
Abstract

To the Editor,
The gradually narrowing gender gap in substance use disorders (SUDs) has led researchers to examine gender differences in SUDs. 1 Very few studies have examined gender differences in substance use in India.2, 3 Hence, our study aimed to compare demographic and clinical characteristics and hospital visits for follow-up treatment between women and matched men visiting the drug dependence treatment center of our hospital from January 2018 to December 2020.
The study was conducted at the drug dependence treatment center of a psychiatric hospital located in the rural outskirts of a state capital in eastern India. After approval from the Institute Ethics Committee, a list of case record file (CRF) numbers of all women who had visited and been registered under the center between January 2018 and December 2020 was made. As the number of men was greater compared to women, CRFs of all male patients who were matched for the period of hospital visit with each female patient were retrieved and reviewed. Among them, one male patient matched with age of a corresponding female patient was selected. Thus, each male patient in the control group was matched for (a) period of a hospital visit and (b) age with a female patient in the women group, on a case-to-case basis. A predesigned semistructured data sheet was used to collect data. It was based on the demographic information collected by the center for all the treatment-seeking individuals. After initial workup by junior residents, assessment and diagnosis were done by psychiatrists according to the International Classification of Disease, 10th version (ICD-10)—clinical description and diagnostic guideline. 4 Any syndromal psychiatric comorbidity was also diagnosed according to ICD-10—clinical description and diagnostic guideline. Substance use was defined as current use, within the past 30 days, of any substance listed under “Mental and behavioral disorder due to psychoactive substances use” in ICD-10. For patients using multiple substances, the primary substance was determined by the duration of the substance use and the reason of the visit at the OPD. Medical comorbidities were recorded based on the past treatment history, related documents, workups, and investigations at our center. Data were analyzed by IBM SPSS Statistics 25.0 for Windows. 5
A total of 39 women visited our hospital’s drug dependence treatment center in the study period. Their mean (SD) age was 39.21 (11.70) years (median = 43 years; interquartile range [IQR] = 18). Sociodemographic characteristics including education (uneducated, up to tenth, up to intermediate, or up to graduation vs. postgraduation or above; Fisher’s exact test = 3.88, P = 0.42), habitat (urban or semiurban or rural; Fisher’s exact test = 1.10, P = 0.61), marital status (married or unmarried/single or separated/divorced; Fisher’s exact test = 4.15, P = 0.14), family types (joint or nuclear; χ 2 = 0.06, df = 1, P = 1.00), and monthly family income (Mann–Whitney U = 624.50, Z = –1.36, P = 0.17) were statistically not significantly different from men. The mean monthly family income among women was INR 12,717.95 (7650.07; median INR 10,000.00; IQR = 12,000). Most women were homemakers (n = 31), whereas more men were employed as professionals (χ 2 = 49.62, df = 6, P < 0.001). History of forensic (Yate’s continuity correction = 1.69, df = 1, P = 0.19), psychological (χ 2 = 0.05, df = 1, P >0.99), and physical consequences (χ 2 = 2.16, df = 1, P = 0.22) was statistically not significantly different from men. Family history of substance use (χ 2 = 0.46, df = 1, P = 0.64) and premorbid personality (well-adjusted or not well-adjusted or not available; Fisher’s exact test = 0.65, P = 0.90) were statistically not significantly different as well. Table 1 compares other clinical and treatment-seeking behavior between women and men.
Although a recent review 6 reported substance use to cause more effect on the occupation of men than women, significant difference in the occupation between the two sexes was observed in our study where more men were employed as professionals, while women were homemakers. The sexes did not differ in marital status in our study, whereas a recent review found more women to be separated or divorced than men. 6 Women had significantly later age of onset of substance use and significantly shorter duration of substance use, thereby indicating a “telescopic” course of illness. 7 Following alcohol, significantly more women used tobacco as the primary substance, while more men used cannabis as the same. Alcohol was the most commonly used substance in our study, consistent with a recently concluded epidemiological study from India. 8 But that study did not include tobacco. Another epidemiological study only on tobacco use found that 14.2% of women in India use tobacco. 9 Two hospital-based studies in India on women with SUD found opioids and tobacco to be the most commonly used substances.2, 3 Thus, the use of tobacco as a primary substance by significantly more women than men in our study agrees with recent evidence. The sex difference in psychiatric comorbidities found in our study is consistent with a recent review. 1 There was significantly lesser number of follow-up visits and a shorter duration of follow-up period among women. Reviews have shown that this could signal lower treatment retention and a poorer prognosis for SUD. 10 Levels of motivation were more favorable among women than men in our study. Earlier studies have shown conflicting results for motivation between the two sexes. 11 Several treatment barriers specific for women, including increased stigma, economic constraints, family responsibilities, unemployment, and social disapproval, less family and friends support, and fear of losing custody of a child, have been discussed in the literature.6, 12
Comparison Between Women and Men (N = 78)
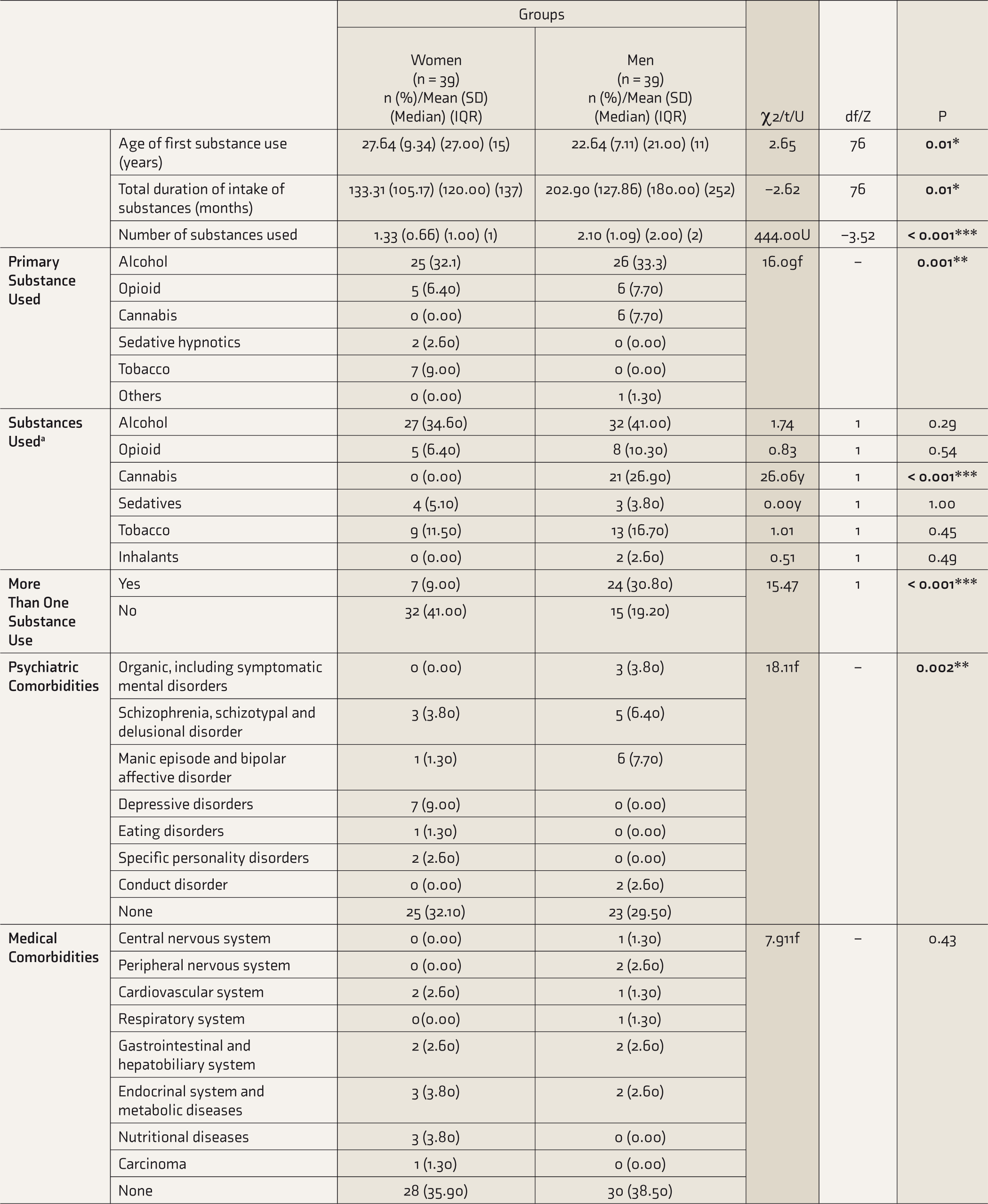
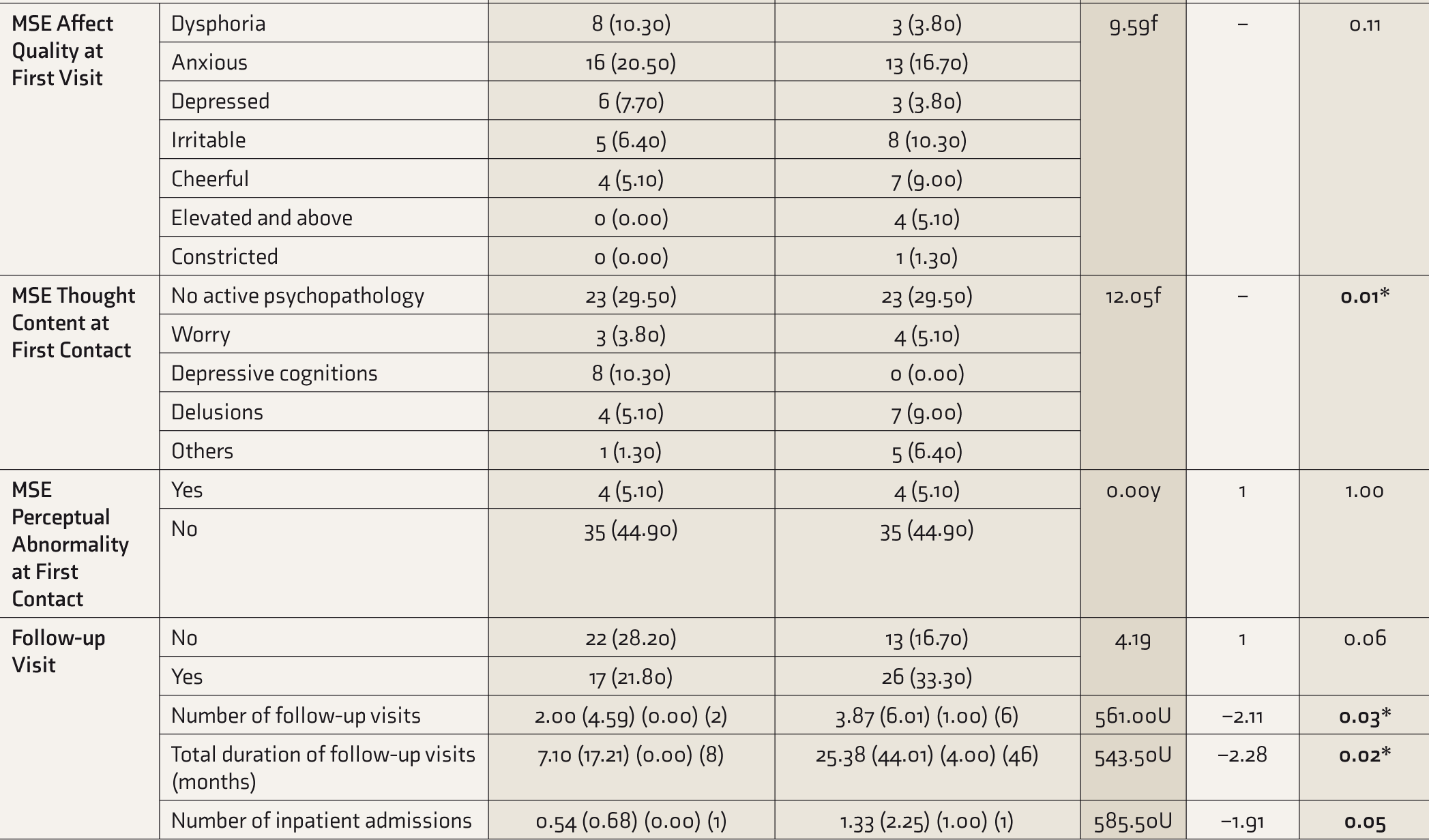
UMann–Whitney U; MSE, mental status examination; atotal number and percentage are more than N and 100 because of multiple substances used by patients; fFisher’s exact test; y Yate’s continuity correction; df, degree of freedom; IQR, interquartile range.
Our study adds to the sparse literature on women with SUD visiting a specialized drug dependence treatment center in developing countries like India and found distinct demographic and clinical differences from men. Future multicentric prospective studies with larger sample sizes and qualitative design would push the current evidence forward.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.