCD. 20 The literature review also revealed that most studies like Cuttler and Graf,15–17 Palmer et al., 21 and Vafa et al. 22 used questionnaires like the Prospective and Retrospective Memory Questionnaire and Prospective Memory Questionnaire (PMQ), which might not provide an objective understanding of the variable under study as questionnaires have their disadvantages. A few studies used individuals with clinical OC symptoms and performance tests14,23,24 while assessing PM functioning or its nature. The objective of our study was to assess PM deficits in patients with OCD and assess PM functioning using a performance-based task.
Material and Methods
Study Design
It was a cross-sectional comparative study based on purposive sampling, carried out in a super-specialty psychiatric set up in the state of West Bengal, of persons with OCD with mild to moderate levels of depression (score ≤15 on Hamilton Depression Rating Scale) 25 and normal healthy individuals without any history of psychiatric morbidity and <12 score in the Likert version of General Health Questionnaire-12. 26 To assess PM, we used a neuropsychological assessment tool called Cambridge Prospective Memory Test (CAMPROMPT, Pearson, UK).
Participants
A total of 60 adults were taken, with 30 diagnosed with OCD as per International Classification of Diseases, 10th revision (ICD-10), and taking treatment in a government tertiary care center in West Bengal. All patients had to be under psychiatric treatment for a minimum of three months and take selective serotonin reuptake inhibitors (SSRIs). The rest of the 30 individuals were nonpsychiatric comparative adults (i.e., normal healthy controls, NC). They were included after taking the informed consent in a written form.
The inclusion criteria for both groups were: (a) minimum education of class 10, (b) both male and female, (c) 18 to 40 years, and (d) right-handed.
The exclusion criteria were: (a) history of substance dependence and psychosis, (b) history of any major physical or organic illness, and (c) females who have attained menopause.
Procedure
After receiving approval from the Institutional Ethics Committee of IPGMER and SSKM Hospital, patients coming to the out-patient department (OPD) of the psychiatry unit of Institute of Psychiatry: A Centre of Excellence, Kolkata, with a diagnosis of OCD as per ICD-10 27 were contacted. They were briefed about the purpose of the study, and their consent was taken. To rule out alcohol or substance dependence and psychotic disorders, the Mini International Neuropsychiatric Interview (MINI, Version 5.0) 28 was administered. They were then interviewed using the Dimensional Yale-Brown Obsessive-Compulsive Scale (DY-BOCS) 29 to determine the presence and severity of obsessions and compulsions with respect to the different dimensions of OCD. This scale includes sections on contamination, hoarding, symmetry, sexual and religion, aggression, and a miscellaneous section. It is an extension of the original Yale-Brown Obsessive-Compulsive Scale (Y-BOCS). The Hamilton Depression Rating Scale was given to assess their level of depression, and the Edinburgh Handedness Inventory 30 was administered to determine their handedness. Those who met the inclusion criteria were included in the group. The sociodemographic details, including age, sex, education, occupation, income, marital status, residence, and family type, were collected. Other necessary information regarding the symptoms, treatment history, and family history was also collected. After the initial briefing and information gathering, the data was collected at the OPD using CAMPROMPT. 31 It is an objective and standardized clinical instrument offering insights into a client’s PM or ability to remember to do things at a particular time or within a given interval. The test has good reliability and validity. A low score on PM tasks means the client requires prompts to remember to perform the task, indicating a PM deficit.
The NCs were selected from in and around the hospital, including staff and family members of patients in general medicine OPD. In addition to the MINI and Edinburgh Handedness Inventory, GHQ-12 was administered to rule out any psychological morbidity. The Likert scoring method was used in calculating the scores of GHQ-12, and those scoring <12 were retained. 32 Those who met the inclusion criteria were selected, and the rest of the procedure followed was similar to that of the study group. The data collection lasted between March 2016 and January 2017.
Statistical Methods
Thus, the data obtained were subjected to the following statistical treatment using the Statistical Package for Social Sciences Version 15 (SPSS 15, Chicago). Homogeneity of variance was assessed using Levene’s test for equality of variances. Because homogeneity of variance was found to be present amongst most of the variables and for age and PM variables, normal distribution was found; hence, parametric tests were used. Under sociodemographic variables, for categorical variables, the chi-square test was done, and for continuous variables, a t-test was done. The student’s t-test was done to determine whether there was any significant mean difference between the two groups: OCD and NC, with respect to PM. Pearson correlation was done with respect to depression (Hamilton Depression Rating Scale [HAMD] scores), duration of illness, and PM variables (time-based, event-based, and total) to determine the association between them.
The one-way analysis of variance was done to assess whether there was any difference between the micro-OCD types–predominantly obsession, predominantly compulsion, and mixed types with respect to PM (time-based, event-based, and total). The Kruskal–Wallis test assessed the impact of the different obsessions such as aggression, sexual, symmetry, cleaning, miscellaneous, and mixed types on PM again (time-based, event-based, and total).
For all the analyses, α < 0.05 (P-value) was considered acceptable significance level.
Results
Table 1 demonstrates the categorical and continuous sociodemographic details distribution between OCD and NC groups. Both the groups could be matched based on sex, education, family type, residence, marital status, and income; however, with respect to age, a significant difference was observed between the two groups at a P-value of 0.046.
Distribution of Sociodemographic Variables Between OCD Group (N1 = 30) and NC (N2 = 30)
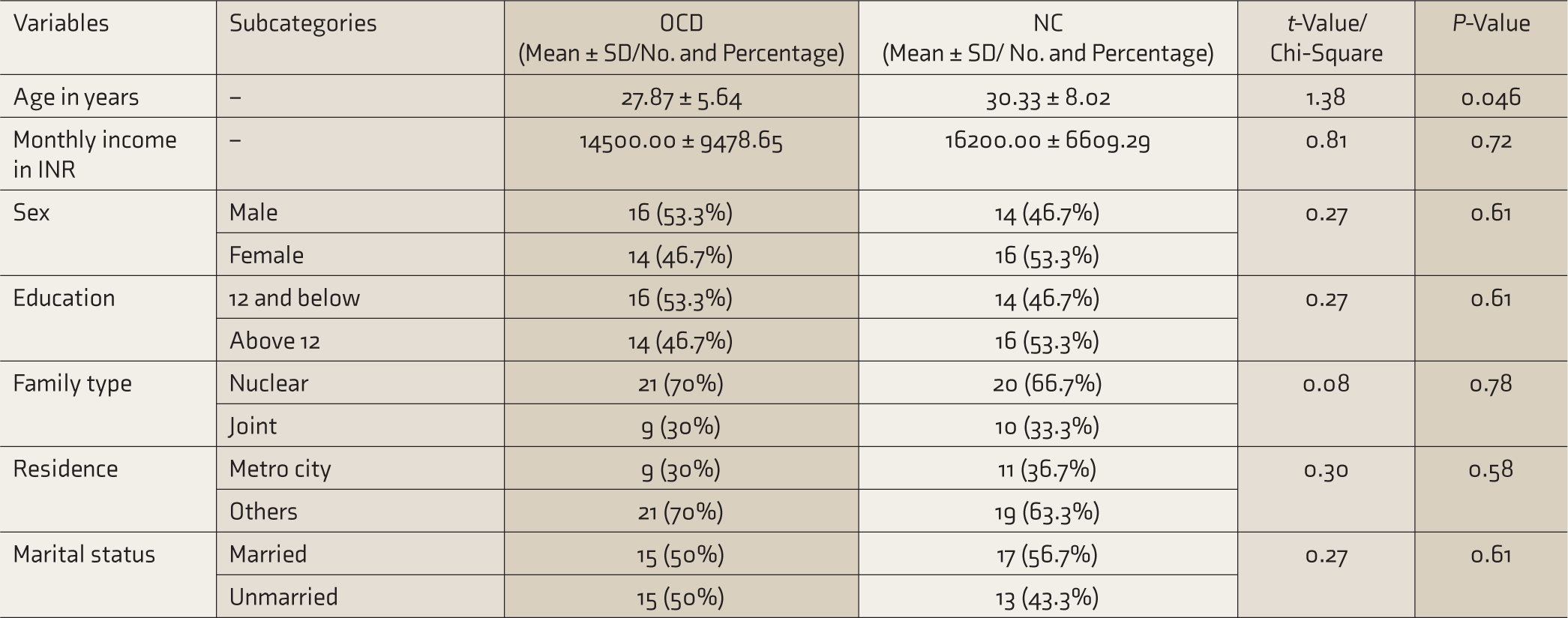
PM, prospective memory; OCD, obsessive-compulsive disorder; SD, standard deviation.
In the OCD group, the mean (SD) duration of illness was 5.65 (2.97) years, and the duration of treatment was 2.97 (2.59) years. Around 13% of patients received only pharmacological intervention, primarily SSRIs, whereas the rest received both pharmacological and psychotherapeutic treatment. The mean depression score on HAMD was 10.73 (2.13). For the NC, the mean GHQ-12 score was 9.67 (3.04), below the cut-off score of 12.
Characteristics of Prospective Memory in OCD and NC
Table 2 shows that the OCD group had poorer event-based PM, which was statistically significant at a P-value of 0.005, with a moderately large effect size (Cohen’s d = 0.75). However, in the time domain of PM and total PM score, the groups did not differ significantly.
Comparison of PM Between OCD (N1 = 30) and NC (N2 = 30)
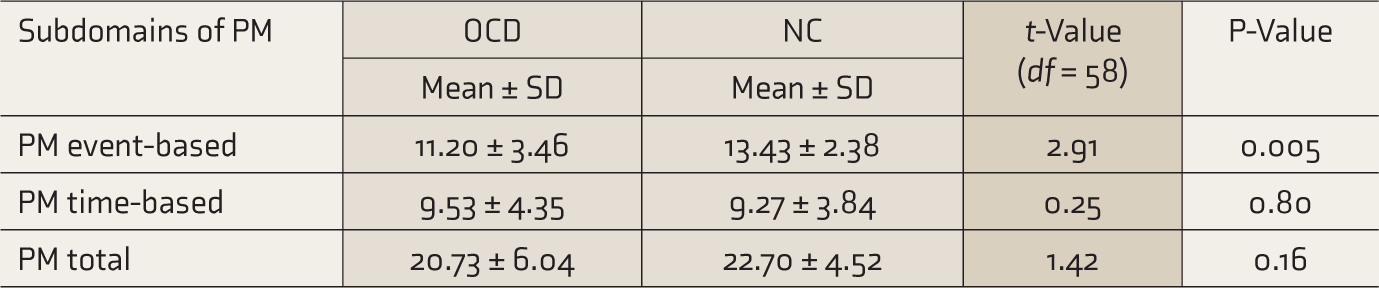
PM, prospective memory; OCD, obsessive-compulsive disorder; NC, normal control; SD, standard deviation.
As age was found to be significantly different between OCD and NC groups ( Table 1 ), a regression analysis was run taking age as a covariate, and the effect of age was found to be nonsignificant across all PM domains, including event-based PM (F = 0.75, P = 0.391), and group difference was almost same (P = 0.004). No significant association was noticed in Pearson correlation scores (r) of the three PM scores with HAMD score (r = –0.01 to 0.10) or with the duration of illness (r = 0.06 to 0.22).
With respect to each of the micro-OCD types—predominantly obsession, predominantly compulsion, and mixed type (Table 3)—no significant difference was observed in any PM tasks.
Comparison Amongst Predominantly Obsessions, Predominantly Compulsions, and Mixed Type on PM Variables

PM, prospective memory; OCD, obsessive-compulsive disorder; SD, standard deviation.
Thirdly, as given in Table 4, the different OCD types—aggression, sexual, symmetry, cleaning, miscellaneous and mixed—were not found to differ with respect to the PM variables (event-based, time-based, and total).
Comparison Amongst the OCD Types (Aggression, Sexual, Symmetry, Cleaning, Miscellaneous, and Mixed) on PM Variables
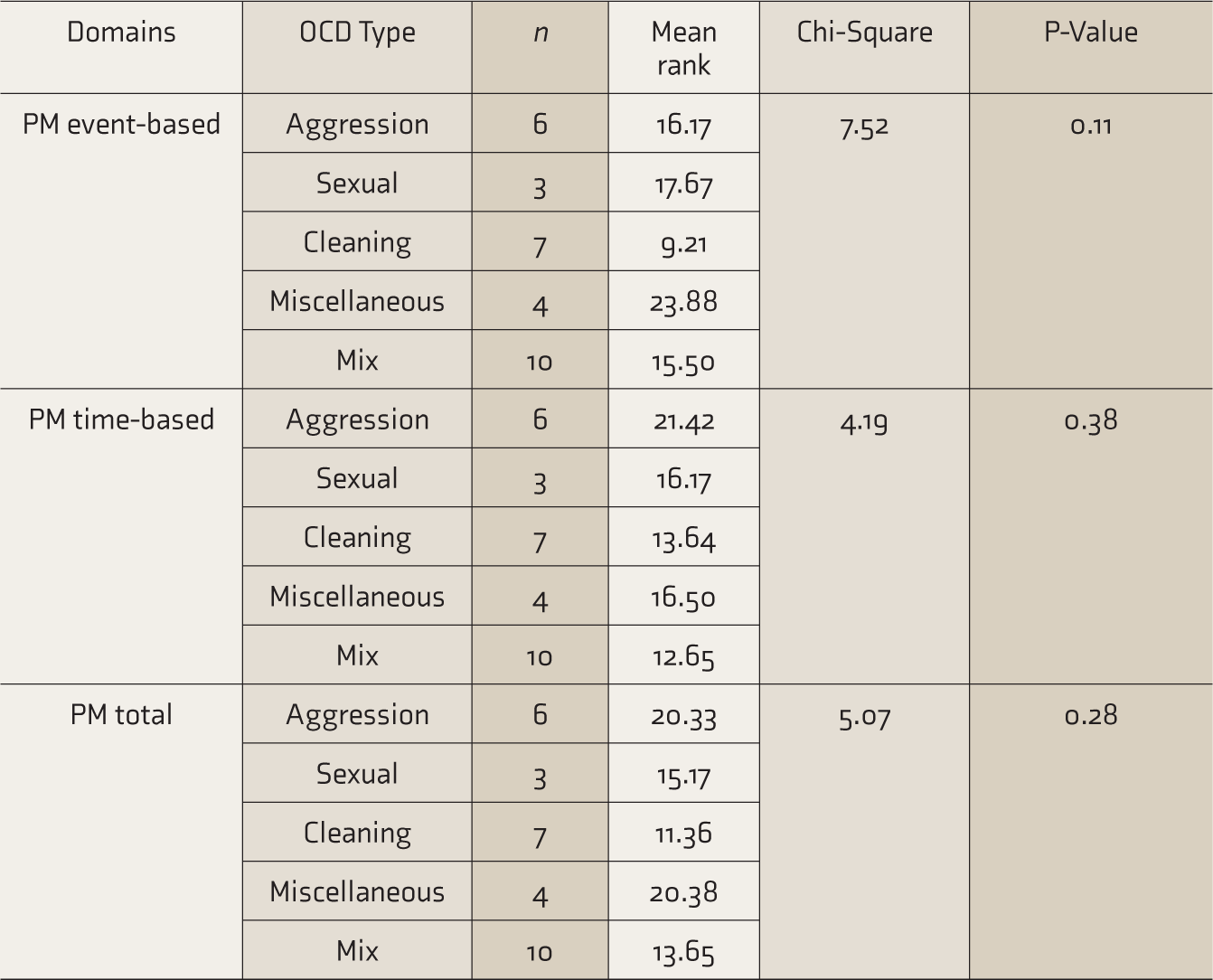
PM, prospective memory; OCD, obsessive-compulsive disorder.
Discussion
Our findings indicate that event-based PM is poor in the OCD group than in the NC. This finding is consistent with previous studies,33–35 which also found poor event-based PM functioning in patients with OCD compared to healthy controls. Graf and Grondin, 33 who measured both time-based and event-based PM, reported that there is a sense of certainty in time-cued tasks or events, as there is a clear sense of dimension (time) during which to anticipate the context in which to perform the intended action. However, in the case of the event-cued task, the occurrence of a cue may be unpredictable. Due to this uncertainty, the compulsion to check increases further, thereby reducing the chance of success in event based tasks. Studies have also indicated the possible role of various cognitive deficits, like in-memory, reality monitoring, and attention, in patients with OCD.36–38
Cognitive self-consciousness (CSC), that is, the tendency to monitor one’s thinking, has been found to be a characteristic of OCD. 39 This chronic monitoring tends to consume the cognitive capacity, and that tends to impede the encoding of information and events and subsequent retrieval, 40 as we can see in Figure 1, which is a figural representation based on our findings, relevant theories, and articles of how PM functioning is hindered in patients with OCD. In addition to this, attentional bias, which has been found to be associated with OCD, as reported by Muller and Roberts 38 and Bar-Haim et al., 41 also contribute to the encoding and retrieval stages. It can be said that when a person with OCD is faced with any input (cue to perform an event in the future) from the environment, he or she is unable to attend to it as there tends to be an additional demand on the attentional capacity because the person is already engaged in self-focused metacognitive processes and gets distracted more toward it rather than the task or input. This probably can be further corroborated by the preparatory attentional and memory processes (PAM) theory. 42 As per the theory, successful event-based PM requires capacity-consuming preparatory processes that are engaged in maintaining a state of readiness to perform a task, which involves some degree of monitoring of the environment for the occurrence of PM target events.
Role of Prospective Memory in Maintenance of Obsessive-Compulsive Disorder
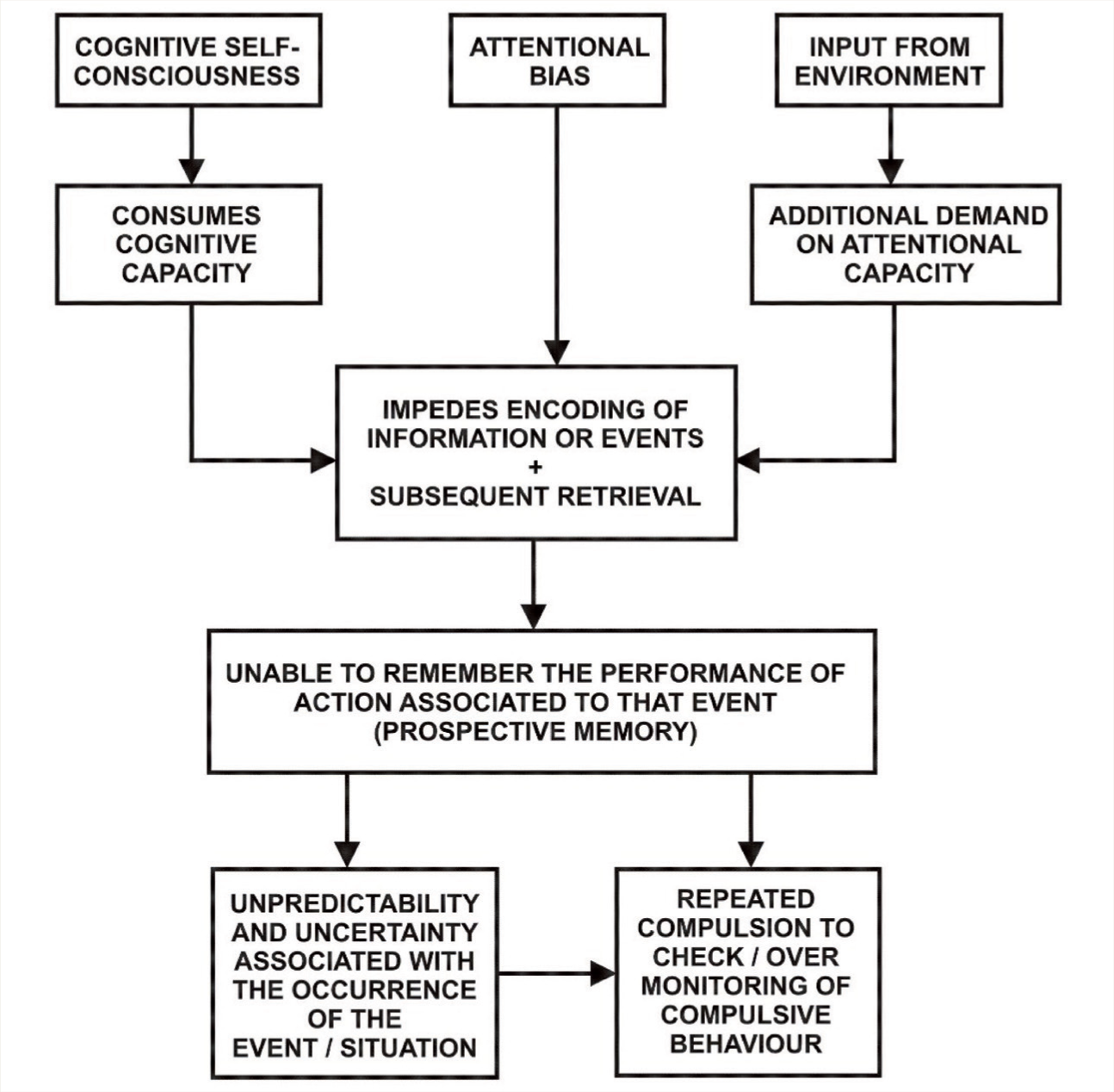
This probably explains the poor encoding of information or event (e.g., the event might be touching the doorknob of the washroom) because of attentional bias and cognitive self-consciousness. This, in turn, creates doubt, and the person is unable to remember the action associated with the event (e.g., the person might not remember whether they have to wash hands when faced with the event of touching the doorknob of the washroom). As a result, the person engages in over-monitoring of the compulsive behavior, which is further exacerbated by the unpredictability and uncertainty associated with the occurrence of the event (i.e., touching the doorknob of the washroom). Thus, it can be said that this can cause significant interference in the person’s daily functioning as the person is left with this doubt and uncertainty, which probably might get in the way of doing regular tasks.
Although we did not find any significant association between comorbid depression and PM performance, studies conducted to assess the effects of depression on PM performance have yielded mixed results.43,44 The neuroanatomical and neurocognitive processes that are affected in depression have also been involved in normal PM functioning. 45 McFarland and Vasterling 46 suggested that although not all studies that have been conducted on depressive clients to assess their PM functioning have revealed deficits in event-based PM, each of them has implicated that individuals with depression have a lesser ability to invest attentional resources in a way that might help in enhancing PM performance. In the current study, we excluded severe comorbid depressive episodes, and it might be interesting to include them in future studies so that more conclusive observations can be made.
With respect to PM variables, no significant difference was found between the three groups—predominantly obsessions, predominantly compulsions, and mixed type ( Table 3 )—which probably indicates that neuropsychological profile with respect to memory is similar in the three groups.
A study indicated that the different dimensions in OCD have distinct yet partially overlapping neurocognitive networks. Moreover, as per the study, the correlation between the neuropsychological profiles and symptom dimensions in OCD is unknown. 47
With respect to the different kinds of obsessions, such as aggression, sexual, symmetry, cleaning, miscellaneous, and mixed types, there was no significant difference among the PM variables, probably indicating that the kind of obsession specifically does not contribute to deficits in PM. Although Cutler and Graf 15 found PM deficits in compulsive checkers, the study was conducted on a sample with subclinical OC symptoms. On the other hand, another study found that the intrusive doubts typical of OCD result from the PM failures that instigate compulsive behaviors like checking. 48
Study Limitations and Future Directions
The present study has some limitations. First, because the sample has been collected from the same place and because of its small size, the generalizability of our findings is limited. Second, the effect of medication was not controlled, which could have affected the neuropsychological findings. Third, the various subtypes of OCD and the content-wise analysis might have high error possibilities because of the smaller sample size. Fourth, sample size estimation was not done. However, in the future, further studies can be conducted to see the difference between the acute and chronic types of the illness with respect to PM functioning and might explore different age groups to see if there is any difference in PM functioning with respect to age in OCD. Lastly, the present study followed ICD-10 for diagnosis where OCD has not been divided into other categories as we find in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; OCD and related disorders). Hence, in the future, we can see how PM might be involved in obsessive-compulsive spectrum disorders. However, the present study used a sample consisting of individuals with clinical symptoms of OCD and performance-based tests exploring PM functioning, which probably increases the generalizability of the findings as most studies have used individuals with subclinical symptoms of OCD.
Conclusion
PM deficits might be significantly associated with OCD, where a deficit in event-based PM has been found. This finding can help explain the psychopathology of this clinical population and can minimize the gap with regard to memory research in OCD. In neurocognitive-based intervention for OCD, the training on improvement of PM functions may be worth incorporating.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this article’s research, authorship, and publication.
Funding
The authors received no financial support for the research, authorship, and publication of this article.