
Abstract
Advances in information technology and the advent of big data (BD) and automated evaluation have changed how we acquire, analyze, and present data in the clinical care continuum. 1 The use of technology is increasingly seen as a solution for addressing the skewed doctor–patient ratio in the field of mental health (MH), albeit with a number of challenges to be addressed. 2 Subsequently, the role of data science and technology in psychiatric practice has been actively explored in recent years. 3 Machine learning (ML) techniques use complex multimodal data in psychiatry for clinical decision-making, otherwise unexplored by psychiatrists.4,5 This technology deployment is shifting the clinical psychiatry practice from theory- and experience-driven to be data- and technology-driven.6–8 The important aspect of this technology-enabled clinical psychiatry is the generation of BD and its analysis and presentation for clinical decision-making.9,10 This paradigm shift, if not accompanied by a corresponding increase in the skills of the psychiatrists to handle new technology, will nullify any advance in the technology. 11
However, BD in psychiatry has been published with less straightforward implications for psychiatrists dealing with the patients directly. BD in MH has been predominantly discussed from a computational and engineering perspective. 12 There are no reviews that broaden the knowledge landscape in clinical psychiatry that underpin the basic science of artificial intelligence (AI) for MH, psychiatry epidemiology, and MH policymaking.
This article aims to create an easy-to- understand functional and process model for psychiatrists with little to no knowledge about BD, ML, and AI. The best way to realize this aim is to synthesize knowledge from the existing literature and personal experiences in dealing with clinical data. Therefore, this article was written to provide familiarity with upcoming concepts and trends in BD, AI, and their potential applications for psychiatrists, without delving into the technical jargon. This viewpoint article will also help psychiatrists collaborate with technology counterparts to translate these ideas and concepts for effective clinical applications. Discussion on complex techniques and technology has been intentionally avoided. Rather, emphasis has been laid upon the actual applications in MH and psychiatry.
Subjects and Methods
Rationale for Choosing the Methodology
Considering the aim of the paper, it was necessary to summarize the existing literature on complex questions using mixed-method reviews.13–15 It is impossible to do a meta-analysis as different studies have used different types of data and ML techniques to address a variety of MH disorders. A systematic review would help gain ideas and concepts but would still lack the knowledge synthesis that can be understood by psychiatrists who have no background in data science or ML. Therefore, a meta-narrative review approach has been used to provide direct, actionable insights to enable the translation of ideas from bench to bedside. It will also help them collaborate with experts/teams of other disciplines. This approach will help offset the methodological weaknesses of various studies and create a comprehensive knowledge of the concepts being studied. 16
Search Strategy and Study Selection
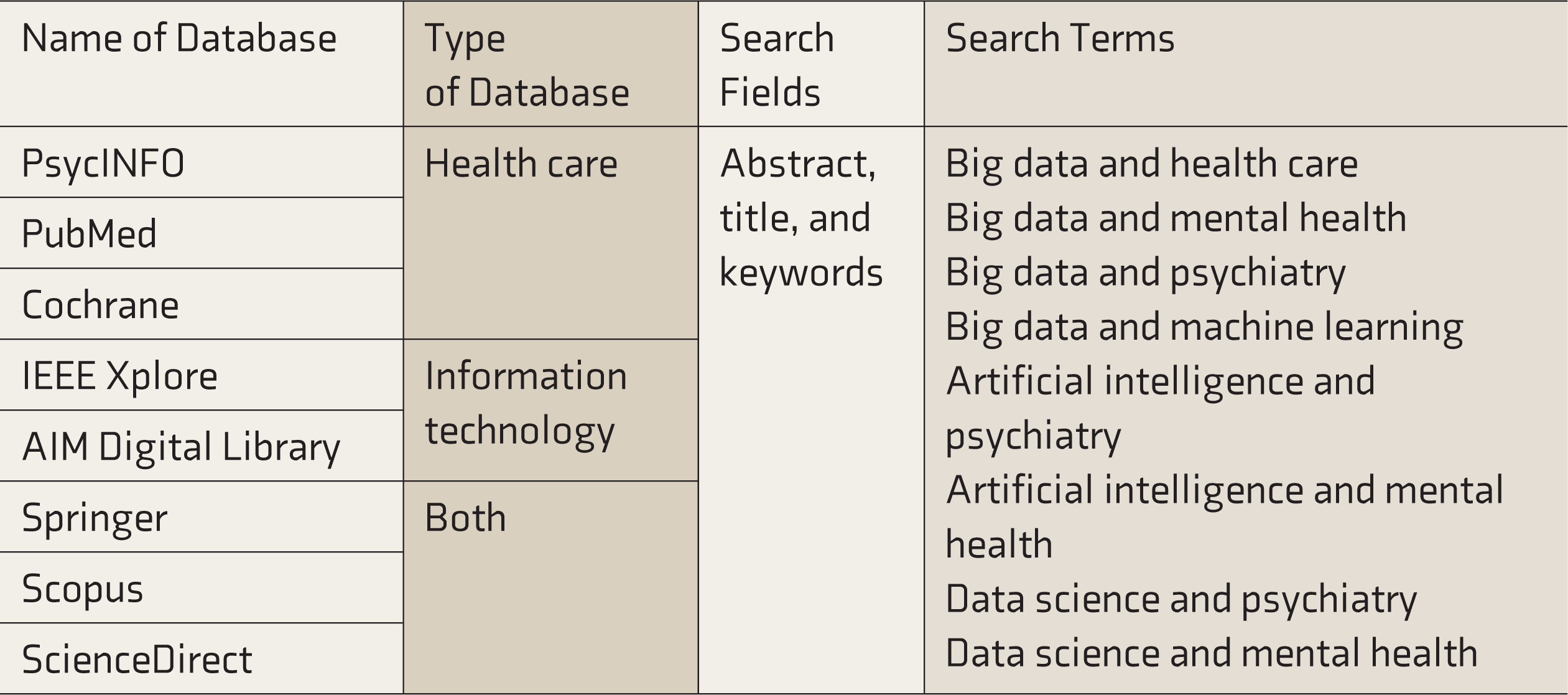
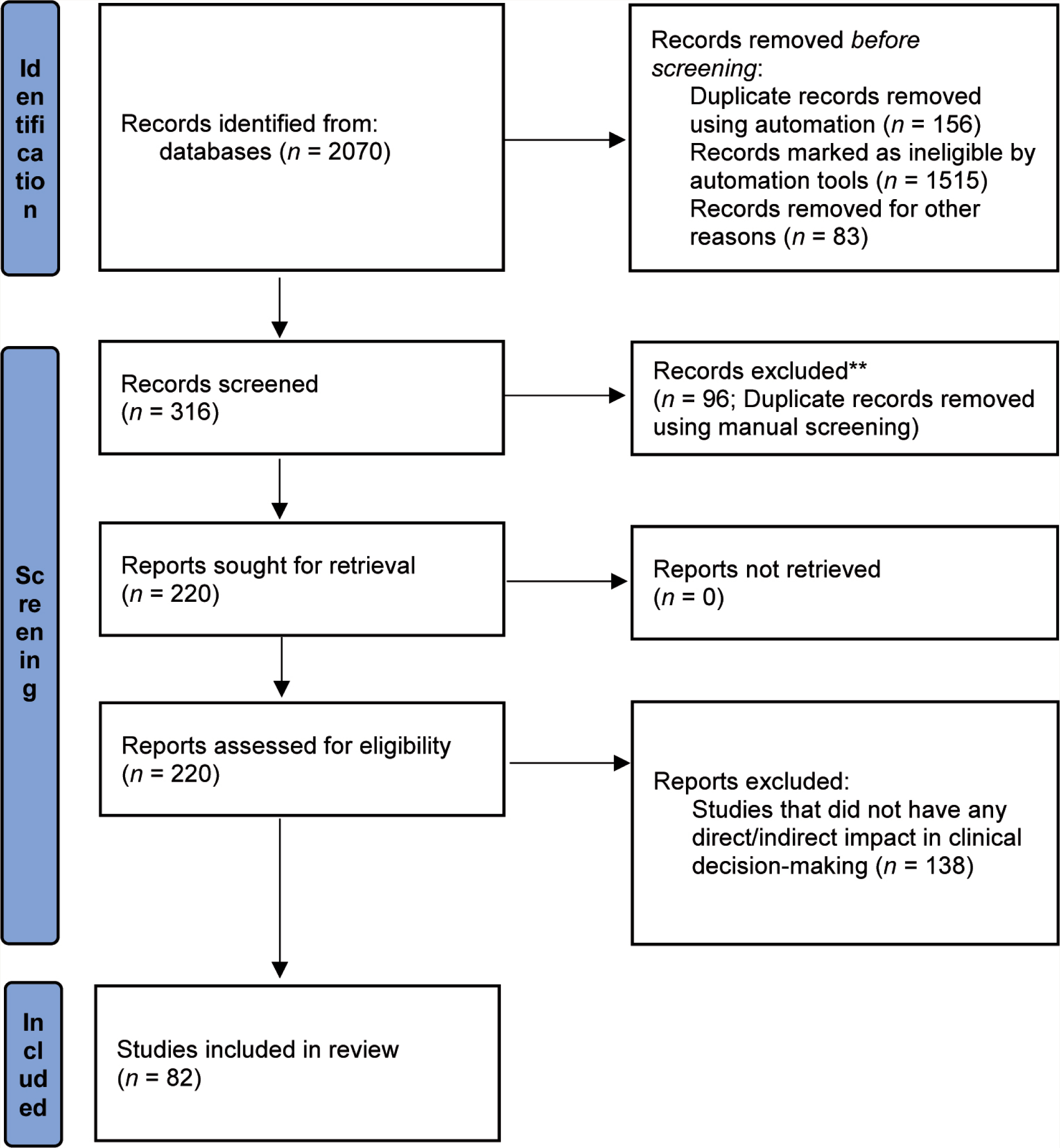
To meet the study’s objectives, several research questions were framed in December 2019 (Box 1). Subsequently, the search strategy (Table 1) and study selection criteria were predefined. The criterion for the study selection was that the information from the studies should have a direct or indirect impact on clinical decision-making. A systematic review was done between January 2020 and June 2021, using the predefined criteria. Articles published in English and peer-reviewed from 2010 to 2021 were selected for review. A title search was done to find the correct papers. Then those screened in the title search were selected for reading the abstracts. Those that fulfilled the eligibility criteria were selected for reading the entire article. The papers were then studied to extract ideas. The articles provide insight on BD in psychiatry, ML in psychiatry, and applications of ML/AI in MH (according to the World Health Organization definition of MH).
Research Questions
1. What is BD in MH and psychiatry?
2. What are the different sources, types, varieties, and methods of acquiring BD in psychiatry?
3. What are the characteristics of this data?
4. How to leverage the potential of BD?
5. How to analyze this data?
6. What is the role of ML and AI in analyzing this data?
7. How can a clinical psychiatrist use BD and related technology for delivering primary care?
8. What are the various applications of AI and BD in clinical care?
Search Strategy
Knowledge Extraction, Analysis, and Synthesis
Initially, three broad themes were framed (data in MH/psychiatry, analysis, and applications in MH/psychiatry). Full papers were read thoroughly, and knowledge was extracted and classified under these themes. Three guiding questions in the analysis of the information extracted were; (a) Is this information relevant for clinical decision making (directly or indirectly)? (b) What is the straightforward implication of this knowledge in various applications of AI/ML in MH and psychiatry, and how do different components interact with each other in the medical-technology spectrum? (c) How can a clinician use this information to contribute to AI/ML in MH and psychiatry?
Within each theme, the content was explored using focused coding and the constant comparative method. Codes and categories were identified. Irrelevant codes were then excluded from the analysis. 17 The information was analyzed using meta-ethnography techniques, and an interpretative qualitative synthesis was done using the best-fit framework synthesis approach. 18 Figure 1 shows the summary of the method. 19 Subsequently, functional and process models from a clinical psychiatry perspective were developed. Realist and meta-narrative evidence syntheses (RAMESES) method for meta-narrative reviews has been followed in reporting this study.
Themes, Categories, and Nodes from the Analysis
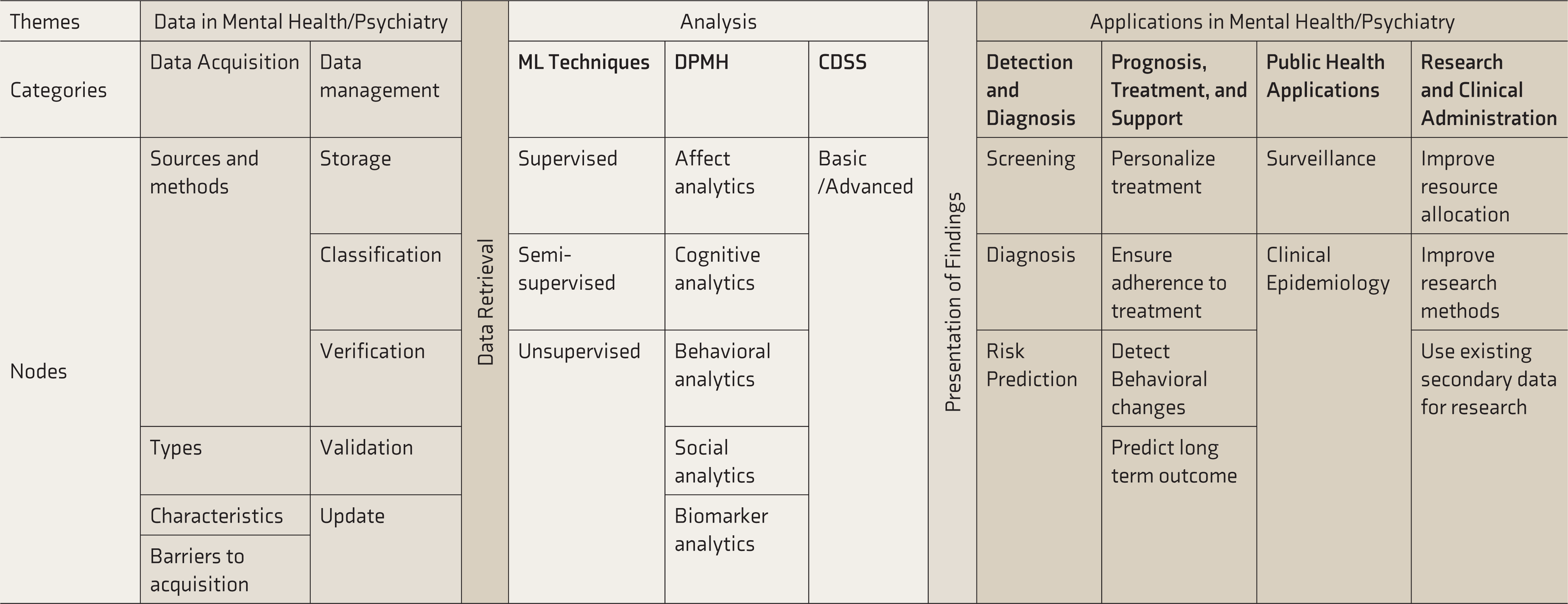
CDSS, clinical decision support system; DPMH, digital phenotyping in mental health.
Summary of the Research Process
Results of the Review
Analysis of the content revealed codes and categories summarized in Table 2. The findings and salient features of the functional and process model are discussed in detail under discussion.
Discussion
Some reviews and studies dealt with the technical aspects of AI in psychiatry and MH. The studies detailed the design of the algorithm, the architecture required to implement them, and the function of the algorithm.20,21 However, when a psychiatrist tries to understand this concept, it becomes overwhelming as these concepts are written from a nonclinical perspective. 22 The need for describing these concepts from a clinical perspective is essential to ensure that psychiatrists can collaborate with technology experts in using AI to solve common problems in clinical practice. Additionally, this paper will serve as a starting point for psychiatrists trying to get an overview of data science and AI in MH without a technical conundrum.
Therefore, the discussion section has been divided into two parts.
Part A: A functional model that discusses the individual components of the entire bench-to-bedside pathway of data science and AI in psychiatry
Part B: A process model on how these components interact and what is expected out of the psychiatrist, the essential knowledge required, and how to enable meaningful innovation in psychiatry
Part A: Functional Model
The functional model was derived from breaking the complex concepts into an easy-to-understand framework for direct clinical implications in psychiatry. Therefore, only insights that are relevant to clinical psychiatry have been discussed. Hence, concepts have been populated and discussed without definitions or detailed descriptions. Most of the insights apply to the entire health care sector, although specific implications in psychiatry have been discussed. Figure 2 shows the functional model from a clinical psychiatry perspective. The ultimate beneficiary is the patient, who is also the model’s starting point.
Functional Model From a Clinical Psychiatry Perspective

This section is further organized under the major themes of the review; data in MH/psychiatry, analysis, and applications in MH/psychiatry.
Data in Mental Health/Psychiatry
The major headings in this subsection are data acquisition (where, what, and how data is collected), data management (when, where, and how data is kept), and data retrieval.
Data Acquisition23–25
Data acquisition can be understood under four common headings:
Source and Methods of Data Collection
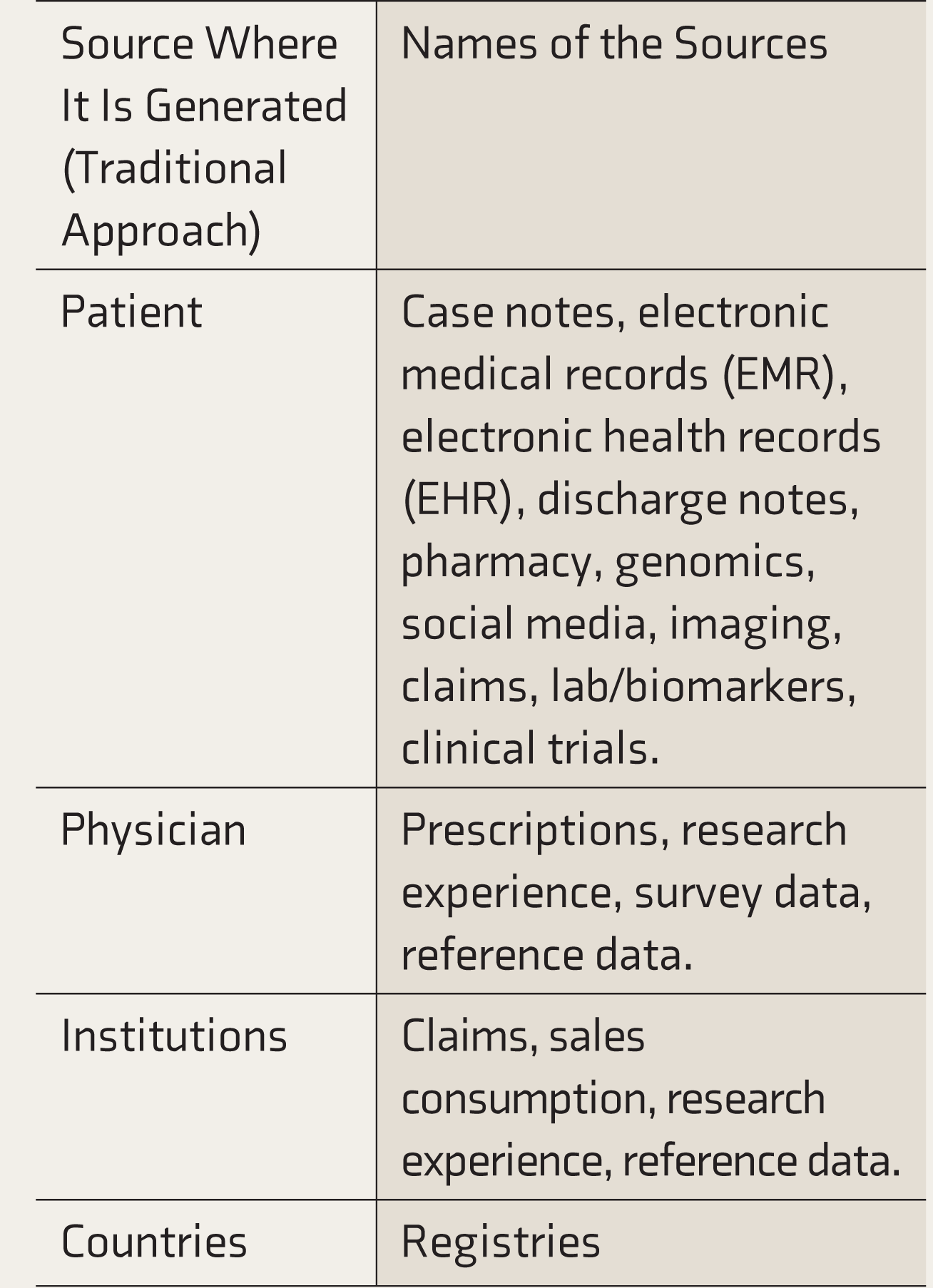
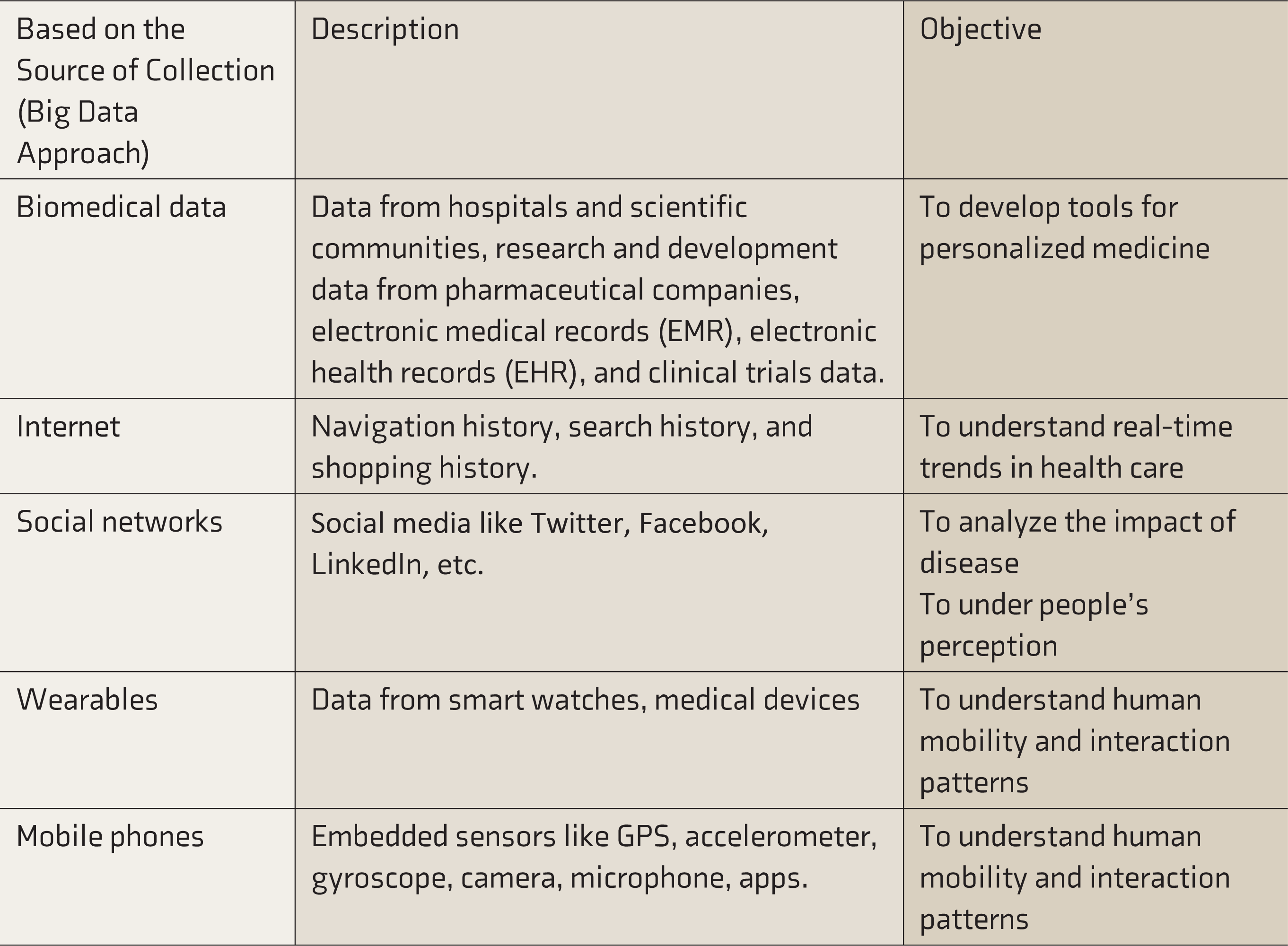
It is essential to understand how and from where the data has been generated. There are two ways to view this. The traditional way of seeing this is to identify who generates this data (Table 3). The other way is the big data perspective based on how and where this data is collected from (Table 4). There will be considerable overlap between these two approaches and between categories within these approaches.
Sources and Methods of Data Collection (Traditional Perspective)
Sources and Methods of Data Collection (Big Data Perspective)
Types of Clinical Data in Mental Health
The data is any of the following types: tabular data, images, voices, speech, video, text, and time series.
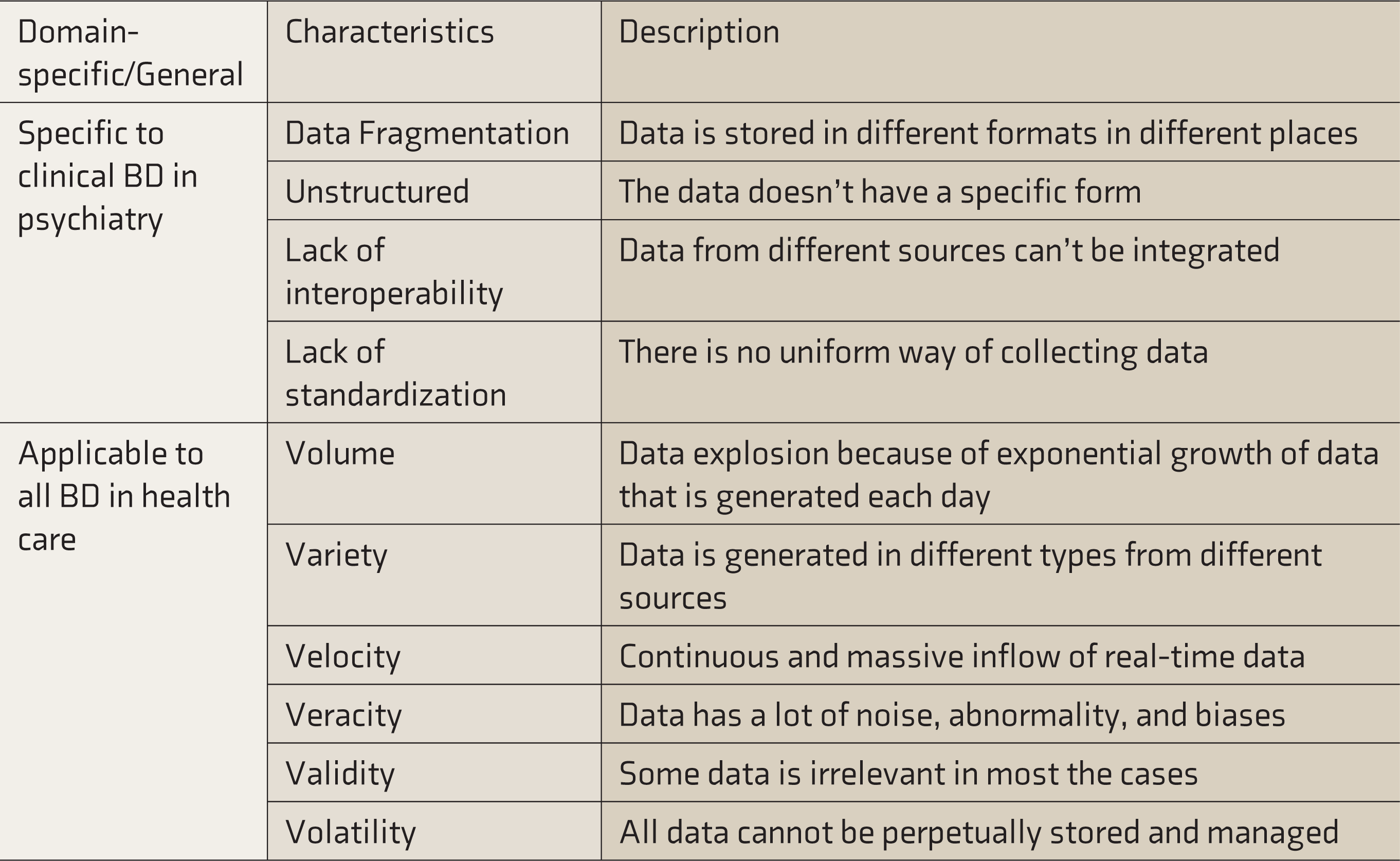
Characteristics of Data in Psychiatry/MH
Please see Table 5.
Characteristics of BD in Mental Health/Psychiatry
Barriers to Efficient Data Acquisition in Clinical Psychiatry
The most common barriers to data acquisition are
25
:
Technical barriers (lack of interoperability). Political barriers (lack of effective data-sharing policies). Ethical barriers (lack of consensus on privacy and confidentiality). Administrative barriers (inadequate human resources to handle clinical data).
Data Management and Retrieval
This is purely a nonclinical aspect of BD, consisting of verification, validation, storage, classification, update, standardization, and review. The process of extracting data from a database for analysis or visualization is called retrieval. This is beyond the scope of this paper to discuss in detail. However, psychiatrists need to be familiar with the vocabulary, terminologies, and various data standards in health care. 26
BD Analysis in Psychiatry 27
Machine Learning Techniques (ML Techniques)
ML techniques can be supervised, semi-supervised, or unsupervised. There are many reviews that detail ML techniques in MH. An important concept to remember is that ML techniques are a way to use computers to analyze BD. This vast domain is not for psychiatrists, although basic knowledge is necessary to collaborate with ML engineers. Each technique has a unique purpose and function. The choice of ML technique depends on the need, available data, and available resources. At any point, the choice of an ML technique is always taken by the nonclinical counterpart; therefore, a general understanding of the concept is enough.
Digital Phenotyping of MH (DPMH)28,29
With such voluminous data and multiple correlations with different variables that can be spurious at times, it is essential to identify those data points that are clinically significant and serve as a surrogate marker for any underlying psychiatric disorder. Also, it is essential to find variables that represent many other variables or variables with higher weightage so that the less significant variables can be ignored from the overall decision-making model. The process of extracting clinically significant digital biomarkers that provide meaningful insight for decision-making in psychiatry is called as digital phenotyping of MH (DPMH). It is of the following types;
Affect recognition (emotion recognition and sentiment analysis) Cognitive analytics (acoustic analysis, linguistic analysis, and emotion processing) Behavioral anomaly detection (sleep monitoring, substance abuse, suicide, and eating disorder) Social analytics (social influence, social dynamics, and social participation) Biomarker analytics (genome and neurological imaging)
Clinical Decision Support Systems (CDSS) 30
Clinical decision support systems (CDSS) are computerized and noncomputerized tools and interventions that aid clinical decision-making for care, support, and treatment. Depending on the complexity of the problem to which support is provided, CDSS can be basic (simple alerts for taking drugs, prompts for better data collection in health management information systems (HMIS), etc.) or advanced (checks for drug-disease interactions, providing treatment recommendations, etc.). Basic CDSS is part of the regular clinical care continuum; however, advanced CDSS is still a theory.
Applications in Mental Health/Psychiatry 31
Data science and AI in MH/psychiatry can be used for the following:
Detection and diagnosis of clinical conditions (screening, diagnosis, and risk prediction). Prognosis, treatment, and support (personalizing treatment, ensuring adherence to treatment, detecting behavioral changes, and predicting long-term outcome). Public health applications (surveillance and clinical epidemiology). Research and clinical administration (improving resource allocation and research methods, using existing secondary data for research).
Part B: A Process Model with Implications in Clinical Psychiatry
The challenge with translational research is that the knowledge of the application of concepts is different from the actual understanding of the concepts. This section is drafted considering that psychiatrists have little to no understanding of data science and AI concepts. However, this should not limit them in providing meaningful contributions to technology experts who require psychiatrists’ input and validation. Therefore, this section deals with a simple process model that any psychiatrist is likely to encounter when dealing with data science and AI in MH. The process can be broadly divided into three phases (Figure 3).
Process Model From a Clinical Psychiatry Perspective

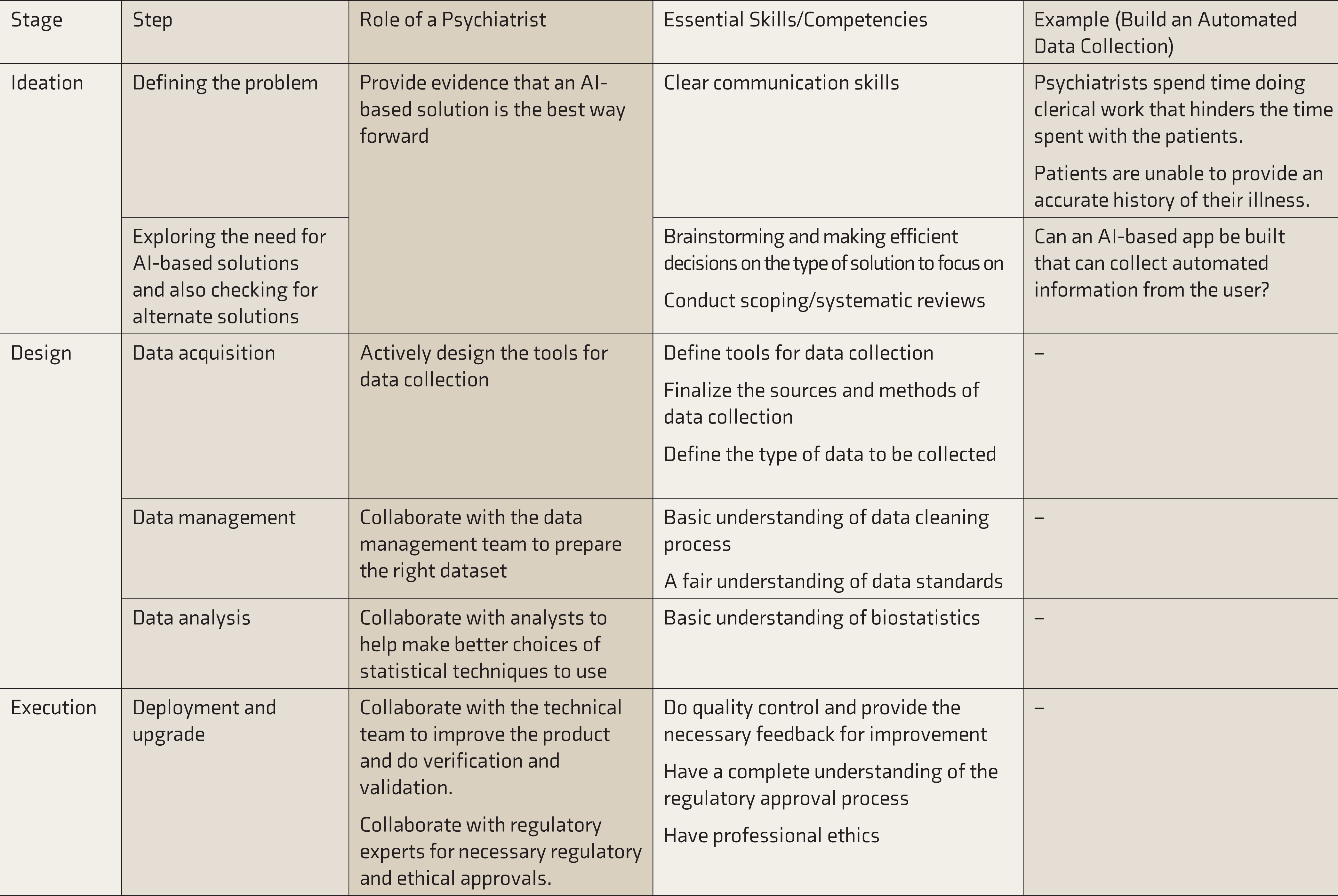
Ideation
This is the most important stage in any innovation or invention. Technology experts lack this insight and rely on psychiatrists to look for gaps where technology can play an efficient role. There is a need to identify a problem that needs a solution and define the problem statement in terms that technology experts can understand. Also, it is essential to determine if an AI-based solution is necessary or will it be another tool that will soon be forgotten and lost.
Design
The design phase is purely for the technology experts to work on, although the choice of tools for data collection, sources, and methods are largely determined by the psychiatrist in line with the clinical practice requirements. This phase is where active collaboration takes place between various stakeholders. Hence, holistic knowledge of various stakeholders and activities is necessary.
Execution
This phase is important for a psychiatrist only from the perspective of verification and clinical validation of the technology and ensuring that every procedure is in accordance with good clinical practices.
Table 6 summarizes the process model with examples, along with the role and essential skills for a psychiatrist. 32
Role of a Psychiatrist and Essential Skills and Competencies
Limitations of the Study
The paper is limited by a single author perspective. However, it is challenging to find psychiatrists who can understand the jargon in engineering and simplify the article. Therefore, a single author perspective is good to start with, considering the nascent stage of clinical data science and clinical AI in MH and psychiatry. The paper doesn’t delve in-depth into the data management and ML concepts. There are a lot of studies that discuss them in detail, and there is a necessity for consolidating the knowledge into understandable domains.
Conclusion
Psychiatrists have a huge responsibility in the ideation and execution of AI-based applications. Hence, it is necessary to understand the important concepts of data science, digital phenotyping, CDSS, and analytics from the process model perspective to make it easier for psychiatrists to understand and collaborate with different stakeholders wherever necessary. Future studies should focus on maintaining ethics, privacy, security, and confidentiality of the data collected through these novel modes of technology.
Supplemental Material
The Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.